Rates of infection with other pathogens after a +ve #COVID test versus a neg test - more brilliant work from @zalaly and team. COVID causes immune dysregulation and ⬆️risk of other infections. https://t.co/yIZ9LvD2NF
My cancer docs are celebrating all the new drugs coming into the armamentarium, but they say in 2-6 years there’s going to be a lag because do much research has been stopped
https://t.co/AvEyhU818G via @NYTimes
Police removed diabetes scientists from the convention center here in New Orleans today after they attempted to pass out copies of an editorial from a peer-reviewed scientific journal (impact factor = 16.6) that was critical of NIH.
New data from David Ho's lab showing that while adults & kids have ~equal antibody responses to XFG & NB.1.8.1, children have essentially no neutralizing antibodies to BA.3.2.
This seems to largely solve the BA.3.2 + kids mystery. 1/14
I talked to a journalist about the return of New World screwworm last spring. There was time to get ahead of this — but apparently no institutional or political will
For 40 years, "high-risk breast cancer" meant chemo for everyone who got that label.
A trial of 4,429 women just broke that rule.
They took the tumor, ran a 50-gene test (Prosigna), and let the biology decide who actually needed chemo. The women the test called low-risk skipped it entirely, hormone pills only.
Five years later: 93.6% alive and cancer-free on pills alone. 94.8% on chemo. Basically the same number.
68% of these "high-risk" women could have skipped chemo and never lost a thing.
That's hair, nausea, nerve damage, and months of your life. Gone because a gene test read the tumor, not because a protocol read the chart.
It was presented at ASCO last week, the biggest cancer meeting of the year.
If you have ER-positive breast cancer, or know someone who does, ask your oncologist about Prosigna by name before the next treatment call.
By the time a Parkinson's tremor shows up, the disease has been running for a decade and most of the dopamine cells are already gone.
We can now see it coming. Six ways, ordered by how early they catch it:
1. Your sense of smell. Losing it is one of the first signs, often 10 years before a tremor.
2. Acting out your dreams. This sleep disorder turns into Parkinson's or dementia in 73% of people within 12 years.
3. Your smartwatch. One week of wrist movement flagged future Parkinson's up to 7 years early, and beat genetics and blood tests doing it. (An early warning, not a diagnosis.)
4. Your eye doctor. Routine retinal scans showed thinning about 7 years before diagnosis.
5. A skin punch you can order in the US today. It finds the Parkinson's protein in your skin nerves in 92.7% of patients, with almost no false alarms.
6. A spinal-fluid test. It catches about 99% of classic Parkinson's, and turns positive in people who still feel fine.
The shaking is the last thing Parkinson's does, not the first. Which of these would you want to know about yourself?
An experimental vaccine from Moderna shows promise in keeping deadly skin cancer from returning for years, according to new clinical trial results. https://t.co/UCVfhRE8na
The main claim — that the US recommends that all kids are vaccinated against many more pathogens than children in peer nations is not true. I did an analysis of 37 other countries. The US is not an outlier. https://t.co/xIxtTJCJAR
One month has passed without a reported death from the hantavirus outbreak on the MV Hondius, with confirmed cases holding steady at 13. The situation is stable, and the global risk remains low. WHO will continue close coordination with affected governments through the completion of the quarantine period for all passengers and crew.
You learned in school that mitochondria are the powerhouse of the cell, locked inside it for life. That’s wrong.
Cells pass mitochondria to each other. New work in @Cell_Metabolism ties that swap to how cancer cells stay alive and how damaged tissue stokes inflammation.
Here’s why it matters beyond cancer. The same organelle trade is showing up in aging research, where failing mitochondria are a hallmark of aging.
One currency, moving between cells, sits underneath two of the hardest problems in medicine.
A piece in JAMA (5/20) proposed treating primary care as a public utility: pool the money public & private payers spend on primary care, have the state administer it, and pay practices directly, vs. through separate insurance contracts. Could this work?
