One of the most revolutionary drugs of our time (Semaglutide, Ozempic) owes its existence not to a sleek laboratory, but to a slow, venomous lizard basking in the American desert.
Come with me, and discover the unlikely journey behind its discovery.
*⃣ The story begins in the deserts of the south-western United States, where the Gila monster (Heloderma suspectum) lives a slow, intermittent feeding life.
Unlike most animals, it may eat only a few times per year, yet it maintains remarkably stable blood glucose levels after large meals. This physiological curiosity drew the attention of endocrinologists in the late 20th century.
*⃣ In the early 1990s, researchers analysing Gila monster venom identified a peptide later named exendin-4. What made it extraordinary was its strong similarity to human GLP-1 (glucagon-like peptide-1), a gut hormone that enhances insulin secretion after meals, suppresses glucagon release, slows gastric emptying and promotes satiety.
🌟 Crucially, exendin-4 was far more resistant to enzymatic degradation than native human GLP-1, giving it a much longer biological half-life.
*⃣ This discovery was a turning point.
Exendin-4 became the blueprint for exenatide, the first GLP-1 receptor agonist approved for type 2 diabetes. From there, medicinal chemistry took over.
*⃣ By subtly modifying the peptide backbone and adding molecular features that improve stability and albumin binding, researchers developed longer-acting, more potent analogues. Semaglutide, the active molecule in Ozempic, is one of these second-generation derivatives. It is fully synthetic, but conceptually descended from that original venom peptide.
*⃣ What makes this story compelling is not the exotic origin alone, but the broader lesson it illustrates.
Evolution has been running biochemical experiments for hundreds of millions of years. Venoms, in particular, are rich libraries of highly selective, receptor-active molecules. Modern pharmacology often succeeds not by inventing biology from scratch, but by recognising, refining and repurposing solutions that nature has already tested.
🚩 In that sense, Ozempic is not “from a lizard” — but without a lizard, it would probably not exist.
Benjamin Franklin is widely recognised for many achievements (pioneering work in electricity, drafting the American Declaration of Independence...). Yet he is far less known for his contribution to the early promotion of smallpox inoculation, a public health intervention that predated vaccination.
This lesser-known facet of Franklin’s life was shaped by personal tragedy.
In 1736, his son Francis died from smallpox, an event that profoundly altered his views on prevention. At the time, variolation—intentional infection with material from smallpox lesions—was already in use but remained controversial due to its risks. Franklin, reflecting on his loss, became a strong advocate for the procedure, convinced that its benefits outweighed its dangers.
Franklin did not rely solely on personal conviction. In a document published in 1759, he presented comparative mortality data between naturally infected individuals and those who had undergone variolation. His analysis showed a consistently lower death rate among the inoculated population.
Although methodologically simple by modern epidemiological standards, this quantitative approach was remarkably forward-thinking and contributed to the growing acceptance of inoculation in both Europe and North America.
By framing the debate in terms of relative risk, Franklin helped shift medical and public opinion toward a more evidence-based perspective.
His efforts played a significant role in legitimising variolation as a preventive strategy, thereby laying conceptual and cultural groundwork for the later introduction of vaccination by Edward Jenner in 1796.
The short guide you need to truly understand GLP-1–based therapies.
