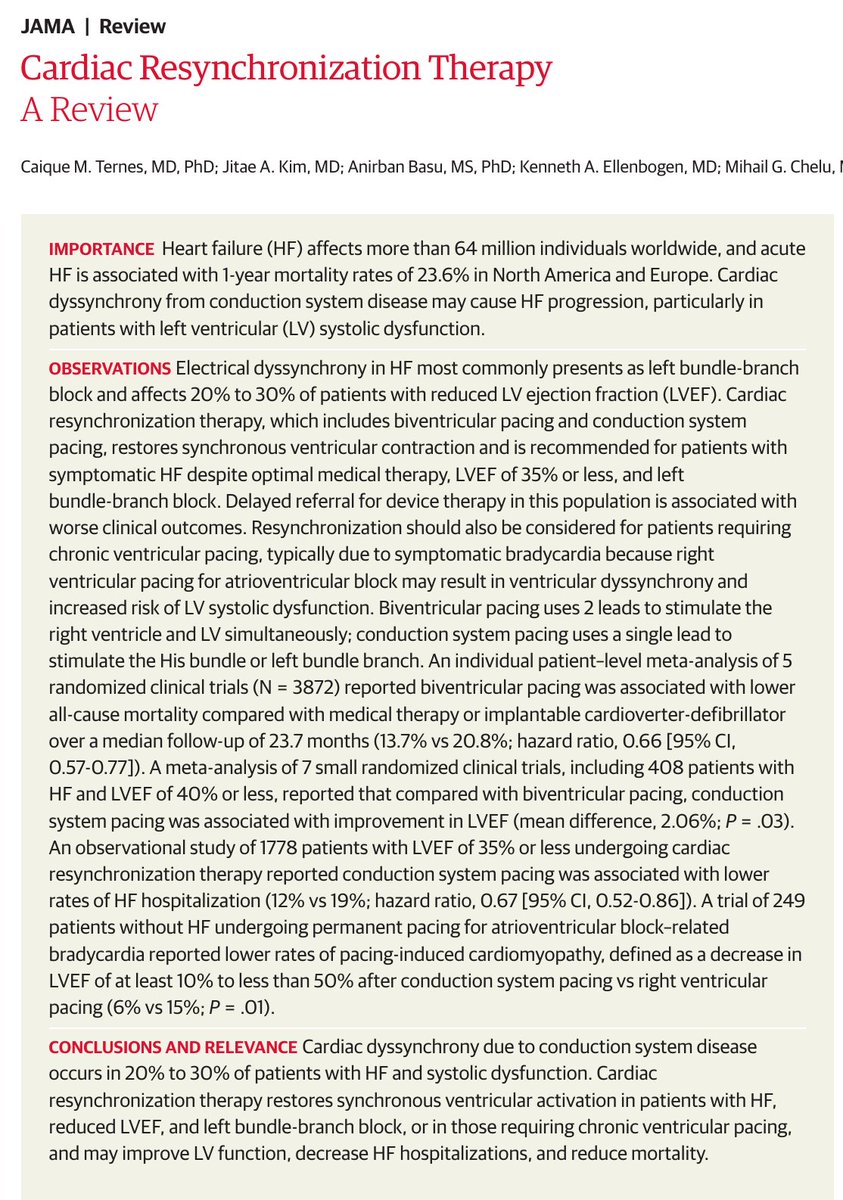
Terapia de Resincronización Cardíaca. 🫀⚡️
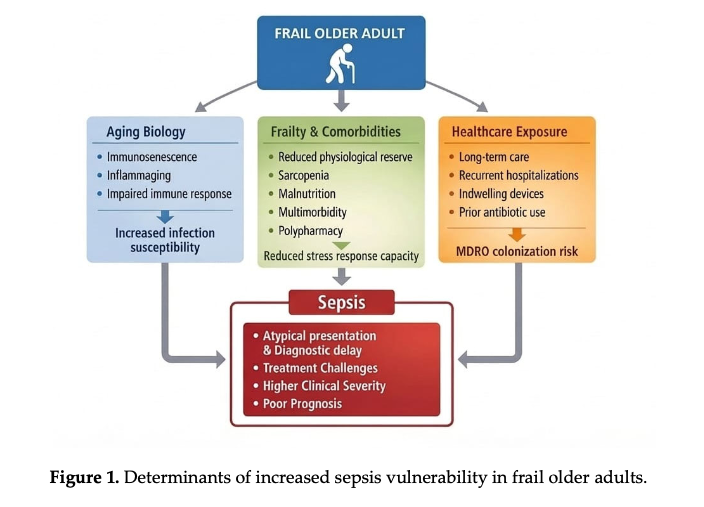
🔴La disincronía eléctrica (BRIHH) está presente en 20–30% de los pacientes con IC-FEVI reducida, y acelera la progresión de la enfermedad. La TRC restaura la activación ventricular sincrónica, algo que el tratamiento farmacológico no puede lograr. ⚡️♻️
🔴Indicaciones clave: IC sintomática pese a tratamiento óptimo + FEVI ≤35% + QRS ≥130 ms (particularmente BRIHH). También considerar en pacientes que requerirán estimulación ventricular crónica, ya que el pacing del VD puede inducir disfunción sistólica. ✍️🏻🧐⚡️
🔴Beneficio clínico sólido: ⤵️mortalidad (HR 0.66) y ⤵️hospitalizaciones por IC.
