An important paper in the next chapter of orchestrating the complex machinery of our immune system is the B cell and the immense diversity of antibodies. The paper describing this next step will be published in June and I will then commentate dots as to why IL-15 is the backbone to this orchestration..from NK cells, to T cells, to memory T cells and now to B cells and memory Antibodies. The Nant quest of understanding the complex immune system ..30+ years and still learning!
If you missed the FDA hearing about the Commissioner’s National Priority Voucher Program where @LoriMills4CA42 I gave comments, here is what I said:
Good afternoon, distinguished panelists and members of the FDA. As Henry Ford said: “We need a faster horse.”
My name is Karol Hansen. I am a Stage IV breast cancer patient with Mets to the bones. I have been fighting cancer for 10 years. In that time, I have undergone chemotherapy twice, radiation three times, and more than 25 surgeries. The cancer has recurred over 11 times.
10 years ago, Nuelasta was prescribed to me before I even had neutropenia because it’s medically known that chemotherapy causes Netropenia. Neutrophils are an inherent part of the body’s immune system that provide rapid, broad, innate protection against infection and injury. Lymphocytes form the core of the adaptive immune system and are responsible for precise, targeted and long-lasting immunity.
Neulasta, and its biosimilars, is given prophylactically to protect neutrophils. ANK TIVA, manufactured by Immunity Bio in California protects lymphocytes, but it is NOT YET approved by the FDA for all cancer types.
During these years of relentless treatment my Absolute Lymphocyte Count remains critically low — below the threshold associated with increased infections, weakness, treatment failure, and shortened survival. There are millions of cancer patients whose ALC looks just like mine. RIGHT NOW, at the Chan Soon-Shiong Institute for Medicine there are 15,000 patients waiting in line to receive ANK TIVA.
ANK TIVA is the first therapy designed to restore and activate lymphocytes through its IL-15 mechanism. It is the missing piece of immune boosting protection — ANK TIVA is the equivalent to lymphocytes as Neulasta is to neutrophils.
I have intractable, treatment-resistant cancer that has failed standard therapies. If ANK TIVA had been available as standard supportive care a decade ago, I might have been spared years of immune collapse, repeated recurrences, and the physical and emotional toll of more than 25 surgeries. Now I am out of time, out of strength and out of options. The 15,000 patients waiting for ANK TIVA can only get it if an opening is available in a narrow group of clinical trials or through the Extended Access Program, which the clinic has to process one at a time, on a case by case basis. A VERY SLOW process. It took almost a year for me to get approved. That’s not POLITICS, that’s imminent death for critically ill patients.
Ladies and gentlemen, we HAVE the cart, which is ANK TIVA. But, as Henry Ford said, “WE NEED A FASTER HORSE!” The Commissioner’s National Priority Voucher Program IS THAT FASTER HORSE!
Immunity Bio is delivering groundbreaking immune-restoring therapy of ANK TIVA but the FDA needs to approve it as a first line of defense for patients with lymphopenia.
The CNPV Program was created to accelerate exactly these kinds of innovative therapies that address critical unmet needs and can transform patient outcomes. I urge the FDA to prioritize ANK TIVA for full approval and label expansion so that every cancer patient undergoing chemotherapy or radiation can receive lymphocyte support proactively — not as a desperate final measure after years of fighting for survival.
It is TIME for a faster horse at the FDA. Streamline the review process. Provide a patient conduit directly to CNPV. Give us a voice. Speed up access to ANK TIVA. Give future patients the CHANCE at a fuller life that I, and others who have died while waiting, have been denied.
Thank you for listening to my story and for the work you do every day on behalf of patients like me
Radical cystectomy ( surgical removal of the bladder ) - The largest complication in all surgeries even more than pancreatectomies ( Whipple) which I used to do!
Imagine if we can avoid this surgery .
