New in #Osteoporosis Int: Evidence-based joint statement position of perioperative bone optimization in the arthroplasty candidate, from FEMECOT, AMMOM, ACOMM, SCCOT, SECOT, SEFRAOS, SEIOMM
Highlights the importance of perioperative bone optimization for all patients undergoing arthroplasty.
#Orthopedics #BoneHealth #Arthroplasty #Osteoporosis
🔗 https://t.co/Za48UkSUJo
🟡CURSO AVALADO POR SCLECARTO🟡
"La fractura de cadera en paciente frágil. ¿Podemos llegar al 0% de complicaciones? Concepto fix and treat."
🗓️20 y 21 de junio
📍Hospital U. Río Hortega, Valladolid
Cursos avalados: https://t.co/wn1Fiz0MaK
Inscripciones: https://t.co/n2vXCfwr6M
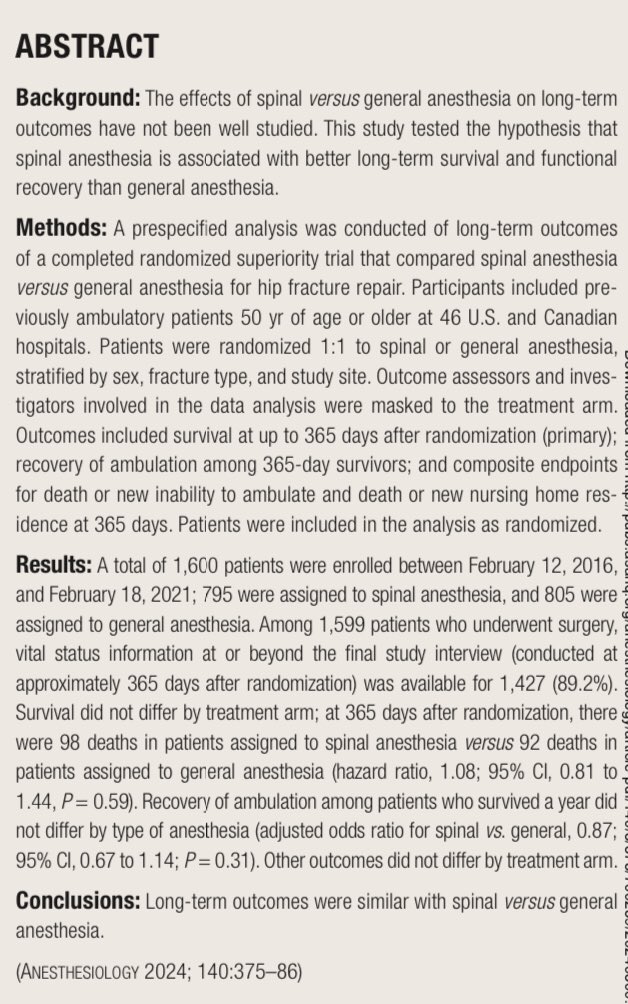
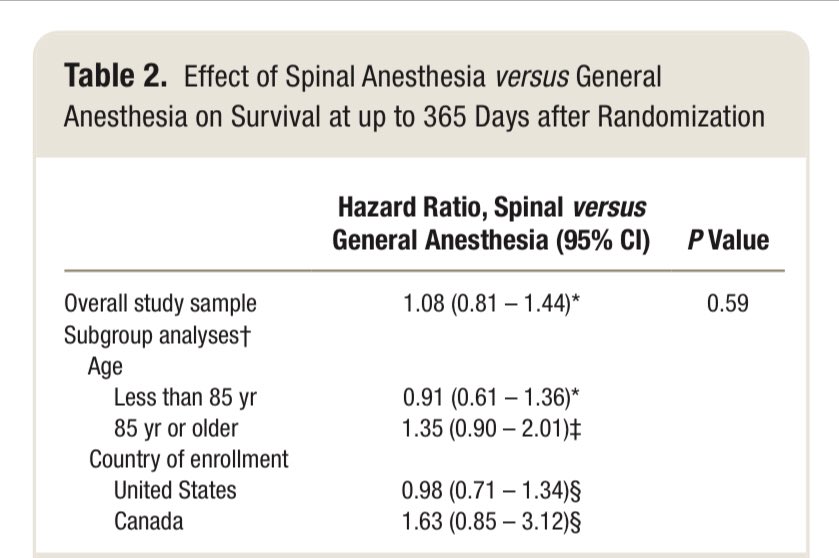
Publicado en @_Anesthesiology los resultados a 1 año de seguimiento del ensayo clínico REGAIN para anestesia espinal vs general en #fxcadera. Sin diferencias en mortalidad / deambulación autónoma. Acceso abierto en enlace https://t.co/qhofDfplHI
Impacto de las fracturas por fragilidad en mujeres españolas con osteoporosis posmenopáusica
https://t.co/nDK8TuXgEQ
por Iñigo Etxebarria @ietxe et al
#fractura#osteoporosis#menopausia
✋🏽 SURGICALLY REDUCING DISPLACED DISTAL RADIAL FRACTURES IN CHILDREN: IS IT WORTH IT? 🏨
