Microcytic anemia is not always iron deficiency.
Think TAILS: Thalassemia, Anemia of chronic disease/inflammation, Iron deficiency, Lead poisoning, and Sideroblastic anemia. A simple high-yield framework for quick differentiation in clinical practice and exam revision.
What’s new in ILD 2025? 🫁
Nueva clasificación ERS/ATS:
🔹 Más allá de “idiopático”
🔹 Nuevos términos (BIP, DAD)
🔹 Patrón ≠ diagnóstico
🔹 Enfoque en comportamiento (PPF)
Not only systemic steroids matter. Higher cumulative topical corticosteroid exposure was associated with osteoporosis and major osteoporotic fractures. #BoneHealth#Dermatology
💡SLE -PAH is an unexplored yet severe entity in lupus
💡RNP association - higher PAH, more anti-PAH therapy
💡 No antibody-associated PAH behaves refractorily
👉Multiple antibody positivity - inflammatory, more resolution of PAH
👉https://t.co/nrf9EoeOLH
PMID: 41607606
Azathioprine [thiopurines] ⬆️ risk of Intra-hepatic Cholestasis of pregnancy
🚩Safe but not risk free
➡️Use lowest effective dose
➡️Monitor metabolites if access [6-TGN & 6MMP ratio]
➡️Monitor for pruritus, rising bile acid, & LFTs
💊 Switch to tacrolimus if shunting or ICP
A subset of patients with Still’s disease had high type I IFN gene signature assoc with lung disease and drug-assoc immune reactions to IL-1/IL-6 inhibitors. These also linked to rare genetic variation in IFN-related immune pathways
A&R
https://t.co/lu5yOt0Inc
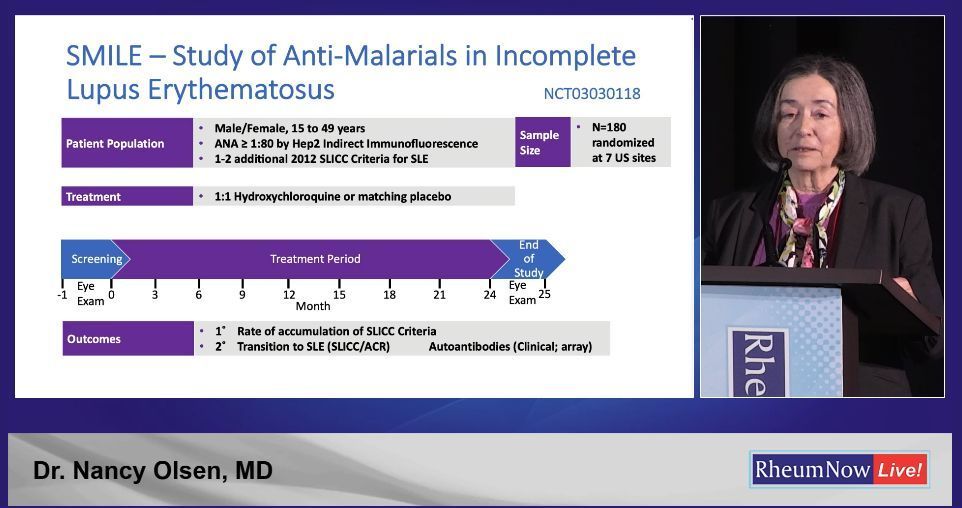
Prevention in Lupus and Therapeutic Evolution in Sjögren’s explores the proactive approach in autoimmune diseases, moving from theory to empirical evaluation. Recent discussions on incomplete lupus and the SMILE trial, along with advancements in Sjögren’s treatments, underscore the promise and complexity of prevention and precision in systemic autoimmunity.
https://t.co/rSrefjkBV9
You know APS is antibody-mediated.
We test anti-β2GPI.
We test anticardiolipin.
We test lupus anticoagulant.
In pregnancy, we give heparin.
But lupus anticoagulant isn’t a single antibody.
And heparin isn’t just a blood thinner.
Yet both revolve around one molecule: β2GPI.
Let me explain.🧵👇
1-APS is NOT truly about phospholipids
Despite the name “antiphospholipid,”
the main pathogenic target is β2-glycoprotein I (β2GPI) -a phospholipid-binding protein.
Cardiolipin is the surface.
β2GPI is the antigen.
2-What is lupus anticoagulant (LA)?
LA is not a specific antibody.
It is a functional laboratory phenomenon:
An antibody that prolongs phospholipid-dependent clotting assays (like dRVVT or aPTT) and corrects with excess phospholipid.