So what is next on the NantWorks platform as we emerge from 15 years of stealth. Remember Diabetes? Remember Abraxane..albumin bound paclitaxel. Well imagine Albumin linked GLIP-1 at one tenth of the dose? This is the program now nearing completion at Nantworks and trials completed ex -USA. Will share news over the next 6 months
Dr. Patrick Soon-Shiong just revealed that 52 million Americans reportedly have low T cell counts.
And he warns having low T cells can double your risk of early death.
“52 million Americans have low T cells.”
“If you have low T cells, they showed statistically that it's below 1500.”
“If it’s below 1000, the risk of dying earlier is two times.”
“This is profound.”
“If your T cells are low … you have a risk of dying earlier.”
“Whether you’re without disease or whether you have cancer.”
@DrPatrick
As predicted in our Nant Cancer vaccine patent. Most excited to see the readout of the Lynch Syndrome trial to prevent cancer. 2 year follow up coming by next year. NK cell stimulation happening so far.
Dear Dr. Pat, @DrPatrick
Thank you for your tireless dedication and unwavering commitment to cancer patients. Your relentless quest to find a cure and deliver innovative therapies like ANKTIVA brings real hope to those who need it most.
We are deeply grateful for your visionary leadership and the difference you continue to make in the fight against cancer.
If you’re reading this, I invite you to join me in supporting Dr. Pat and ImmunityBio $IBRX on this important journey.
With sincere appreciation,
BullishBruk
@LoriMills4CA42
$IBRX Imagine you love someone with high-grade papillary bladder cancer that came back after BCG. They were told the next step was to take out the bladder. They went looking for anything else they could try. Last week they came across a drug, ANKTIVA, that the FDA approved in 2024 for the closely related form of the same disease, but not yet for theirs. They asked their urologist whether it could be used. The urologist said they were waiting to see what the FDA was going to do.
This Tuesday, the FDA answered.
WHAT THE LETTER SAID
On May 19, 2026, the FDA accepted ImmunityBio's supplemental Biologics License Application for ANKTIVA in combination with BCG, for BCG-unresponsive high-grade papillary-only non-muscle-invasive bladder cancer.
The action date the FDA committed to, the day by which it will issue its final decision, is January 6, 2027.
THE SIXTY DAYS THAT BECAME SEVENTY-ONE
The same application was turned away last year. The FDA refused to file it.
The company met with the FDA in January 2026 and was told what additional information was needed. No new clinical trials. A written submission detailing the overlapping features of papillary disease and CIS. The company submitted it. On March 9, 2026 the FDA acknowledged receipt, and the formal sixty-day filing-review clock started.
Sixty days from March 9 is May 8.
May 8 came and went. So did May 9, 10, 11, 12, 13, 14, 15.
On Saturday, May 16, at the American Urological Association Annual Meeting, the company's founder stood on a stage and said, into a microphone: "The 60 days have passed. We've not heard anything from the FDA. We're awaiting some response. I'm hopeful."
Three days later, on Tuesday, the response came.
Seventy-one days from receipt. Eleven days past the formal window. And then accepted.
ACCEPTED IS NOT APPROVED
Accepted means the FDA looked at the resubmitted application, decided it was complete enough to review on the merits, and started the formal clock. The decision comes in January 2027.
Between now and then the FDA reviews the application, may ask further questions, may convene advisory panels, may extend its own timeline. None of that has happened yet. This week, only one thing happened. The door opened.
But the door opening matters.
THE PAPER ANYONE CAN READ
The trial behind this application is QUILT-3.032 (NCT03022825). Its papillary-only cohort, Cohort B, was published in the Journal of Urology in January 2026, peer-reviewed and Open Access. The lead author is Sam S. Chang at Vanderbilt.
That is unusual for a binary regulatory event. Most of the time, the data on the FDA's desk is summarized through press releases and conference slides while the peer-reviewed publication lags by months or years. Here, the peer-reviewed publication landed first. The FDA is reading the same paper a patient's spouse can read tonight.
The link: https://t.co/E6Fma7y4Fu.