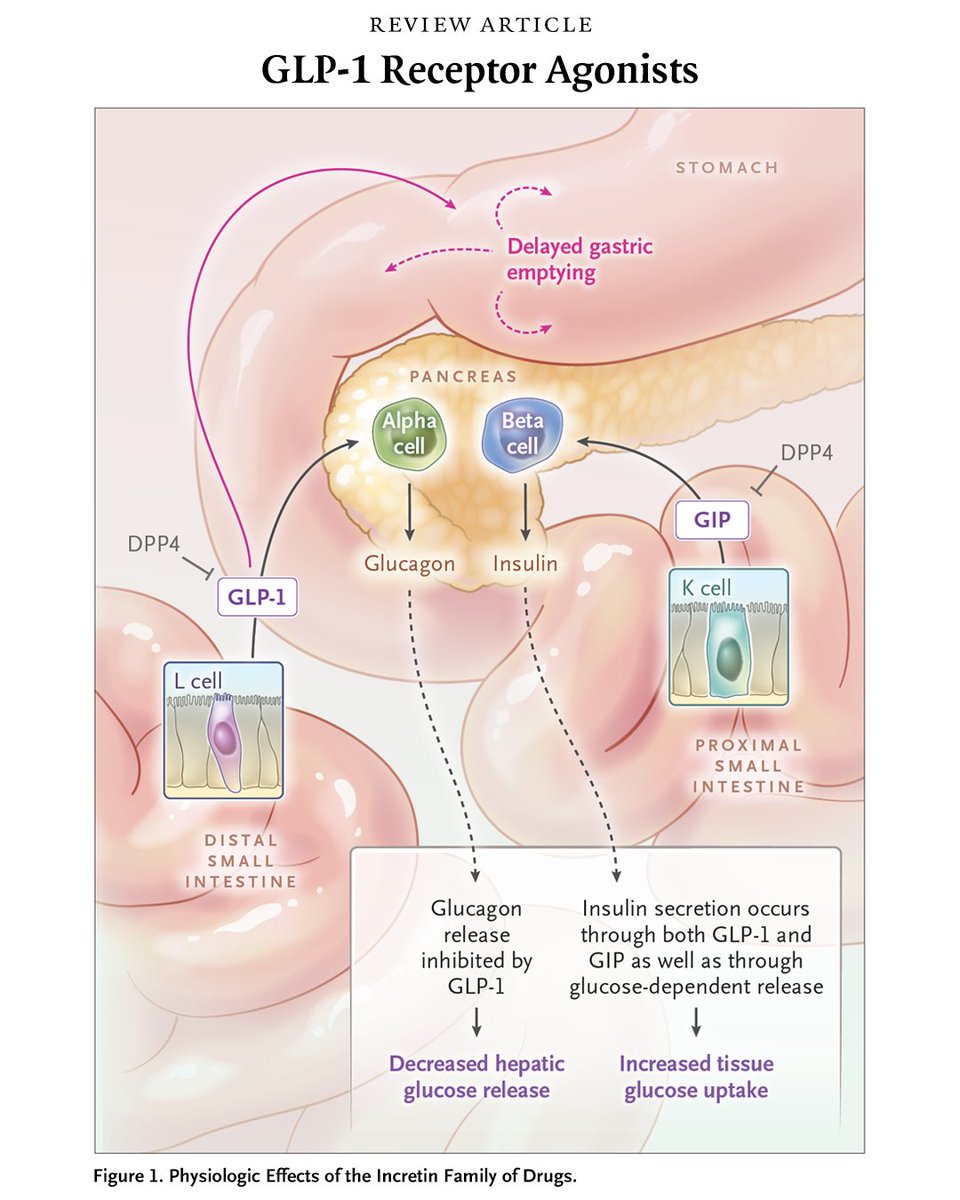
In recent years, few pharmacological developments have reshaped metabolic medicine as profoundly as the incretin-based therapies. Originally rooted in basic physiology, these drugs exploit a simple but elegant observation: oral glucose elicits a greater insulin response than intravenous glucose.
This is the incretin effect.
At the centre of this system are two gut-derived hormones, most notably GLP-1 (glucagon-like peptide-1).
Secreted by enteroendocrine L cells in response to nutrient intake, GLP-1 enhances glucose-dependent insulin secretion, suppresses glucagon release, delays gastric emptying, and promotes satiety. Collectively, these actions align postprandial metabolism with nutrient availability.
Pharmacologically, two main therapeutic strategies have emerged.
- The first involves GLP-1 receptor agonists, such as semaglutide and liraglutide. These molecules mimic endogenous GLP-1 but are structurally modified to resist rapid degradation. Their effects extend beyond glycaemic control: they induce significant weight loss, largely through central appetite regulation and delayed gastric emptying. This has repositioned them not only as antidiabetic agents but as key tools in obesity management.
- The second strategy targets the enzyme DPP-4 (dipeptidyl peptidase-4), which rapidly inactivates endogenous incretins. DPP-4 inhibitors, such as sitagliptin, prolong the action of native GLP-1 and related peptides. Their effect is more modest, but they are orally available and generally well tolerated.