Check out an introduction to the Children’s Radius Acute Fracture Fixation Trial (CRAFFT) in the current issue of the #BJJ now!
https://t.co/uCa2QjV4PN
#ChildrensOrtho#Trauma@MrDanPerry
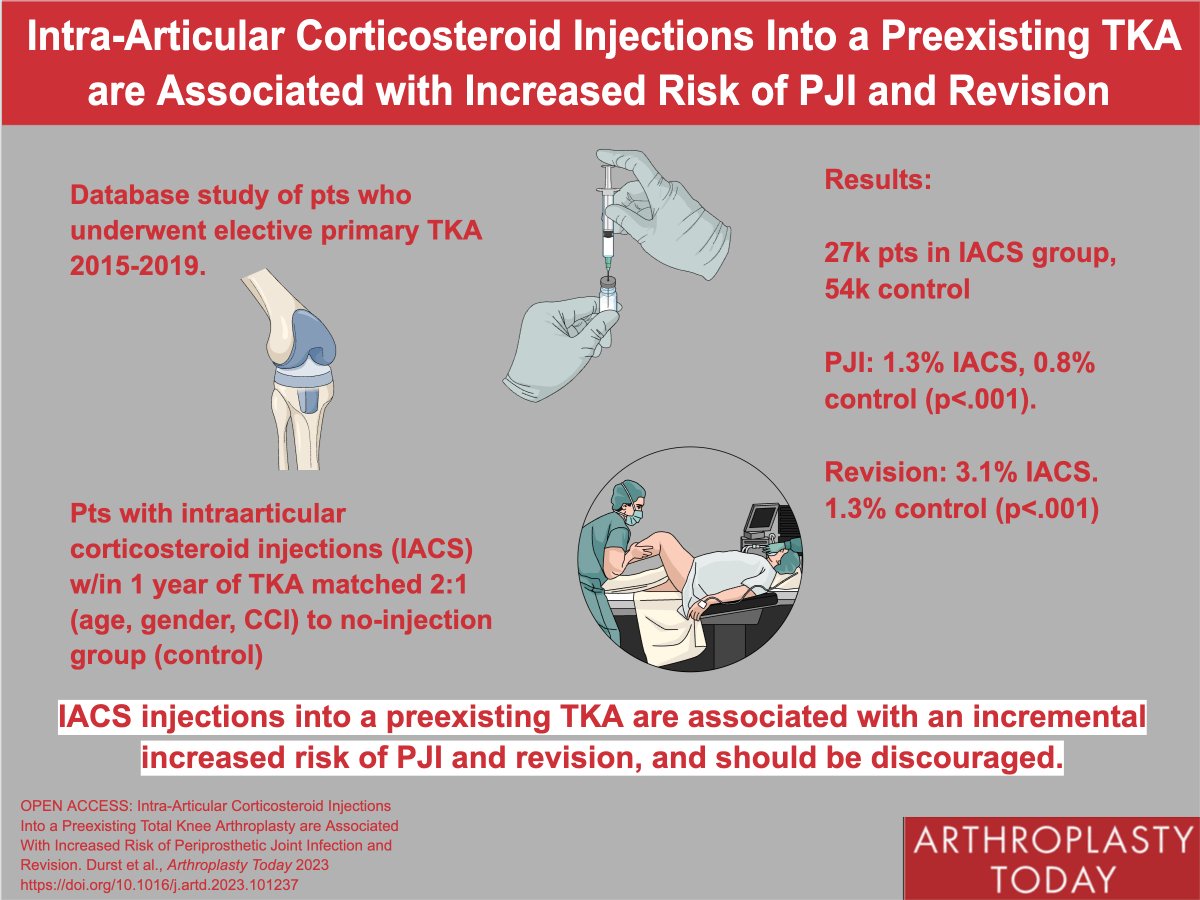
Would you inject steroids into a prosthetic knee? This database study from @CedarsSinaiMed found ⬆️ risk of PJI and revision TKA in pts who had undergone ipsilateral knee steroid injection w/in 1y of TKA. #orthotwitter@AlexisGaskin32@pjamiesonkay
https://t.co/ffcRZJ87WS
💊Aspirin for Thromboprophylaxis After Fracture: The PREVENT CLOT Trial
Published in the @NEJM
Venous thromboembolism is one of the most dangerous complications in trauma cases.
Low molecular weight heparin is regularly used for prophylaxis. But could aspirin be just as good?
🏗️METHODS
This randomized, non-inferiority trial included 21 centers in the US 🇺🇸 and Canada 🇨🇦 randomized 12,211 patients with an extremity, pelvic, or acetabulum fracture to receive:
1⃣ Aspirin (81mg twice daily) (n=6,101)
2⃣ Low-Molecular-Weight Heparin (30mg twice daily enoxaparin) (n=6,110)
The primary outcome of interest was all-cause mortality at 90 days.
Secondary efficacy outcomes included: cause-specific death, non-fatal pulmonary embolism, and deep-vein thrombosis.
Secondary safety outcomes included: bleeding events, wound complications, and surgical site infection.
🔎 RESULTS
All-Cause Mortality
Aspirin was found to be non-inferior to low-molecular-weight heparin (p<0.001)!
Secondary Efficacy Outcomes
Similar rates of cause-specific death (relation to pulmonary embolism) and pulmonary embolism were observed between the two groups.
However, the rate of deep vein thrombosis - in particular distal deep vein thrombosis - was higher in the aspirin group!
Secondary Safety Outcomes
Similar rates of bleeding complications, wound complications, and infection were observed between the two groups.
✅ INTERPRETATION
Aspirin was non-inferior to low-molecular-weight heparin for the prevention of all-cause mortality!
It has a similar safety profile too -- aspirin could be a safe, low-cost alternative for thromboprophylaxis after a fracture!
📅 #Agenda ¡No te pierdas el 10 de febrero en la Jornada de #Ortogeriatría! Un evento donde hablaremos sobre la #fisioterapia en centros residenciales y la prescripción de ejercicio en la Comunidad para prevenir la #fragilidad y #dependencia
Más info: https://t.co/CVw9439Zu3
The most-read paper in the December issue of #BJJ reported that longer time to surgery due to non-medical reasons was associated with higher incidence of postop pressure sores & UTIs.
Read the full paper here!