🔴Estrategias:
✔️Estimulación biventricular (estándar): efectiva, pero ~30% no responden.
✔️Estimulación del sistema de conducción (His/rama izquierda): más fisiológica, ligero ⤴️ de FEVI y ⤵️ hospitalizaciones.
🔴La referencia tardía se asocia a peores desenlaces. Complicaciones: 5–8%, principalmente relacionadas a electrodos. ⚠️💥
📜🆓️⤵️ Review 2026 @JAMANetwork
doi: 10.1001/jama.2026.4893
https://t.co/98cPKBO1N1
“Semaglutide shifts MASH therapy from glycemic control to multi-organ disease modification—but fibrosis still demands time and combination strategy.”
Semaglutide in MASH with F2–F3 Fibrosis (ESSENCE Trial Perspective)
🔬
MASH with F2–F3 fibrosis represents a critical therapeutic window, where timely intervention can prevent progression to cirrhosis, HCC, and liver-related mortality.
💉 Semaglutide: Disease-Modifying Potential
Once-weekly semaglutide 2.4 mg demonstrates true disease-modifying signals, not just metabolic improvement.
🧠 Histological Efficacy (Key Takeaway)
Semaglutide significantly increases:
Resolution of steatohepatitis without worsening fibrosis (~2/3 vs ~1/3 placebo)
≥1-stage fibrosis improvement (~1/3 vs ~1/5 placebo)
👉 Number needed to treat (NNT):
~3–4 for MASH resolution
~6–8 for fibrosis improvement
⚖️ Weight Loss: The Central Driver
Semaglutide induces ~10–11% weight loss vs ~2% with placebo, a threshold strongly linked to:
MASH resolution
Fibrosis regression
👉 ≥10% weight loss remains a biological pivot point in MASLD management.
❤️ Cardiometabolic Amplification
Semaglutide delivers multi-organ protection, including:
HbA1c reduction
Blood pressure lowering
Improved lipid profile
Reduced inflammatory markers (hs-CRP)
👉 Important: Cardiovascular disease remains the leading cause of mortality in MASLD.
🧪 Non-Invasive Markers Align with Histology
Consistent improvements seen in:
ELF score
VCTE (FibroScan stiffness)
PRO-C3
FAST score
ALT/AST
👉 This supports a future biopsy-sparing strategy in MASH monitoring.
⚙️ Mechanistic Insight (Very Important)
Semaglutide works via dual pathways:
Weight-dependent effects (dominant)
Reduced caloric intake
Improved insulin sensitivity
Reduced adipose inflammation
Weight-independent (partial)
Anti-inflammatory pathways
Gut–liver axis modulation
👉 However:
GLP-1 receptors are not expressed in hepatocytes, suggesting indirect hepatic benefits.
⚠️ Fibrosis: The Hard Endpoint
Fibrosis improvement is:
Slower and less weight-dependent
Likely requires longer duration and targeted antifibrotic pathways
👉 Cirrhosis (F4) shows limited reversibility with semaglutide alone.
🛡️ Safety Profile
GI side effects (nausea, vomiting) are common but transient
No major hepatotoxicity signal
Similar serious adverse events vs placebo
👉 Caution:
Gallbladder disease
Rare pancreatitis
🔄 Therapeutic Positioning
Semaglutide is best suited for:
Obese / T2DM phenotype MASH (commonest in India)
High cardiometabolic risk patients
🔬 Future Strategy: Combination Therapy
Semaglutide (systemic metabolic drug) + Resmetirom (liver-directed THR-β agonist) offers:
Upstream metabolic unloading + direct hepatic antifibrotic action
👉 Likely future paradigm:
Multi-target therapy for MASLD
❗ Clinical Gaps
Long-term outcomes (cirrhosis, HCC, mortality) not yet confirmed
Limited data in:
Lean MASH
Diverse ethnic populations
Need for omics-based patient stratification
🔴 CME INDIA key point
“Semaglutide shifts MASH therapy from glycemic control to multi-organ disease modification—but fibrosis still demands time and combination strategy.”
📚 Key Reference
Pirola CJ, Sookoian S. Semaglutide in MASH with F2–F3 fibrosis: ESSENCE phase 3 perspective. Metab Target Organ Damage. 2026.
https://t.co/KG024CiBtF
MASLD in elderly is not just fatty liver—it is a frailty–metabolic–cardiovascular syndrome where fibrosis and function matter more than fat.
