Outcomes of Y90-radioembolization as downstaging to liver transplantation HCC and tumoral portal vein thrombosis
@HEP_Journal
https://t.co/RcHl1K7vxQ
👉25% sustained downstaging after TARE
👉15% eventually LTx with good outcome
🧐Downstaging is feasible in MVI pts
@myESMO@ILCAnews@EASLnews
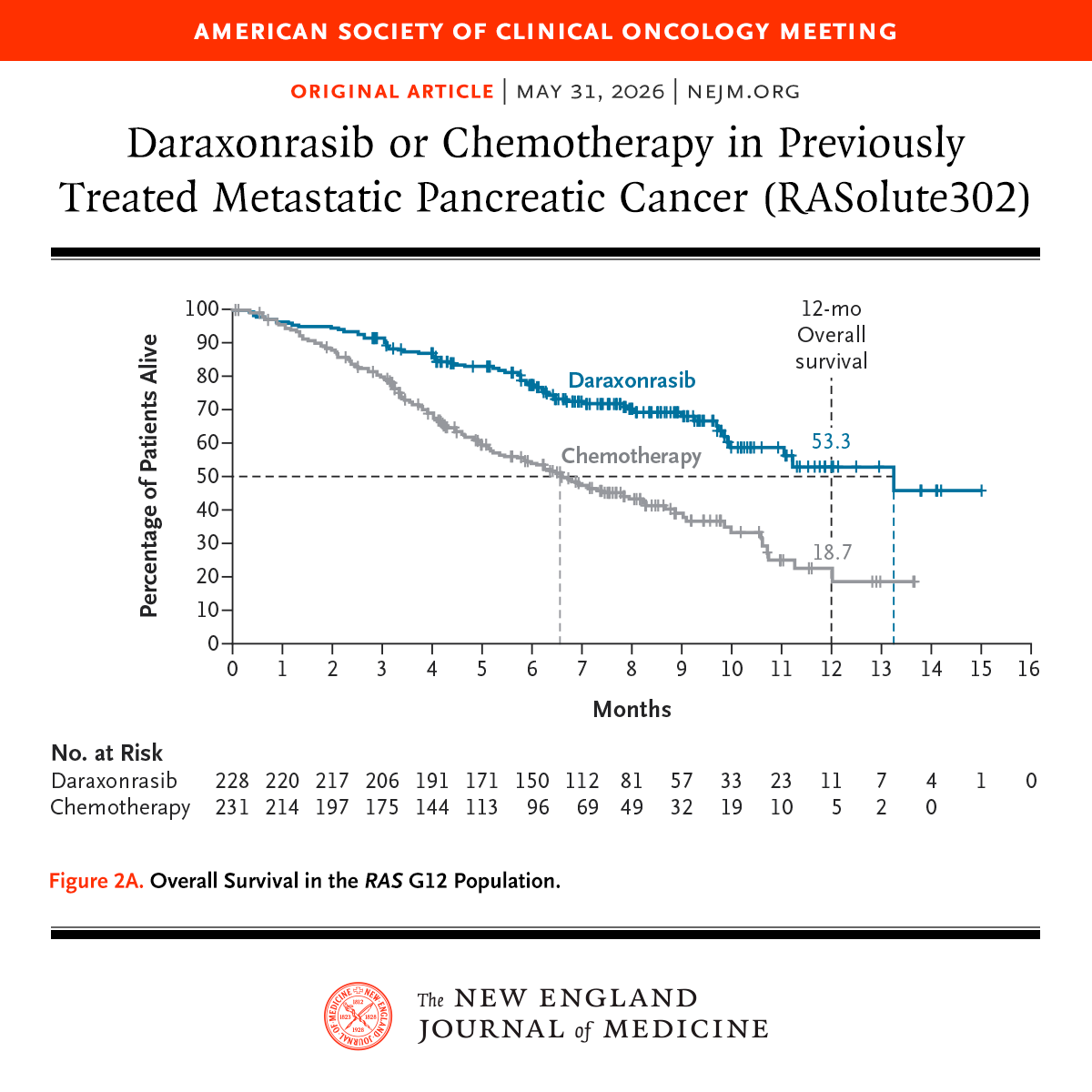
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
🧬 FAPI PET is redefining the future of cancer imaging.
Unlike FDG PET, which visualizes tumor glucose metabolism, FAPI PET maps the tumor microenvironment — especially cancer-associated fibroblasts (CAFs) and stromal activity.