#OpenAccess#Ortho#Surgery
https://t.co/bBXBDBX3R8
@Wally_Gator_MD@ojedathies@RNFCadera Hay trabajos con diferentes sistemas para pacientes que sufren una fractura de cadera y en el mismo acto quirúrgico proponen fijar la otra. De momento sin grandes resultados. Podría ser interesante, pero fijar sin que haya fractura en una de las 2 no lo veo…
@juanmarodsan96 La ponencia está grabada para los inscritos al congreso. Pero dentro de poco creo que se va a publicar algo al respecto para intentar adecuar esos tiempos antes de la cirugía
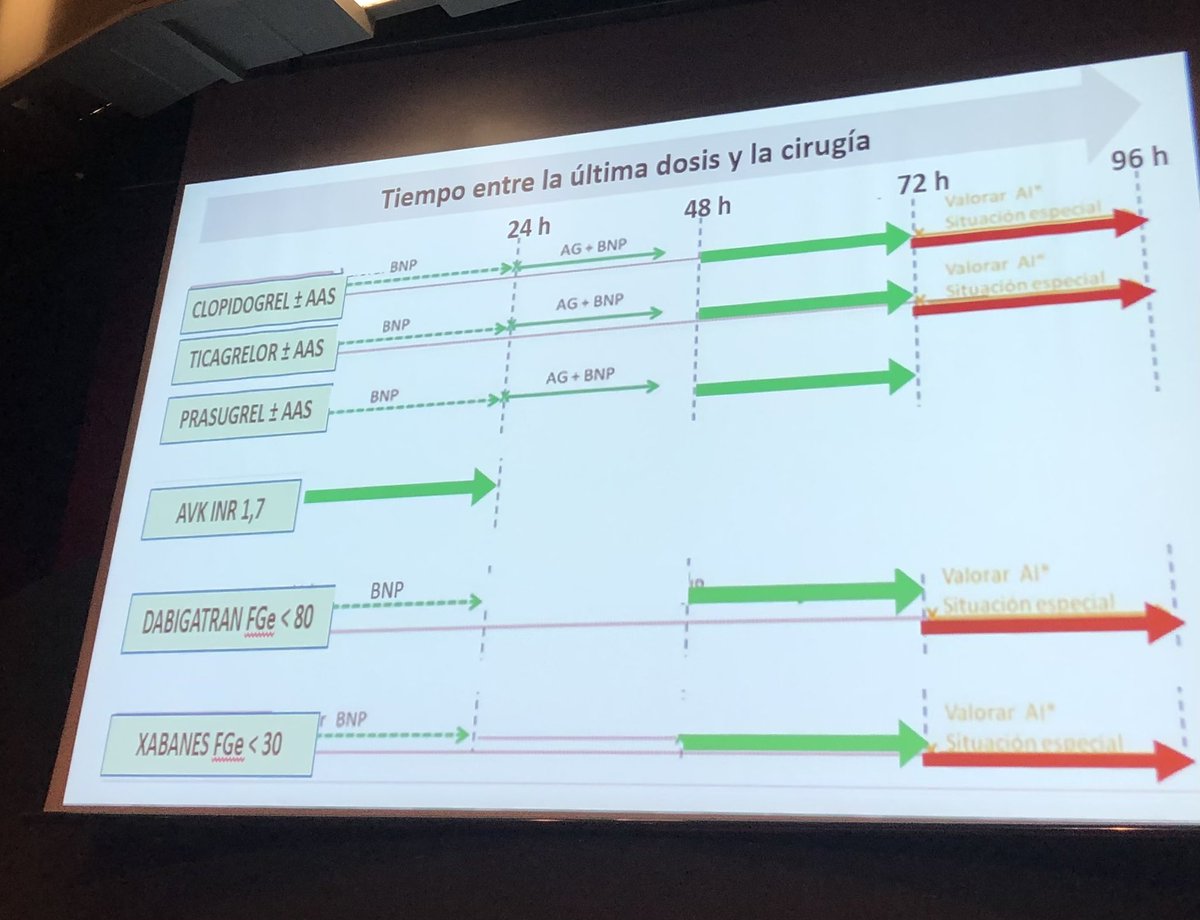
Buenas noticias. Ya lo sabíamos pero lo confirma la Dra. Cassinello, podemos operar con seguridad a los pacientes antiagregados y anticoagulados como lo hacen en el norte de Europa. En 24-48h. Ya es hora de cambiar el paradigma