From the paper, with a data cutoff of July 15, 2024:
- Disease-free survival at 12 months: 58.2% (95% CI 46.6, 68.2)
- DFS at 24 months: 52.1% (CI 40.3, 62.7)
- DFS at 36 months: 38.2% (CI 25.6, 50.6)
- Progression-free survival at 12 months: 94.9% (CI 86.9, 98.0)
- PFS at 36 months: 83.1% (CI 69.5, 91.0)
- Disease-specific survival at 12 months: 98.7% (CI 91.4, 99.8)
- DSS at 36 months: 96.0% (CI 88.2, 98.7); median not reached
- Cystectomy avoidance at 12 months: 92.2% (CI 83.4, 96.4)
- Cystectomy avoidance at 36 months: 81.8% (CI 68.1, 90.1); median time to cystectomy not reached
- Treatment-related adverse events: 61% Grade 1 to 2; 3% Grade 3; no Grade 4 or 5
In plain English. Disease-free survival measures whether the cancer comes back at all, including in non-aggressive forms. About six in ten patients had no return of any kind at one year. By three years that has fallen to roughly four in ten, which sounds modest. The next three lines are the ones that change a patient's life.
Progression-free survival measures whether the cancer becomes muscle-invasive, the stage at which the bladder has to be removed or the disease becomes lethal. At one year, nineteen out of twenty patients had kept the cancer in the bladder lining, where it was still treatable. At three years, that was true for more than four out of five.
Disease-specific survival measures whether the bladder cancer kills you. At three years, ninety-six out of a hundred patients were still alive from this disease. The median, the point at which half the patients have died, has not been reached. The statisticians cannot yet draw the line.
And cystectomy avoidance, the line that means the patient still has a bladder: more than four out of five at three years. The median time to cystectomy, the point at which half had needed the operation, has not been reached either. They still have their bladders.
These are not press-release marketing numbers. They are the numbers in a peer-reviewed paper, downloadable as a PDF, sitting under a DOI.
The patients were told to lose their bladders.
Most still have them.
WHAT THE FDA WROTE ABOUT THE REVIEW
The FDA did not just accept the application. The acceptance letter, summarized in the company's press release on Tuesday, said two things.
The first set the review focus. The company quoted the FDA verbatim:
"The scientific data detailing these overlapping features will be the focus of the review of this sBLA to determine if there is adequate justification to allow for such an extrapolation and expansion of the indication of Anktiva with BCG to include the treatment of patients with BCG-unresponsive NMIBC with papillary tumors."
The FDA committed to spend the months between now and January 6 on the exact question the workshop spent Monday answering.
The second the company described in its own narrative prose, attached to the first by the word "while." Per the press release, the FDA reiterated its concerns relating to single-arm trials in papillary disease alone (Cohort B), given that the initial indication for CIS and papillary disease (Cohort A) has already been approved on a single-arm trial.
That second statement, even in the company's paraphrase, is the most interesting thing about the letter.
The concern, as reported, is that Cohort B was a single-arm trial. Patients received ANKTIVA plus BCG; their outcomes are reported; there is no randomized control arm receiving a different therapy for comparison. The FDA has historically preferred randomized controlled trials.
But the FDA approved Cohort A, CIS with or without papillary disease, from the same QUILT-3.032 trial, on the basis of a single-arm result in April 2024.
The exact methodology the FDA is reported to be reiterating concerns about is the methodology the FDA itself accepted as adequate two years ago, for the closely adjacent indication, in this same disease.
The review will turn on whether what was acceptable for one face of the disease is acceptable for the other.
WHAT THE FDA HAS ALREADY APPROVED
The FDA has approved five drugs for BCG-unresponsive non-muscle-invasive bladder cancer in the last twenty-seven years. All five were approved on single-arm trials.
- Valrubicin, 1998. Single-arm Phase 2 in 90 patients.