Why this matters clinically 👇
✅ Better tumor-to-background contrast
✅ Superior detection of peritoneal disease
✅ Improved visualization of desmoplastic tumors
✅ Better assessment of low-FDG tumors
✅ Potential role in radiotherapy contouring
✅ Emerging theranostic applications (^177Lu-FAPI)
The shift in oncology imaging is happening:
➡️ From “tumor metabolism imaging”
➡️ To “tumor ecosystem imaging”
#FAPIPET #PETCT #NuclearMedicine #MedicalOncology #CancerImaging #Radiology #Oncology #PrecisionOncology #Theranostics #RadiationOncology #PancreaticCancer #GastricCancer #BreastCancer #HeadAndNeckCancer #CancerResearch #DrRupamManna #CancerConceptsExplained
🔬 MSI-High / dMMR Rectal Cancer After Neoadjuvant Immunotherapy with Complete Response: What Next?
In the rapidly evolving landscape of precision oncology, patients with localized MSI-High (MSI-H) or deficient mismatch repair (dMMR) rectal adenocarcinoma are benefiting from one of the most dramatic paradigm shifts in gastrointestinal cancer care.
Neoadjuvant immunotherapy — using agents such as dostarlimab, pembrolizumab, nivolumab ± ipilimumab — can produce extraordinarily deep and durable responses. Many patients achieve clinical complete response (cCR) or even pathologic complete response (pCR), raising a critical question:
“If the cancer is gone, do we still need surgery?”
The Key Principle
For MSI-H/dMMR rectal cancer, the goal is clear:
Avoid overtreatment while maintaining cure.
Immunotherapy-first strategies now allow selected patients to safely pursue organ preservation through non-operative “Watch-and-Wait” management when a sustained complete response is confirmed.
What the Infographic Breaks Down:
• Clinical scenario for neoadjuvant IO followed by cCR/pCR
• A. Non-operative management (“Watch-and-Wait”) – preferred when sustained cCR is achieved → No immediate surgery, no chemoradiation, no routine adjuvant chemotherapy
• B. Post-surgical true pCR (ypT0N0) → Observation + surveillance only
• Why this works MSI-H tumors are highly immune-sensitive → exceptional pCR/cCR rates Surgery carries real long-term risks: permanent colostomy, infertility, sexual dysfunction, bowel issues, neuropathy
• Evidence that changed the game Dostarlimab MSKCC study (and supporting trials) → very high clinical complete response rates, many patients avoided surgery entirely, durable responses maintained on long-term follow-up
• Strict surveillance protocol (MRI pelvis, endoscopy, DRE, CEA, selective CT) — essential because cCR ≠ pCR (microscopic disease can still exist)
• 2025–2026 Practical Standards table: clear next steps for cCR without surgery, pCR after surgery, residual disease, or progression
• Unresolved questions still evolving: optimal IO duration, role of radiation omission, long-term regrowth risk, ctDNA, ideal patient selection
This approach represents one of the biggest modern advances in GI oncology: Immunotherapy-first organ preservation for MSI-H/dMMR localized rectal cancer — combining evidence, precision, and quality-of-life focus.
Designed as a quick, high-yield reference for oncologists, surgeons, radiation oncologists, fellows, residents, and anyone involved in rectal cancer care.
📌 Save • Share • Discuss
What are your experiences with IO-first strategies in MSI-H rectal cancer? Have you adopted Watch-and-Wait in your practice?
Follow for more visual, evidence-based explanations of complex oncology concepts.
Dr Rupam Manna, MD
Medical Oncologist
X: @DrRupamOncology
#RectalCancer #MSIHigh #dMMR #Immunotherapy #OrganPreservation #WatchAndWait #PrecisionOncology #CancerResearch #GIOncology #pCR #NeoadjuvantTherapy
🫁 Metastatic trajectories in NSCLC: redefining local + systemic therapy through disease evolution! @JCO_ASCO
https://t.co/XcpEhaGHML
▪️ Genomics + ctDNA + radiomics + functional imaging
▪️ Defines progression by pace, pattern, organotropism & resistance mechanisms
▪️ Adaptive strategies: escalate, switch, consolidate or locally ablate
▪️ Could reshape biomarker-driven platform trials in mNSCLC
Not all metastases follow the same road…some take very different “trajectories” 🚦
@OncoAlert@OncoReporte@myESMO@_SEOM@LungCancerRx@Lung_Cancers@gecp_org
“HFS hurts.
