Curve below is OS on PD1 retreat after progression by stage. 31% patients in IGNYTE were stage III which isn't even on here. Note Opdualag is comparator which has 20% risk reduction vs PD1 in 1L. When you adjust for these factors, it is unclear if RP1 is adding much/wins in RCT.
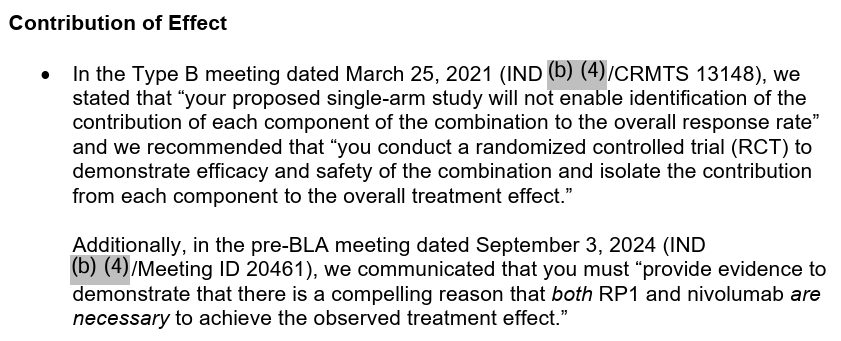
$REPL crazy how the FDA published the CRL from a team under Pazdur citing trial design as a no-go and ppl on here acting like FDA accepting resub is 'right thing to do'. Let be honest there is no objective rationality for AA here, this is politics.
i hesitate to "dump" on @adamfeuerstein. i'm sure he means well! but this post confirms his core skill is mistaking condescension for expertise. he knows very little about prediction markets, incentive design, or what biotech desperately needs. old man, please reconsider.
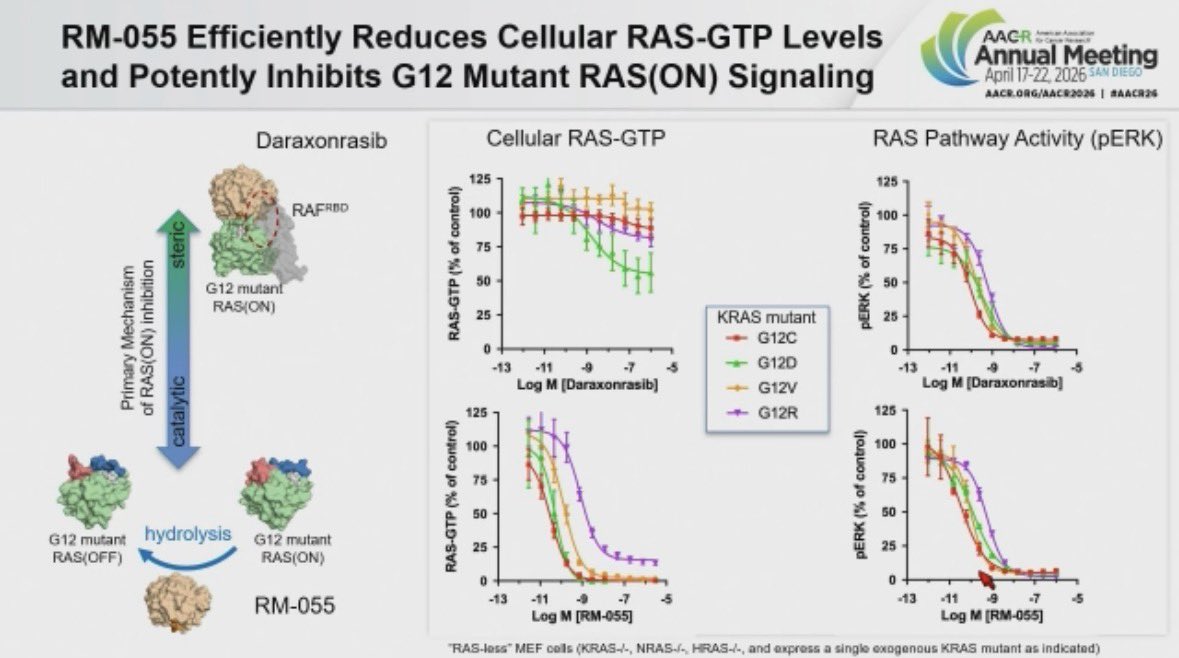
@Banana_Oncology Agree, I just wish they showed the wt hydrolysis to give mechanistic plausibility. I imagine getting selectivity here is not trivial. Also in regards to ear skin, what if there is a ceiling effect on DUSP6 not present in tumor cells? Not saying that's the case but its possible.
@Banana_Oncology Right but that nature paper empirically showed that dara does promote wt hydrolysis similar to mutants. I just wish they showed WT hydrolysis in that 055 chart as would've been moneyshot experiment imo.