3-Why does LA prolong clotting in vitro?
Clotting assays require phospholipid surfaces.
In many APS patients:
• β2GPI binds phospholipid
• Anti-β2GPI antibodies bind β2GPI
• This interferes with coagulation complex assembly
→ Clotting time prolongs.
That’s why it’s called “anticoagulant.”
4-But not all LA is anti-β2GPI
Important nuance:
Some LA activity is prothrombin-dependent (e.g., aPS/PT antibodies).
So LA is heterogeneous.
But in high-risk APS (especially triple positive patients),
LA is often β2GPI-dependent — and strongly associated with thrombosis.
5-Now shift to obstetric APS
Pregnancy loss in APS is not just thrombosis.
Placental studies and animal models show:
• Complement activation
• Trophoblast injury
• Impaired placental remodeling
Sometimes with minimal thrombosis.
This is immune-mediated placental dysfunction.
6-β2GPI at the maternal–fetal interface
β2GPI binds trophoblast membranes.
Anti-β2GPI antibodies:
• Inhibit trophoblast invasion
• Increase apoptosis
• Trigger complement cascade
The placenta becomes the target.
7-So why does heparin help?
If pregnancy loss were purely thrombotic,
aspirin alone should be enough.
But aspirin + heparin improves live birth rates.
Because heparin does more than anticoagulation..
8-Heparin disrupts β2GPI biology
Heparin binds a heparin-binding region in domain V of β2GPI.
This can:
• Reduce β2GPI binding to phospholipids
• Interfere with antibody clustering
• Promote β2GPI inactivation in some settings
9-Complement may be the key
Animal models show:
Block complement → prevent aPL-mediated fetal loss.
Heparin reduces complement activation at the placenta.
This may be central to its benefit in obstetric APS.
10- The concept
APS revolves around β2GPI.
Lupus anticoagulant is a functional manifestation, often reflecting antibodies that disrupt phospholipid surfaces (frequently β2GPI-dependent, but not always).
And in pregnancy:
Heparin works not only by preventing clots..
but by modulating β2GPI interactions and complement activation.
Same axis.
Different angles.
One central protein.
β2GPI.
#Rheumatology #APS #ObstetricAPS #Lupus #Immunology @DrAkhilX @IhabFathiSulima
𝗠𝗲𝗹𝘁𝘇𝗲𝗿'𝘀 𝘁𝗿𝗶𝗮𝗱 (𝗰𝗿𝘆𝗼𝗴𝗹𝗼𝗯𝘂𝗹𝗶𝗻𝗲𝗺𝗶𝗮)
◦ The triad of palpable purpura, weakness (often manifesting as fatigue), and arthralgia is known as Meltzer's triad.
◦ It was identified in 1966 by M. Meltzer and E.C. Franklin (along with colleagues) in a landmark study of 29 patients suffering from cryoglobulinemia.
◦ This triad is characteristically associated with mixed cryoglobulinemia (types II and III), often triggered by chronic conditions such as hepatitis C virus infection, autoimmune diseases, or certain hematologic malignancies.
◦ Cryoglobulinemia is a rare medical condition characterized by the presence of abnormal proteins called cryoglobulins in the blood, which precipitate or clump together at low temperatures.
◦ These cryoglobulins, composed of immunoglobulins and sometimes complement components, deposit in small- to medium-sized blood vessels throughout the body, causing endothelial injury and end-organ damage.
◦ Cryoglobulins can cause a range of symptoms, including joint pain, skin rashes, and kidney problems, due to their tendency to obstruct blood vessels and trigger inflammatory reactions.
📸 Clinical, serological and pathological hallmarks of cryoglobulinemia.
*From: Roccatello, D., Saadoun, D., Ramos-Casals, M. et al. Cryoglobulinaemia. Nat Rev Dis Primers 4, 11 (2018).