- Pembrolizumab, January 2020. KEYNOTE-057, single-arm Phase 2 in 96 evaluable patients. The advisory committee voted nine to four in favor.
- Nadofaragene firadenovec, December 2022. Single-arm in 98 evaluable patients.
- ANKTIVA's Cohort A, April 2024. The same QUILT-3.032 single-arm design, 77 patients.
- TAR-200, 2025. SunRISe-1 Cohort 2, single-arm Phase 2b in 85 patients.
In 2018, the FDA published its own guidance on developing drugs for BCG-unresponsive NMIBC. The guidance states, in writing, that a single-arm trial design is appropriate in this disease for patients with no standard therapy other than cystectomy. The FDA wrote the rule. The FDA then approved five drugs under it.
There is precedent outside this disease as well. In May 2017, the FDA granted the first-ever tissue-agnostic cancer approval to Merck's Keytruda (pembrolizumab) on the basis of 149 patients across five single-arm trials covering fifteen tumor types.
ANKTIVA's Cohort B sBLA uses the same single-arm methodology, in a population the FDA's own letter describes as having overlapping clinical and non-clinical profile with the indication already approved. Eighty patients. Three years of published peer-reviewed follow-up.
WHAT HAPPENED MONDAY
The day before the acceptance, on Monday May 18, the FDA's Oncology Center of Excellence convened a public workshop on non-muscle-invasive bladder cancer.
The first panel asked, on the record, whether CIS and papillary disease are the same disease.
The panel concluded they probably are. Different anatomical presentations of one biological process. A urologist on the panel testified that about one in twenty US urologists routinely use blue-light cystoscopy, which means CIS is missed at the initial diagnosis in most cases when it is there. Several panelists testified that when they treat high-grade papillary disease, they treat it the same way regardless of whether CIS is found alongside it. Because the FDA has not yet approved any therapy specifically for papillary-only BCG-unresponsive disease, urologists routinely use therapies labeled for CIS off-label in this setting, because what else is there.
ImmunityBio's own acceptance press release the next day restated the workshop conclusion in nearly the same language: that CIS and papillary disease "arise from the same cancer inducing clone, is therefore the same disease." The company's submission, the panelists' testimony, and the FDA's filing letter about "overlapping features" of the two presentations all converge on the same sentence.
That is the answer to the exact question the FDA's review will turn on.
It was on the record at the FDA the day before the FDA accepted the file.
The workshop happened on Monday.
The letter went out on Tuesday.
The timing is not a coincidence and was never supposed to be.
WHAT WAS ALREADY IN PLACE
While the application sat at the FDA, several other pieces had been locking into place around it.
The National Comprehensive Cancer Network added ANKTIVA plus BCG for BCG-unresponsive papillary-only NMIBC to its bladder cancer Clinical Practice Guideline as a Category 2A recommendation in March 2026. The NCCN's Drugs and Biologics Compendium, the publication that the Centers for Medicare and Medicaid Services consults under §1861(t)(2)(B)(ii)(I) of the Social Security Act, tracks the Guideline. The statutory pathway to Medicare coverage for off-label use was already open before the FDA accepted the file.
The United Kingdom's Medicines and Healthcare products Regulatory Agency approved ANKTIVA plus BCG for BCG-unresponsive CIS in July 2025. The European Medicines Agency followed in February 2026. International regulators had already decided the data was strong enough for the closely related indication.
On Monday, the day of the workshop, ImmunityBio also disclosed a US patent estate of five issued and one pending patent, with coverage extending through 2035, written to apply to any FDA-approved BCG strain rather than to a single supplier. The same day, a separate SEC 8-K disclosed an exclusive ten-year US supply agreement for the Japanese BCG-Tokyo-172 strain, structured with no payment due to the supplier until FDA approval of the combination. The US BCG supply has been served by a single FDA-approved strain, rationed since 2019; adding a second strain matters.
None of those pieces are the trial data. None of them substitute for FDA approval. But all of them are the pieces you would put in place if you were preparing for the moment a regulator opened the door.