Ageing Liver & MASLD (BMJ Frontline Gastroenterology 2026)
MASLD now affects ~25% adults, and burden is rising sharply in ≥65 years, with distinct phenotype compared to younger patients.
Elderly MASLD is a “multimorbidity disease”—frequently coexists with CVD, T2DM, sarcopenia, frailty, making outcomes more severe despite slower disease kinetics.
Pathophysiology is age-driven:
Telomere shortening, mitochondrial dysfunction, impaired autophagy, epigenetic drift → accelerated fibrosis and HCC risk.
Sarcopenia + visceral adiposity (sarcopenic obesity) is a key driver of adverse outcomes—not BMI alone.
Diagnosis is tricky in elderly:
Normal ALT is common even in advanced disease → do not rely on transaminases.
FIB-4 overestimates fibrosis in elderly → use age-adjusted cut-off (<2.0 = low risk in ≥65 yrs).
Best practical approach (Primary care):
FIB-4 → Elastography → Hepatology referral if high risk.
Fibrosis stage—not steatosis—is the strongest predictor of mortality, with exponential rise in risk from F2 onwards.
CVD is the leading cause of death in MASLD, exceeding liver-related mortality.
HCC risk increases with age, even without cirrhosis in selected patients—questioning current surveillance thresholds.
Lifestyle remains cornerstone, but in elderly:
Avoid aggressive weight loss → risk of malnutrition + muscle loss.
Target strategy in elderly MASLD:
Moderate weight loss + high-protein diet + resistance training to preserve lean mass.
Exercise is disease-modifying:
+2500 steps/day → ~47% reduction in MASLD risk.
Emerging therapies:
Resmetirom and GLP-1 RAs show promise, but elderly underrepresented in trials → evidence gap.
Key Clinical Insight:
“Younger patients lose more life-years, but elderly patients have higher event severity due to frailty and comorbidity load.”
@C_V_Schneider@schattenbergJ@PhilSmithIsBack@OTavabie@dr_aditi_kumar@TrevorTabone@eathar_s@IrenePerezMD@KGananandan@zare_benjamin@medicalreg@dtleiberman@BASLedu@BSGtrainees@ulstergastro #GITwitter #GIX
https://t.co/cgH6vTJFUH
Time to Measure
In primary aldosteronism, chasing renin may mislead—Angiotensin II tells the real story
Angiotensin II Measurement in Primary Aldosteronism Screening
Core Concept
Primary aldosteronism (PA) is a renin-suppressed, aldosterone-driven state, but Angiotensin II (Ang II) is the true proximal driver of aldosterone secretion, not renin itself.
Why Renin Alone Is Inadequate
Plasma renin is not a direct surrogate for Ang II levels due to downstream enzymatic modulation (ACE, degradation pathways).
Discordance exists:
→ Renin may be low/high, but Ang II may not parallel it
Therefore, ARR (aldosterone–renin ratio) can misclassify physiology in selected patients.
Pathophysiological Insight
Angiotensin II directly stimulates zona glomerulosa → aldosterone secretion
Additional modulators:
→ ↑ K⁺, ACTH, adipokines (positive)
→ ANP, ↓ K⁺ (negative)
Thus, aldosterone regulation is multifactorial—not renin dependent alone
Key Paradigm Shift
Traditional model:
→ Renin → Ang I → Ang II → Aldosterone
Emerging insight:
→ Measuring Ang II provides a closer estimate of aldosterone drive than renin
Clinical Implication
In suspected PA:
ARR remains first-line screening tool
But consider Ang II when:
Discordant ARR results
Atypical physiology (e.g., CKD, ACE variability, medications)
Unexplained aldosterone excess despite low/normal renin
Timing Matters (Practical Pearls)
Hormonal assays (renin, aldosterone ± Ang II):
Morning sampling preferred (8–10 AM)
Patient ambulant ≥2 hours, seated 5–15 min before sampling
Ensure:
Normal potassium
Liberal salt intake
Drug interference minimized
Why Angiotensin II Measurement Matters Now
Advances in mass spectrometry-based peptide assays allow accurate Ang II quantification
Helps distinguish:
True autonomous aldosterone secretion (PA)
vs
RAAS-driven secondary hyperaldosteronism
CME INDIA – Takeaways
Renin ≠ Ang II → do not equate physiology blindly
Ang II is the real effector hormone in aldosterone regulation
ARR is screening—not pathophysiology
Consider Ang II measurement in complex or discordant cases
Standardize timing, posture, and biochemical conditions before testing
Tagline
➡️ “In primary aldosteronism, chasing renin may mislead—Angiotensin II tells the real story.”
https://t.co/3VCJ89HNv1