🔗https://t.co/a0ergqppAg
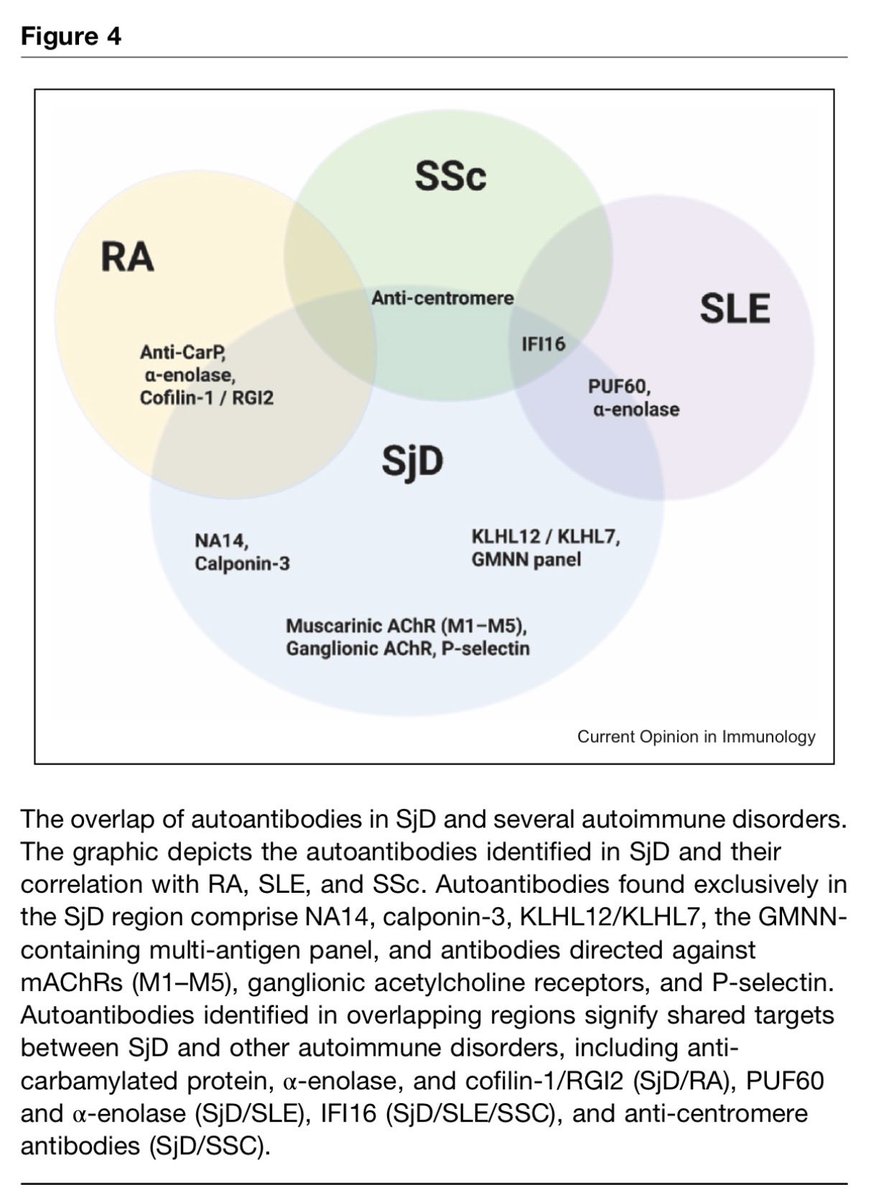
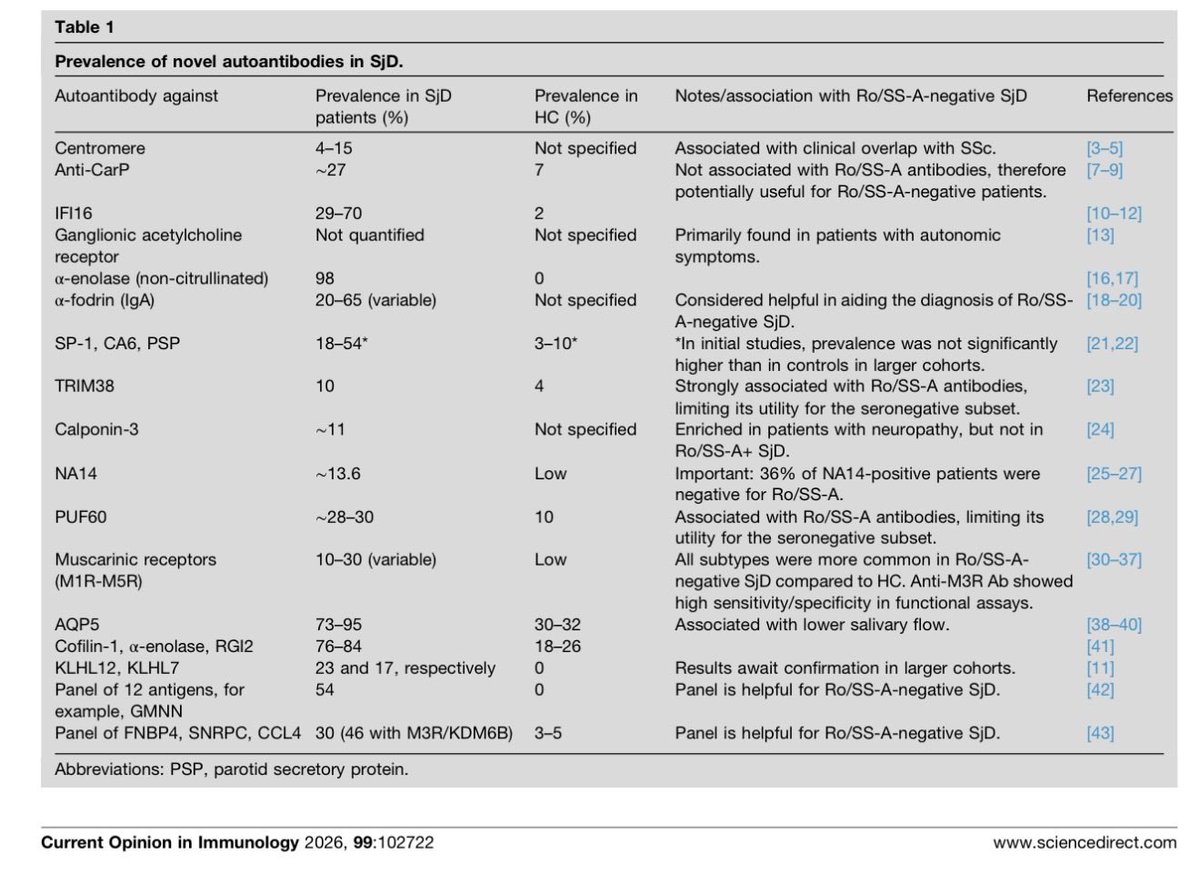
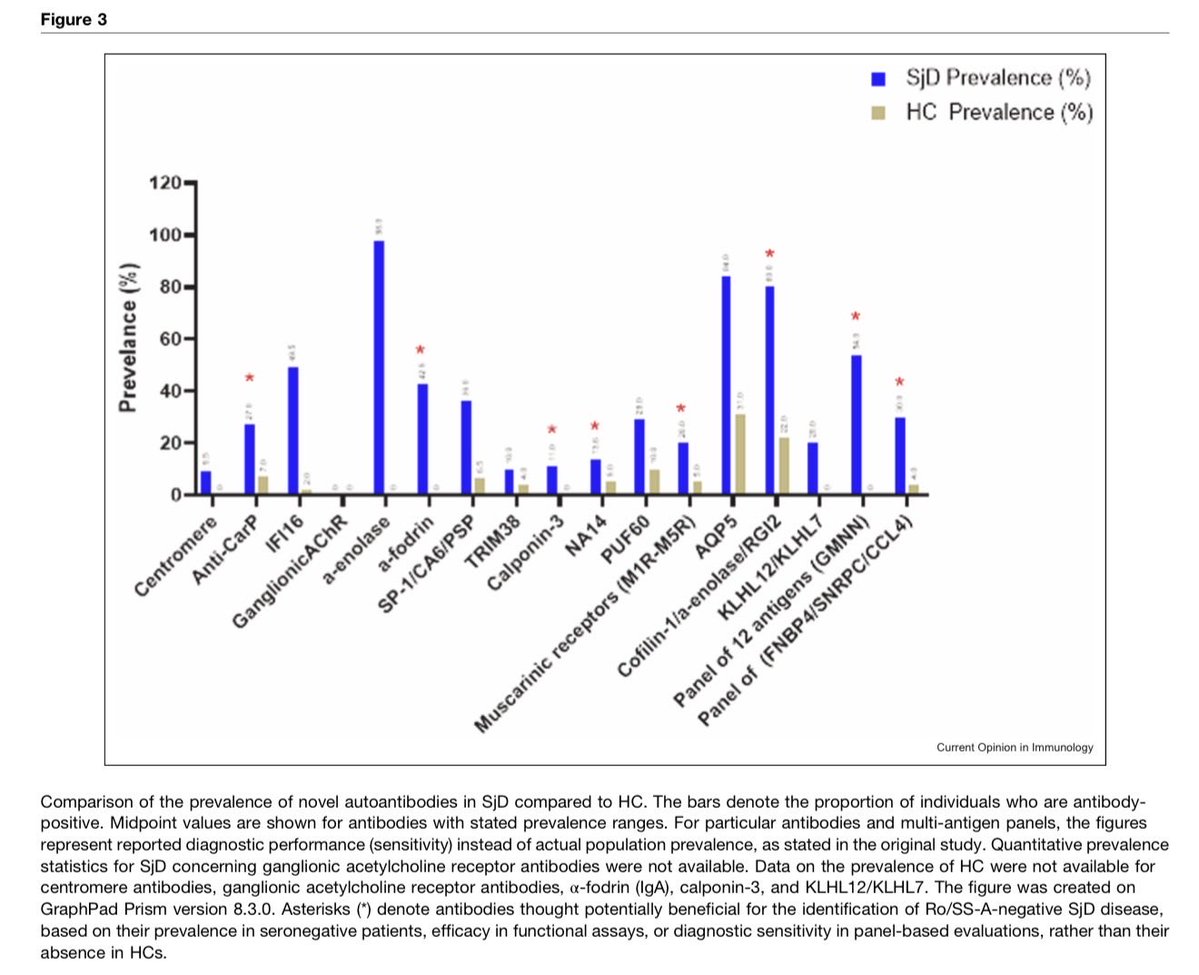
New autoantibodies in Sjögren's disease
#Rheumatology#MedTwitter These findings strongly suggest that a multi-marker panel approach is the most promising strategy for developing a new diagnostic test for seronegative SjD…
Primary heart involvement in systemic sclerosis (SSc-PHI) refers to cardiac abnormalities directly attributable to SSc, excluding those secondary to other SSc manifestations (e.g., pulmonary hypertension, interstitial lung disease, renal crisis) or unrelated conditions (e.g., ischemic heart disease). It is an important cause of mortality in SSc and accounts for ~12% of deaths in the EUSTAR cohort.
SSc-PHI may manifest as pericarditis, myocarditis, myocardial fibrosis with conduction defects, or biventricular diastolic/systolic dysfunction. Both microvascular ischaemia and myocardial inflammation contribute to perivascular and myocardial fibrosis in SSc, with an increasing recognition of the role of accelerated macrovascular disease.