- More recently, dual agonists—such as tirzepatide—have expanded the field by co-activating GLP-1 and GIP receptors, achieving even greater metabolic effects.
What is particularly striking is how these therapies reintroduce a physiological logic into treatment: rather than forcing insulin secretion, they restore context—making insulin release contingent on nutrient presence.
Incretin drugs do not simply lower glucose. They recalibrate the metabolic dialogue between gut, pancreas, and brain.
Leptin exemplifies a broader principle in endocrinology: hormone concentration alone is biologically insufficient; signal transduction competence is equally determinant.
Leptin gene (Ob) was identified in 1994 in a mouse model of severe obesity and hyperphagia. This discovery provided the first molecular evidence that adipose tissue is not merely a passive energy reservoir, but an active endocrine organ capable of signalling energy sufficiency to the brain.
Leptin is a peptide hormone predominantly secreted by white adipocytes in proportion to intracellular triglyceride stores, effectively functioning as a long-term adipostat. That means a self-regulating biological mechanism ("fat thermostat") in the brain, primarily the hypothalamus, that monitors and maintains a consistent level of body fat.
Once released into circulation, it crosses the blood–brain barrier via a saturable transport mechanism and binds to the long isoform of its receptor (Ob-Rb), highly expressed in the hypothalamic arcuate nucleus.
Receptor activation triggers intracellular signalling primarily through the JAK2–STAT3 pathway, with additional contributions from PI3K and MAPK cascades. Functionally, leptin activates anorexigenic neurons while inhibiting orexigenic neurons. The integrated outcome is reduced food intake and increased energy expenditure, partly mediated by sympathetic activation and modulation of the thyroid axis.
Leptin operates as a pleiotropic hormone with systemic reach.
- Reproductive axis: acts as a permissive signal for puberty and fertility via hypothalamic GnRH regulation
- Immune system: promotes Th1 polarisation and pro-inflammatory cytokine production
- Metabolic tissues: modulates insulin sensitivity and lipid oxidation
- Neuroendocrine control: influences both HPA and thyroid axes
These roles reflect its fundamental function as a signal of energy availability to coordinate organismal physiology.
Leptin resistance: the central paradox
In obesity, circulating leptin levels are markedly elevated, yet its central effects are attenuated—a condition termed leptin resistance. Mechanistically, this involves impaired transport across the blood–brain barrier, reduced receptor signalling efficiency, and intracellular inhibitory feedback (notably SOCS3-mediated suppression of JAK–STAT signalling).
The consequence is a maladaptive loop.
Increased adiposity leads to elevated leptin, but diminished central responsiveness sustains hyperphagia and lowers energy expenditure.
Clinically, leptin replacement is highly effective in rare cases of congenital leptin deficiency, restoring normal appetite and metabolic control. However, in common obesity, therapeutic strategies must address leptin resistance rather than hormone deficiency.
His discovery was rejected.
His experiments were dangerous.
His conclusions contradicted everything chemists believed.
But, he was right.
At the beginning of the 19th century, Friedrich Sertürner isolated a crystalline compound from opium that would not only become the first modern analgesic, but also overturn one of the central assumptions of medicinal chemistry…
He named it Morphium, after Morpheus, the Greek god of dreams. What is critical here is not only the pharmacological activity, but the chemical nature of the compound.
At that time, the prevailing paradigm in pharmacognosy and early organic chemistry held that the “active principles” of medicinal plants were acidic in nature. This belief derived from earlier successes in isolating organic acids such as tartaric and citric acid, which reinforced a reductionist but ultimately flawed framework: biological activity was assumed to correlate with acidity.
Sertürner’s compound directly contradicted this dogma.
Morphine was not an acid—it was a basic, nitrogen-containing molecule, inaugurating what would later be defined as the class of alkaloids. This was a profound epistemological shift: it established that plant bioactivity could reside in organic bases, thereby expanding the chemical landscape of pharmacologically active compounds.
Equally transformative was the fact that Sertürner isolated morphine in a pure, crystalline form.
For the first time, a drug derived from a plant could be quantified, titrated, and administered with controlled dosing. This marked a decisive transition from empirical phytotherapy—where variability in plant extracts led to unpredictable effects—to a proto-pharmacological model grounded in dose–response relationships.