WHAT JANUARY 6 MEANS
It does not mean approval. It means the day by which the FDA has committed to issue its decision, and the decision can be one of several: approve, approve with restrictions, issue a Complete Response Letter requiring further work, extend the timeline. The decision lands on or before that day.
It also does not mean a fast decision. From the FDA's receipt of the application on March 9 to the action date on January 6 is about ten months, the Standard Review goal for an efficacy supplement. Priority Review would have been six. The FDA, by the calendar, did not expedite.
For the patient whose spouse read about ANKTIVA last week, whose disease is high-grade papillary-only and whose next medical step is removal of the bladder, January 6 is not the end of the wait. It is the new shape of the wait. There is now a calendar date, set by the FDA itself, by which the FDA has committed to answer.
There was no such date on Monday.
There is one now.
THE LETTER
The letter came on Tuesday.
The patients in the paper were told to lose their bladders. Most still have them.
January 6 is the day the FDA decides who else gets to keep theirs.
Congratulations to @DrPatrick, the entire @ImmunityBio team, patients, advocates, and long-term $IBRX investors.
After months of short-driven fear around a potential RTF, FDA has officially ACCEPTED the ANKTIVA + BCG label expansion sBLA and assigned a Jan. 6, 2027 PDUFA date.
A major regulatory milestone and an important step toward expanding treatment options for patients with papillary NMIBC. Now the focus shifts to approval.
Onward and upward.
https://t.co/g05V4Zg2D8
It is OFFICIAL! 🙌
A massive shoutout and huge praise to the dedicated reviewers at @FDAOncology — our Heroes and Sheroes of the Day!
Thank you for your hard work, thorough science, and commitment to getting this done right for patients. $IBRX
You’ve earned every bit of this recognition! 🚀 @LoriMills4CA42@DrPatrick
$IBRX Tomorrow marks the day. All issues related to the FDA workshop have been resolved. The supplemental BCG naïve BLA submission remains on schedule for 2026.
$IBRX — Dr. Pat just delivered another masterclass! IL-15 ALC….explained perfectly.
One of the best presentations I’ve seen.
If you haven’t watched it yet… drop everything and go listen. This is big. 🚀 https://t.co/us6f4vcLTd
Dear Mr. @joerogan@joeroganhq@JamieVernon
Below is a copy of the email I sent to you. For ease and social media reference, I will also post a similar message here.
Doctor Patrick Soon-Shiong is a contact of mine and I broached the idea of him going on your show in the similar manner as when @seanspicer and @ChrisCuomo hosted Dr. Patrick.
If you would like to reach out to him directly, I will include his X contact here, and you may follow each other (@DrPatrick). Otherwise, please see my email attached and I hope you could consider his life-long work and efforts to not only treat and beat cancer, but also treat a wide range of immuno suppressed ailments, such as Lymphopenia, Sepsis, HIV and Covid.
I appreciate any efforts to advance this matter forward, as it is a matter that affects all of humankind in the most beneficial of ways - by granting improved health and additional life!
Thank you for your attention to this matter!
BR,
The Macro Ghost
For reference and ease, here are the podcasts also listed in the email.