Distinguishing primary from secondary cardiac involvement is often difficult due to overlapping symptoms, masked presentations, and shared abnormalities on biomarkers and imaging (e.g., pulmonary arterial hypertension and/or interstitial lung disease vs. right ventricular dysfunction or SSc-PHI).
Management requires a multidisciplinary team (rheumatologist + cardiologist experienced in SSc), however, evidence is limited (mostly small cohorts/case series). Treatment is tailored to the specific cardiac presentation, but key principles include:
◦ Controlling overall SSc disease activity
◦ Supportive care aligned with standard cardiovascular management
◦ First-line immunosuppression: mycophenolate mofetil
◦ Alternatives: tocilizumab or rituximab
◦ Frequent addition of calcium channel blockers or vasodilators
*Soo CY, Jex N, Bissell L-A, Del Galdo F, Plein S. Cardiac involvement in systemic sclerosis: mechanisms, manifestations and management. Rheumatology (Oxford). Published online February 4, 2026.
🔗https://t.co/xaxmgvYsMx











![LastManStand85's tweet photo. Azathioprine [thiopurines] ⬆️ risk of Intra-hepatic Cholestasis of pregnancy
🚩Safe but not risk free
➡️Use lowest effective dose
➡️Monitor metabolites if access [6-TGN & 6MMP ratio]
➡️Monitor for pruritus, rising bile acid, & LFTs
💊 Switch to tacrolimus if shunting or ICP https://t.co/LVMRhBkGxe](https://pbs.twimg.com/media/HCBHa6KW0Aolxma.jpg)
![LastManStand85's tweet photo. Azathioprine [thiopurines] ⬆️ risk of Intra-hepatic Cholestasis of pregnancy
🚩Safe but not risk free
➡️Use lowest effective dose
➡️Monitor metabolites if access [6-TGN & 6MMP ratio]
➡️Monitor for pruritus, rising bile acid, & LFTs
💊 Switch to tacrolimus if shunting or ICP https://t.co/LVMRhBkGxe](https://pbs.twimg.com/media/HCBHa6DW0Ak3sUq.jpg)
















![LastManStand85's tweet photo. Azathioprine [thiopurines] ⬆️ risk of Intra-hepatic Cholestasis of pregnancy
🚩Safe but not risk free
➡️Use lowest effective dose
➡️Monitor metabolites if access [6-TGN & 6MMP ratio]
➡️Monitor for pruritus, rising bile acid, & LFTs
💊 Switch to tacrolimus if shunting or ICP https://t.co/LVMRhBkGxe](https://pbs.twimg.com/media/HCBHa7WW0AAxGeK.jpg)