Sertürner himself explored these relationships experimentally, in a manner that today would raise serious ethical concerns but was methodologically revealing. He conducted self-experiments and trials on acquaintances, administering measured doses of morphine.
Through these observations, he described a clear dose-dependent progression of effects: at lower doses, morphine induced euphoria and analgesia; as the dose increased, these effects transitioned into dizziness and somnolence; and with approximately doubled concentrations, profound sedation and sleep ensued.
These observations constitute one of the earliest documented characterizations of a graded pharmacodynamic response, anticipating the modern concept of therapeutic windows and toxicity thresholds.
Despite the robustness of his findings, Sertürner’s initial publications were met with skepticism and even rejection.
His conclusions challenged entrenched chemical doctrine, and the notion that a basic compound could be the principal active agent of opium was considered implausible.
The resistance he encountered reflects the inertia of scientific paradigms: evidence alone is often insufficient when it conflicts with established theoretical frameworks.
Only after repeated publications, broader dissemination, and independent confirmation did the scientific community begin to accept his work.
The implications were far-reaching.
Morphine became the prototype for a new class of compounds, and its discovery catalyzed the isolation of other alkaloids such as quinine, strychnine, and caffeine.
More importantly, it established a new principle: that specific physiological effects can be attributed to discrete, chemically defined molecules, whose activity depends on dose and molecular structure.
Thus, the isolation of morphine was not simply the discovery of a powerful analgesic—it was the collapse of a chemical dogma and the birth of molecular pharmacology.
It redefined how drugs were conceptualized, studied, and administered, and it introduced a quantitative, experimental approach that remains foundational in biomedical science.
Cancer is often described as a genetic disease—but that statement is incomplete unless we understand which mutations actually matter.
Tumours accumulate thousands of genomic alterations over time.
However, not all of them contribute to the disease. This distinction led to one of the most important conceptual frameworks in oncology: driver versus passenger mutations.
✳️ Driver mutations are the ones that change the rules of the game.
They confer a selective advantage to the cell, allowing it to proliferate faster, evade apoptosis, adapt to hypoxia, or escape immune surveillance. In evolutionary terms, they are under positive selection. Without them, cancer does not develop.
At the molecular level, drivers typically affect three major classes of genes.
- Oncogenes become constitutively active (for example, mutations in KRAS or BRAF).
- Tumour suppressor genes are inactivated (such as TP53).
- DNA repair systems are compromised (e.g. BRCA1).
The result is not just growth, but uncontrolled, deregulated growth with evolutionary potential.
Importantly, not all drivers appear at the same time. Some occur early and are present in all tumour cells (so-called truncal drivers), while others arise later in subclones, contributing to intra-tumour heterogeneity and therapeutic resistance.
✳️ In contrast, passenger mutations are biologically neutral—at least in principle.
They accumulate as a by-product of genomic instability, particularly in tumours with defective DNA repair. These mutations are not under selection and do not directly contribute to the malignant phenotype. In many cancers, the vast majority of detected mutations fall into this category.
However, dismissing passengers as irrelevant would be an oversimplification.
- First, they provide a molecular record of the tumour’s evolutionary history, allowing reconstruction of clonal dynamics.
- Second, some passenger mutations generate neoantigens, which can be recognised by the immune system—this is one of the mechanistic bases underlying the association between high mutational burden and response to immunotherapy.
The key challenge, both experimentally and clinically, is therefore not detecting mutations—but distinguishing signal from noise.
In essence, cancer genomes are not just chaotic. They are structured by selection, where a small number of driver events shape the disease, and a vast background of passengers reflects the instability that fuels it.
The architecture of intestinal villi and microvilli is regionally specialized along the small intestine, reflecting functional compartmentalization.
In the duodenum, villi are broad and leaf-shaped, optimised for rapid mixing and initial nutrient absorption.
The jejunum displays tall, slender, finger-like villi with dense microvilli, maximising absorptive surface for carbohydrates and amino acids.
In contrast, the ileum exhibits shorter, sparser villi and relatively reduced microvillar density, consistent with its role in bile salt and vitamin B12 uptake.