1) Spicer: https://t.co/z33hgLVIT8
2) Cuomo: https://t.co/OZ4pvBOZEq
2a) Cuomo short: https://t.co/MrwesecCzP
2b) Cuomo short: https://t.co/7uG6J7MAeJ
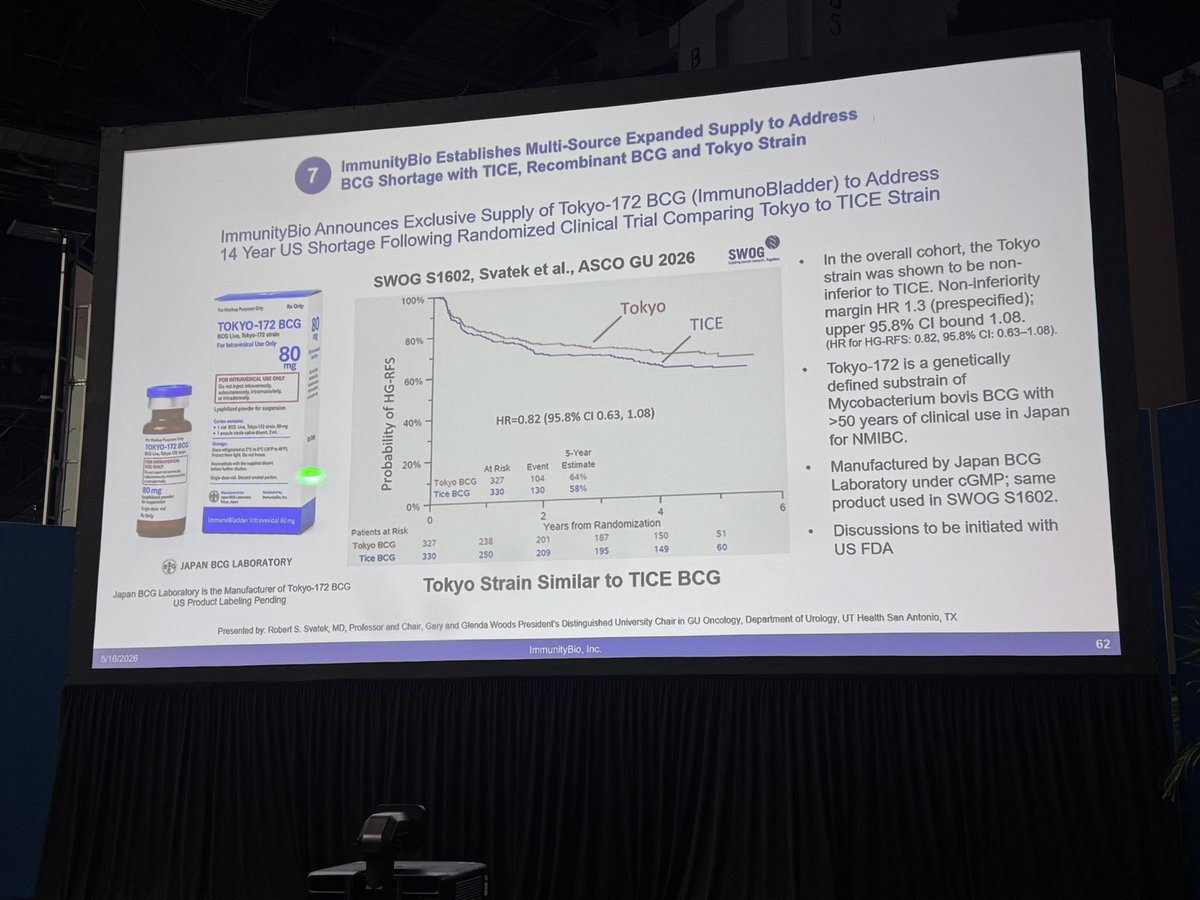
ImmunityBio Announces Exclusive Supply of Tokyo-172 BCG (ImmunoBladder) to Address 14 Year US Shortage Following Randomized Clinical Trial Comparing Tokyo to TICE Strain.
Learn more here: https://t.co/FAhapwwDmk
@DrPatrick#AUA26
ImmunityBio has announced an exclusive U.S. Development and Supply Agreement with Japan BCG Laboratory for the development and commercialization of Tokyo strain BCG in the U.S.
Today's announcement marks a notable step forward in addressing the ongoing BCG shortage that has impacted urologists and bladder cancer patients for more than a decade.
Learn more: https://t.co/99wRn8gns0
The year of the fire horse. Now in Italy and inspecting our Ai driven robot nearing completion and a stainless steel horse in the lobby. A good sign of what is to come!! World Bank of NK cells.