HFSR frustrates.
One is collateral damage from chemotherapy.
The other is a pharmacodynamic footprint of VEGF inhibition.
But in clinic?
Both can decide whether treatment continues… or stops.
🔴 HFS (Hand-Foot Syndrome)
→ diffuse redness, swelling, burning
→ classically with capecitabine, 5-FU, liposomal doxorubicin
🔵 HFSR (Hand-Foot Skin Reaction)
→ painful hyperkeratotic lesions at pressure/friction points
→ classically with TKIs like regorafenib, sorafenib, cabozantinib
Same hands.
Very different biology.
And sometimes the toxicity tells you more about the drug than the scan does.
What’s the WORST HFS/HFSR case you’ve seen in practice? 👇
#OncoTwitter #MedTwitter #Oncology
@OncoAlert@myesmo@ESMO_Open
🩺 LFTs are more than just numbers — they reveal the story of liver injury, bile obstruction, and liver function.
Learn the easy approach:
🟡 Bilirubin → Jaundice type
🔴 AST/ALT → Liver cell injury
🟢 ALP/GGT → Cholestasis or obstruction
🔵 Albumin & INR → Liver synthetic function
Recognizing patterns early can help diagnose:
✔️ Viral hepatitis
✔️ Alcoholic liver disease
✔️ Fatty liver
✔️ Obstructive jaundice
✔️ Cirrhosis & liver failure
Interpret LFTs systematically — not randomly. 📋🧠
#LFT #LiverFunctionTest #Hepatology #Medicine #MedTwitter #FOAMed #MedicalEducation #Doctors #MedicalStudent #LiverDisease #ClinicalMedicine #Healthcare #MBBS #InternalMedicine
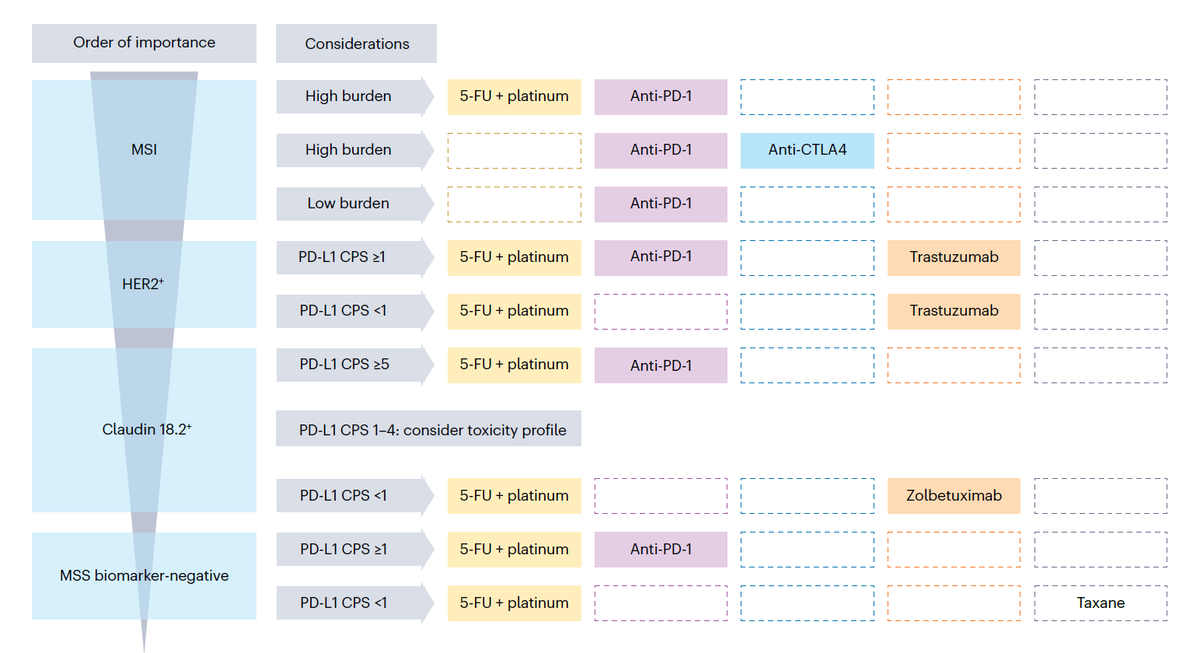
This is an absolutely outstanding review on the management of patients with metastatic gastric cancer.