https://t.co/FugPCg4mgZ
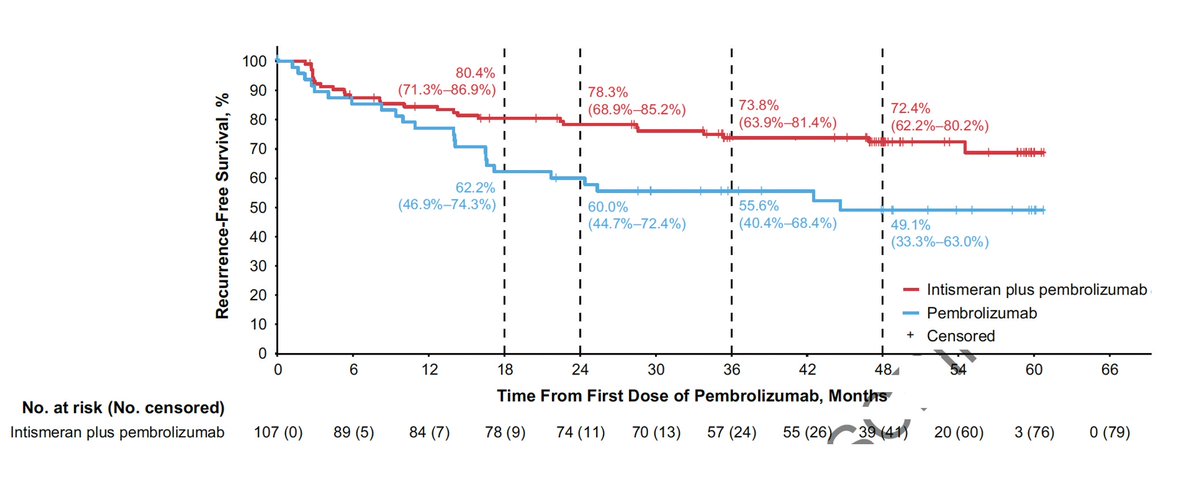
Another major advance vs cancer! @ASCO#ASCO26
Personalized neoantigen mRNA vaccine 5 year follow-up vs metastatic melanoma reduced recurrence and death by 49% (on top of Keytruda)
https://t.co/NadITTYIT2
One year ago, I gave this interview to CNN about leaving the U.S. because of cuts to scientific funding and because immigrant scientists like me no longer felt welcome there.
What followed was a difficult year. I applied for dozens of positions, received dozens of rejections, and eventually relocated to Germany. Even now, I still mourn some of those opportunities that never materialized. That's a normal part of the process.
At the time, there was widespread concern that American scientists would flood an already saturated European academic job market. That never happened, and likely never will. The reality is that opportunities outside the U.S. are far scarcer than many people realize.
Many of the initiatives and campaigns that promised a "safe haven" for scientists leaving the U.S turned out to be something else entirely. In practice, most were used to attract European researchers back from American institutions, while others functioned largely as political or media statements. Very few created meaningful opportunities for the thousands of scientists, immigrants and U.S. citizens, whose careers were disrupted by funding cuts and instability.
The hard truth is that most scientists affected by these policies remain trapped. They cannot easily stay, but they cannot easily leave either. Meanwhile, the situation continues to deteriorate.
I wish more institutions and governments expressing concern about the U.S. scientific exodus would move beyond press releases and empty gestures and invest in real pathways for talented researchers to rebuild their careers elsewhere.
#BrainDrain
https://t.co/r6CycmGWfB
US hospitals, 457,950 COVID patients.
AI found long COVID in 16.28%, about 1 in 6, with 89.31% developing chronic conditions.
Coding misses over half of cases.
https://t.co/prqZnFk72R
Not all organs respond equally to #COVID infection. DISCO-seq, a new technique led by my talented friend @HarsharanBhatia, combines 3D imaging and single-cell analysis to map Spike Protein tropism and found mostly in the liver, lungs, intestine & kidneys. https://t.co/9dA0axeUbU
#LongCovid has not decreased from 2020-2024.
Prevalence is 13-23% of US population, increasing 0.4%-1.5% every 3 months.
Incidence was 10-29%, but began increasing in 2023.
"These findings indicate an accumulating rather than resolving disease burden." https://t.co/SZGm2NFkg0
In an Ebola outbreak, the virus itself isn’t the only killer. When communities fear that health facilities or services are disrupted, deeper challenges arise. In the 2014–2016 Ebola outbreak, more people died from malaria because the health system shut down than from Ebola itself. That's what's at stake. The goal isn't just stopping Ebola—it’s also keeping health systems from collapsing around it.
Five cancers that used to be death sentences. Pancreatic. Glioblastoma. Triple-negative breast. Renal. Melanoma. The median survival for metastatic pancreatic cancer is still 6 months. Glioblastoma, 15 months.
Now personalized mRNA vaccines are producing complete remissions in some of these patients. Not responses. Remissions.
BioNTech’s pancreatic cancer vaccine has 6-year follow-up data. 8 of 16 patients who mounted an immune response are still alive. For a cancer that kills 95% of patients within 5 years, that's incredible.
Topol’s pyramid here maps the trajectory. From broad checkpoint inhibitors at the base to personalized neoantigen vaccines at the peak. The technology is climbing.