Additionally, glycocalyx composition and transporter expression vary, indicating that not only morphology but also molecular specialization underpins segment-specific absorptive efficiency.
Bilirubin Production and Excretion.
Red blood cells (RBCs) are viable for about 120 days, and new cells are continually being produced to replace damaged old cells.
MPS cells (Mononuclear Phagocyte System) throughout the body (especially Kupffer cells in the liver and spleen macrophages) remove and break down the old red blood cells, so that the iron can be recycled and waste eliminated.
Bilirubin is a by-product of RBC heme-group degradation and is eliminated from the body by incorporation into bile (and subsequent loss in feces) and by urinary excretion as urobilinogen.
The addition of bilirubin to bile, and its excretion in feces, contributes to the pigmentation of the feces and urine. The bile pathway of excretion is important for ridding the body of excess bilirubin.
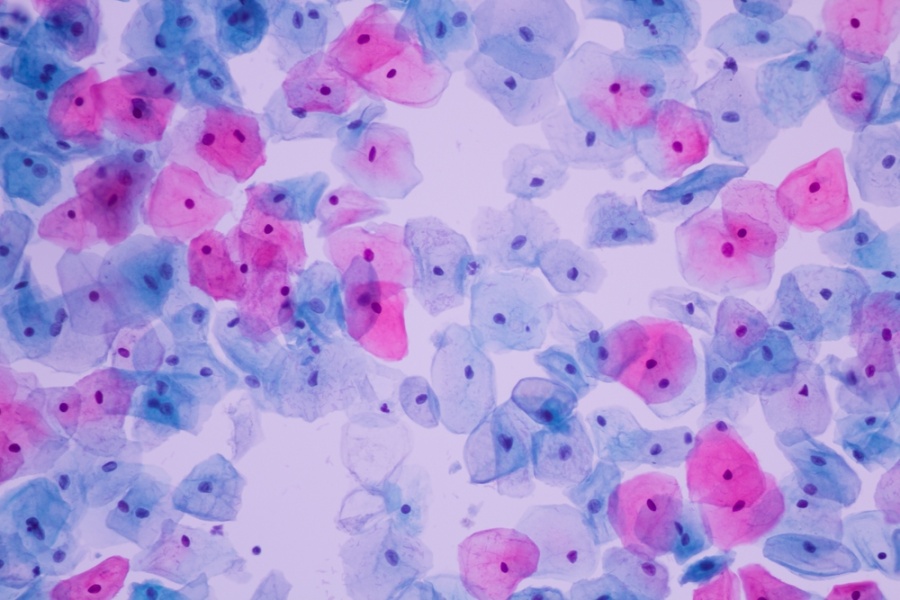
The stained smears of the female reproductive tract possess a quiet, unexpected beauty. Under the microscope, layers of colour unfold with an almost abstract elegance: blues, pinks, and amber tones arranged in cellular geometries that could have inspired Kandinsky himself.
🌟 Yet this visual poetry is not mere aesthetics. It marks one of the greatest achievements in modern medicine—the prevention of a deadly female cancer—made possible by scientific devotion, patience, and the extraordinary partnership of a couple.
🚩 In this post, I am presenting one of the major milestones of twentieth-century medicine, comparable to antibiotics and vaccines in terms of lives saved: the Papanicolaou test, or cervical cytology. Simple, minimally invasive, painless, and inexpensive, it has transformed women’s health and public health policy worldwide. The Pap test is not just a medical procedure; it is a story of science, love, and perseverance that has saved millions of women’s lives.
▶️ The history behind
In 1913, a young Greek physician, George Papanicolaou, arrived in the United States aged 30, carrying little more than 250 dollars and accompanied by his wife, Mary Papanicolaou, who would become his inseparable partner in life and in the laboratory.
George aspired to be a scientist, despite his father’s wish that he become a surgeon. In New York, he survived on whatever work he could find, even playing the violin in restaurants, until he eventually secured a position at Cornell University. There, he began to study cells.
In 1928, after examining a cervical sample, he observed something remarkable: cells showing malignant changes. Cervical cytology had been born. Yet the medical community dismissed his findings, and his work was largely ignored.