I may have posted about this review before but it is so good that it deserves another round of applause... Thanks @KlempnerSam@YJanjigianMD@amalsargsyan and all the other co-authors I could not find on X...
Sorry AI, I love you but you are just not there yet. True content experts writing a practical review still beat you easily.
This should be a required read for all who take care of patients with gastric cancer.
https://t.co/5eCIbBwK7G
Porto Alegre será palco de mais uma importante edição do encontro que conecta especialistas, atualização científica e discussões multidisciplinares em oncologia torácica. 🫁
O VI Simpósio GBOT Sul já tem data marcada e reunirá grandes nomes da área para dois dias de troca de conhecimento, debate clínico e aprofundamento nos principais avanços da especialidade.
📍 Hilton Porto Alegre Hotel
📅 31 de julho e 01 de agosto de 2026
A programação contará com uma comissão científica formada por referências da oncologia torácica da região Sul, fortalecendo ainda mais a qualidade científica do evento.
As inscrições já estão abertas. Para mais informações e inscrições, entre em contato pelo e-mail [email protected] ou pelo WhatsApp (51) 99358-3746
#gbot #oncologiatoracica #cancerdepulmao #educacaomedica #eventomedico
🚨 Up to 40% of rectal cancer patients may not need surgery.
In dMMR disease (with proper testing)
Immunotherapy → ~90-100% CR
In MSS
TNT: ~1 in 3 achieve cCR
With watch-and-wait:
~85% keep their rectum
>95% remain metastasis-free
Local regrowth ~15%, mostly detected early and successfully salvaged
It’s smarter upfront intensification then personalized decisions.
But this isn’t a simple algorithm.