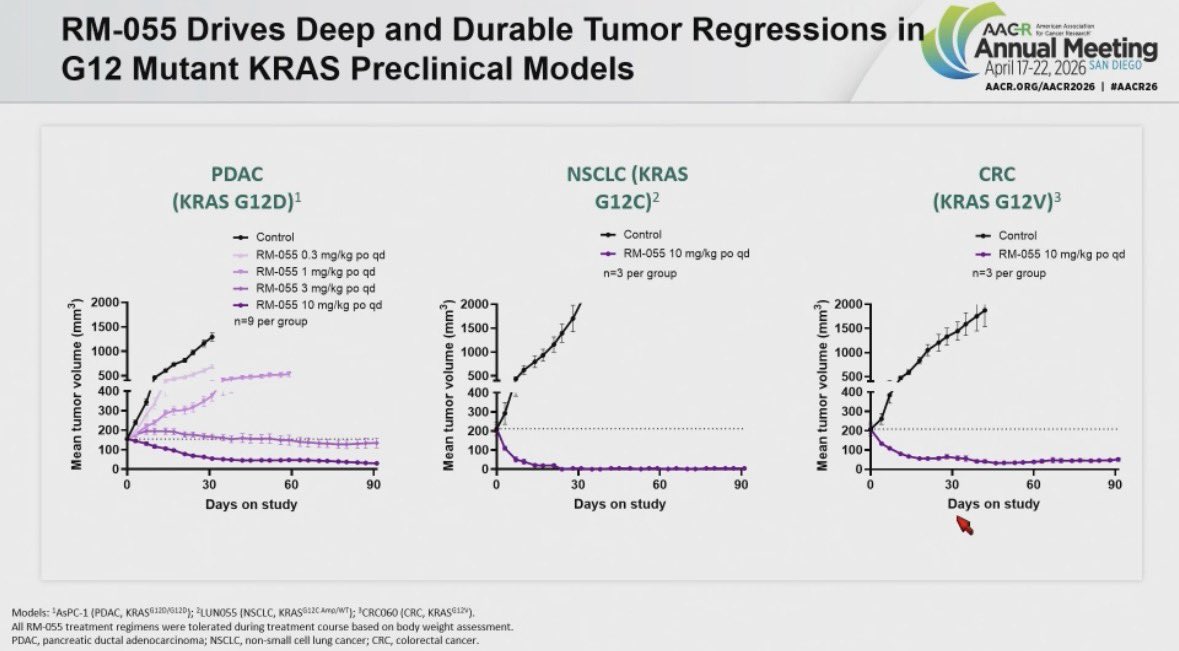
New compound from @RevMedicines RM-055 disclosed at #AACR26
They took a subtle finding 👉🏽Daraxonrasib-CYPA complex modestly increasing RAS GTP hydrolysis 👉🏽 to build a RAS GAP on steroids. RM-055 flattens Daraxonrasib resistant tumors including RAS amplified cases across models.
@augurbio Imo the messaging has been while skin fxn can be used, its not strong enough to stand on its own, ie clear efficacy needs to be there. 1yr 10 patients who cant even deteriorate on upright stability, the only metric where there is no placebo effect isn't all that compelling.
btw $LRMR almost has no shot at AA. Skin fxn is not surrogate for CNS fxn, mFARS improvements in nonamb patients likely just placebo/noise, wont have 30 patients at 6m at filing because 36% discon rate in OLE, modified dosing regimen will only have data in handful of patients..
@augurbio Open to considering is not strong language imo. Besides even that is contingent on demonstrating evidence of exposure-response. On the relevant tissue they leave out cns which should be highly relevant to derisking a confirmatory with upright stability as endpoint.
Straight up lying that fda rugpulled them when they said trial would be unapprovable in 2021. Making 4m a year. What an asshole. At what point do these guys start getting prosecuted for securities fraud?
𝐂𝐨𝐦𝐩𝐚𝐧𝐲 𝐍𝐞𝐰𝐬: After receiving a CRL for its RP1 oncolytic immunotherapy yesterday, the CEO of @Replimune walks us through the program's timeline and history, and what this might mean for its future. $REPL
Full video: https://t.co/x2wDgAa9IV
$REPL CRL is WILD...these guys lied for fucking years. Also FDA is absolutely correct here, management story never made sense, cant comp Gr3 to Gr4 population. Also censoring PD in retreated patients is dirty. V little chance this beats opdualag on OS imo this company should die.
@WillSpagnoli I mean he adopted a dog with a treatable cancer to do a short bus science experiment on and then has some fluff piece written about it leaving out dog was given a separate immunotherapy inciting a circle jerk for techbio chads
Turns out the dog guys vaccine was given concomitant with pd1 and looking for investors…so basically the classic single arm io combo grift has now come to n=1 dog studies. Probably wasn’t even his dog tbh
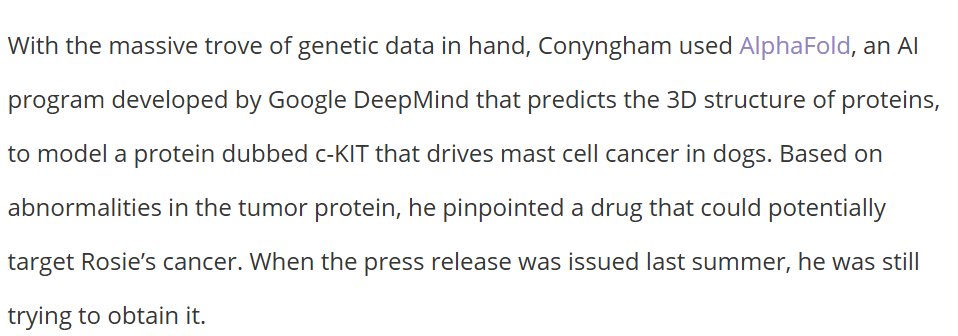
@LizHighleyman My point was he did all this sequencing and protein modeling to pinpoint the tumor driver in an unbiased manner (supposedly) which is already identified for mast cell cancer. Sure enough all this 'work' led him to the target that could've been ID'd w 5 minutes of googling.
Very techbro of the dog guy to sequence and use alphafold to find a bespoke therapy for a cancer that is almost unilaterally driven by KIT which has multiple approved inhibitors