Mary never allowed him to give up. For more than twenty years, she underwent daily sampling, assisted in every experiment, and sustained him during moments of doubt. She was simultaneously his muse, his technician, and his emotional anchor.
By the 1940s, the “Pap test” began to gain acceptance. Medical associations and women’s health advocates broke longstanding taboos surrounding vaginal smears. The impact was profound: mortality from cervical cancer fell by over 70% within a few decades.
Today, the World Health Organization considers cervical cancer a disease that could be eliminated this century through HPV vaccination combined with systematic screening.
▶️ The biological perspective
The cervix is a dynamic tissue. Its epithelium constantly renews itself, shedding cells into the vaginal lumen. Persistent infection with high-risk human papillomavirus induces characteristic morphological changes: koilocytosis, dysplasia, nuclear enlargement, and chromatin irregularities.
The Pap test relies on a sophisticated interplay of stains that reveal nuclear architecture (haematoxylin) and cytoplasmic maturation (Orange G and eosin-azure). Interpretation requires contextual knowledge of the menstrual cycle, which enhances both sensitivity and specificity.
Through these stains, the cytologist can distinguish superficial, intermediate, and basal squamous cells; metaplastic and endocervical cells; and the hallmarks of premalignant and malignant transformation, including altered nuclear-to-cytoplasmic ratios and pleomorphism. Lesions typically progress along a continuum from low-grade intraepithelial changes to high-grade lesions, carcinoma in situ, and finally invasive cancer.
Importantly, cervical epithelium is hormonally responsive. Fluctuations in oestrogen and progesterone shape the cellular composition of the smear, allowing cytology to serve as a readout of the vaginal maturation index, a classic tool in gynaecological endocrinology. Deviations from expected cellular patterns may suggest endocrine disorders, atrophy, chronic inflammation, or intraepithelial neoplasia.
▶️ The power of the Pap test lies in time.
It exploits the long window—often years—between initial HPV infection and invasive cancer, making early detection both effective and economical. It stands as a paradigm of preventive medicine and a gateway to broader sexual health interventions, including education and STI prevention.
Today, cytology is increasingly complemented by molecular HPV testing, allowing longer screening intervals when results are negative. However, access remains uneven. In low-resource settings, limited screening coverage continues to translate into preventable deaths, highlighting a persistent global challenge in health equity.
@ProfSirera Absolutely impressed!! What might appear as abstract, decorative patterns are in fact highly ordered biological signatures, where nuclear architecture and cytoplasmic maturation are rendered visible through colour.
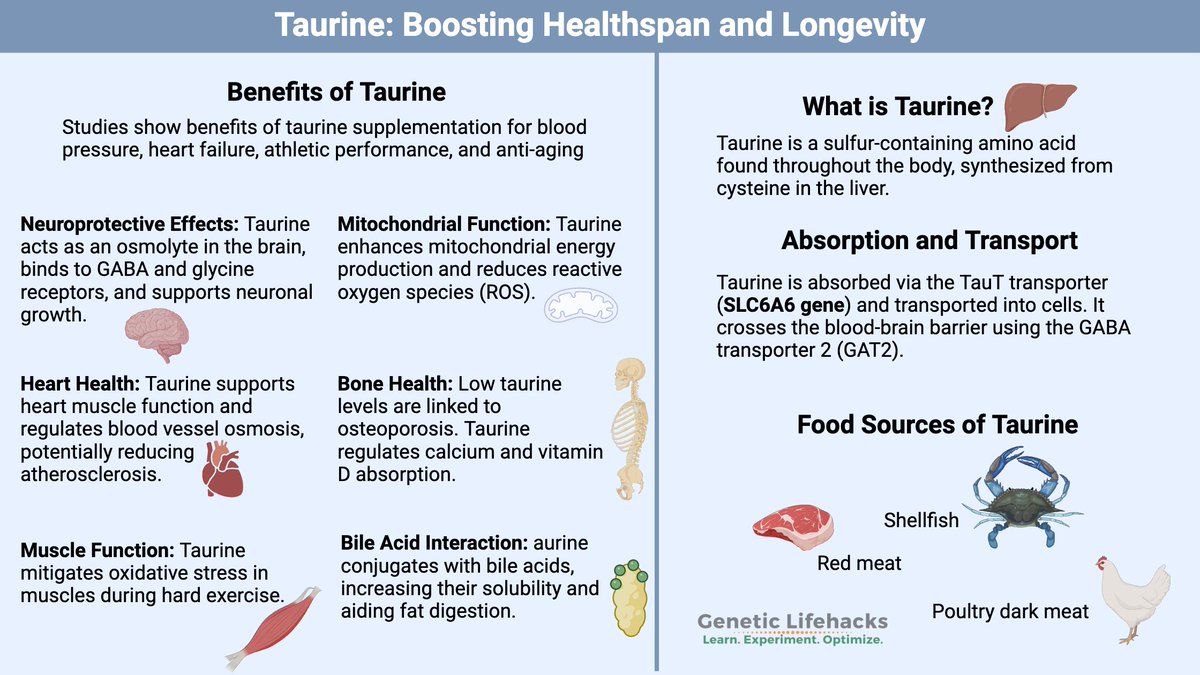
Taurine is a sulphur-containing β-amino acid that, unlike most amino acids, is not incorporated into proteins but exists freely in high concentrations in excitable tissues such as the brain, heart, and retina.