It requires clinical judgment, proper testing, careful selection and intensive surveillance.
What once seemed unthinkable is now part of evolving clinical practice; the state of the art care
https://t.co/qM4gjtik8v
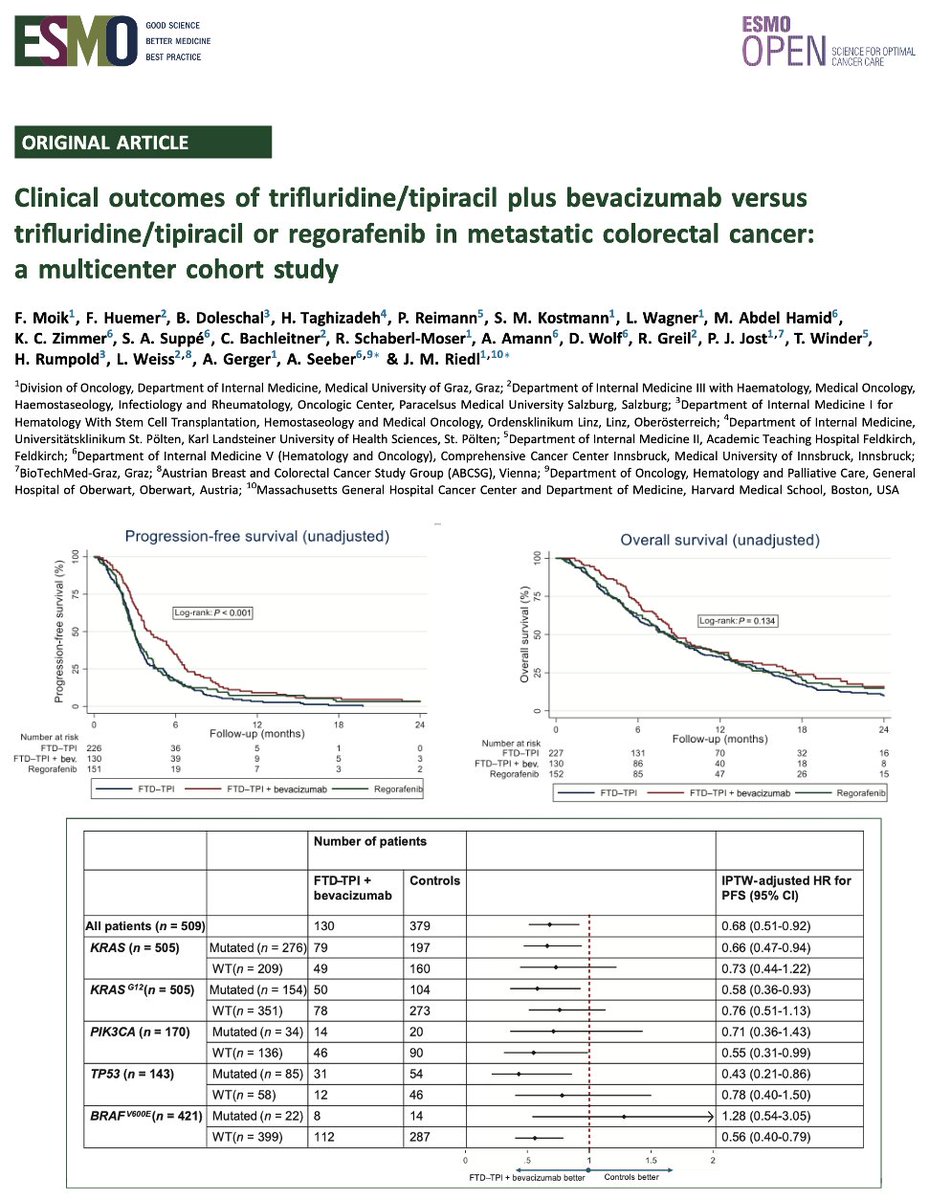
Clinical outcomes of trifluridine/tipiracil plus bevacizumab versus trifluridine/tipiracil or regorafenib in metastatic colorectal cancer: a multicenter cohort study in @ESMO_Open.Improved PFS & DCR with FTD-TPI Bev, including KRAS p.G12C mCRC. https://t.co/HDrVKI40R1
🧪 FOLFIRINOX in digestive NEC
📊 Retrospective (n=50), later lines (82%)
🔹 ORR 44% | DCR 72%
🔹 mPFS 5.6 mo
💥 Notable activity in: CRC NEC (52%), Ki67 <55% (50%), post PE (39%)
👉 Supports FOLFIRINOX as a potential option beyond 1L in aggressive NEC
🔗 https://t.co/Qj7JLAQ2Ae
Japanese subgroup from RATIONALE-306:
1L tislelizumab + chemo showed consistent efficacy & safety in Japanese patients with ESCC, aligning with global population with ≥3Y follow-up
🔗https://t.co/HTKCtFhNzH
@OncoAlert
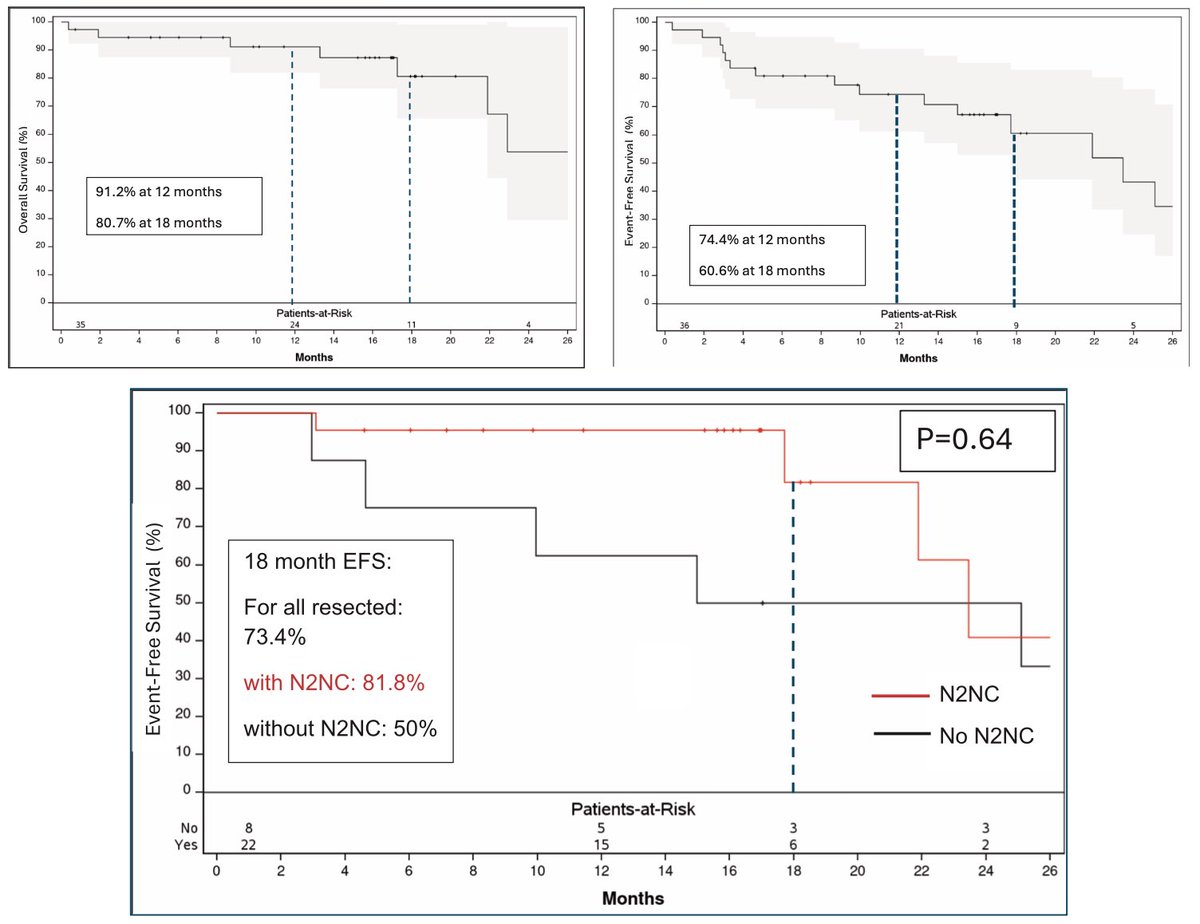
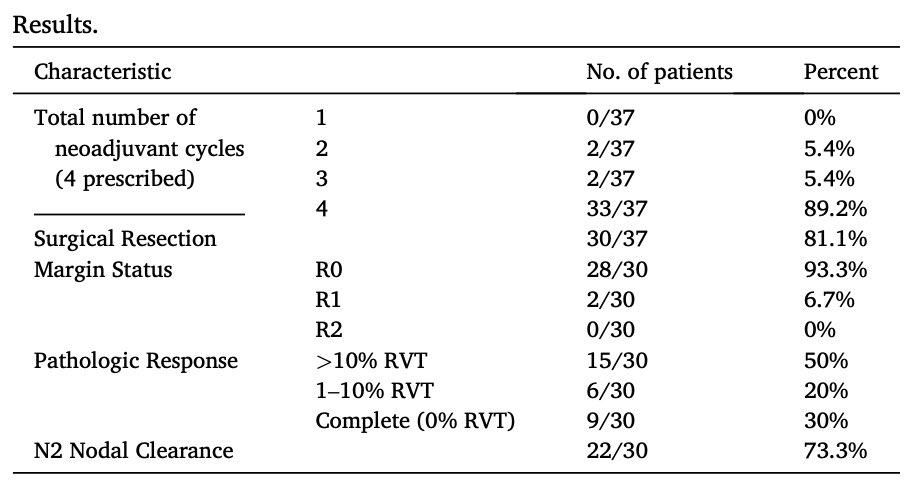
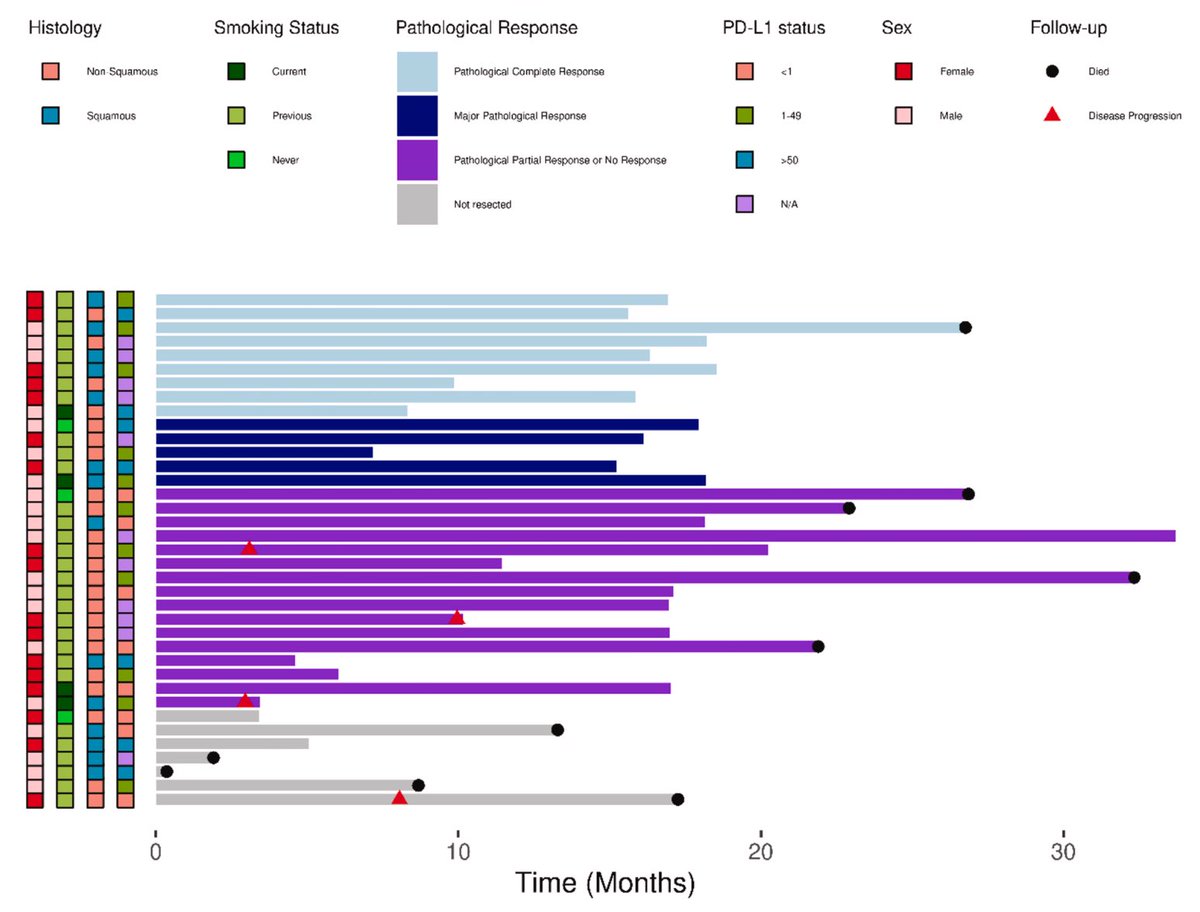
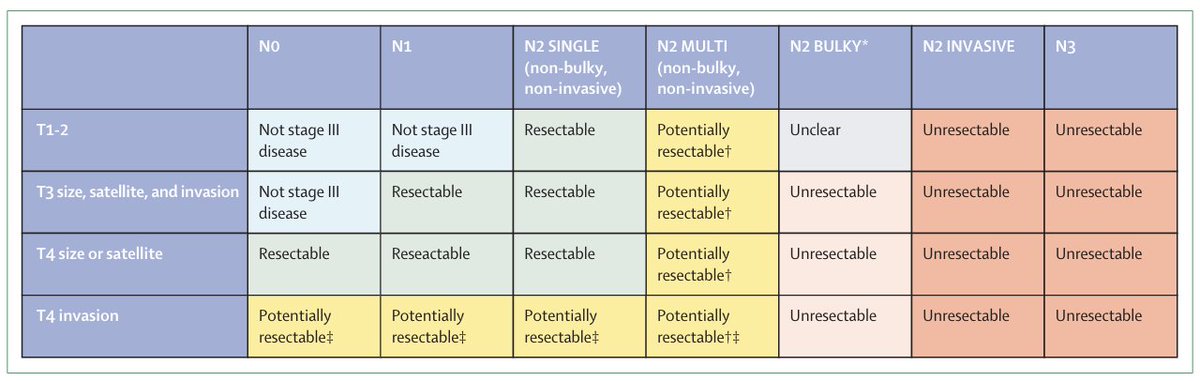
Consensus definition on resectability of stage III NSCLC from @EORTC published @LancetRespirMed. Current consensus is that N3 or bulky N2 is unresectable but multi-station N2 remains potentially resectable. Does not lend itself perfectly to a flowchart given heterogeneity:
Here's the latest on repeat NGS testing for patients with #colorectalcancer. Well done by @OHSU Fellow Dr Nick Kendsersky!
The Evolving Role for Repeat Molecular Testing in Metastatic Colorectal Cancer https://t.co/zVtbrOYfjC #mdpicancers via @Cancers_MDPI