In physiological terms, taurine plays diverse and crucial roles.
1⃣ Biochemically, it is synthesised mainly in the liver from cysteine. This pathway depends on vitamin B6 and is part of the transsulphuration route linking methionine and cysteine metabolism.
Because human synthesis is relatively inefficient, taurine is considered conditionally essential, especially in infants or individuals with hepatic dysfunction.
2⃣ As an osmolyte, it regulates cell volume under osmotic stress by balancing intracellular and extracellular ion concentrations through specific taurine transporters (TauT). This mechanism maintains membrane integrity in the brain, kidney, and myocardium during osmotic fluctuations.
3⃣ In the liver, taurine conjugates with bile acids such as cholic acid to form taurocholate, enhancing the solubility and emulsifying properties of bile salts essential for lipid digestion and absorption of fat-soluble vitamins.
4⃣ Within the central nervous system, taurine functions as a neuromodulator, interacting with GABA and glycinereceptors to exert inhibitory, neuroprotective effects and stabilise calcium flux and membrane potential.
5⃣ In the retina, it is indispensable for photoreceptor survival, preventing oxidative and excitotoxic damage; its deficiency leads to retinal degeneration and visual loss.
6⃣ Taurine-rich foods include seafood, especially shellfish and oil-rich-fish. Meats also provide significant amounts. Plant foods contain virtually none. Human breast milk is naturally rich in taurine, reflecting its importance in neonatal brain and retinal development.
7⃣ In addition to food sources, taurine is widely found in energy drinks such as Red Bull and Monster. While often associated with caffeine, taurine itself is not a stimulant; instead, it supports neuromodulation, osmoregulation, and membrane stability under stress or fatigue.
It stands as a silent biochemical guardian, preserving cellular balance and function across diverse tissues due to its remarkable versatility.
Not as universally renowned as the Sistine Chapel, yet I would argue that it rivals it in artistic power and historical depth. And stay tuned: in just one week we will unveil another set of restored ceiling paintings from fire and ash, this time in one of Valencia’s oldest churches, Santos Juanes.
@ProfSirera Enantiomers often exhibit distinct interactions with enzymes, receptors, transporters, and antibodies, despite having identical physicochemical properties in an achiral environment.
@ProfSirera ChatGPT said:Lysosomes are classically described as the cell’s digestive system, but their functional spectrum is far broader and central to cell physiology, signaling, and homeostasis.
The term lysosome comes from the Greek roots lysis, meaning “loosening,” “dissolution,” or “breaking down,” and soma, meaning “body.”
It was introduced by Christian de Duve in 1955 after discovering membrane-bound organelles rich in hydrolytic enzymes capable of degrading macromolecules.
The name reflects their essential function as “digestive bodies” within the cell, responsible for breaking down worn-out organelles, engulfed particles, and cellular debris.
Thus, lysosome literally means “body that breaks down,” encapsulating their role in intracellular digestion, recycling, and maintaining cellular homeostasis.