"Statin Drugs Have Not Saved Millions Of Lives."
Dr. Jack Wolfson, Cardiologist
"Statins Have Actually Killed Millions Of People."
Low Cholesterol causes 3X increase in brain bleed Strokes.
Every 30 mg decrease in Cholesterol causes a 22% higher risk of death from all causes...
Documented Peer Reviewed Data Shows:
When LDL decreases below 70 mg/dL, hemorrhagic strokes (brain bleeds) increase 3 fold.
The Minnesota Coronary Experiment showed that for every 30 mg/dL (0.78 mmol/L) decrease in serum cholesterol is linked with 22% higher risk of death from any cause.
When total cholesterol is chemically lowered below 180 mg/dL the rate of cancer & dementia increases dramatically.
And when total cholesterol stays under 150 mg/dL, chronic illnesses like cancer & autoimmune diseases strike.
36% of those on statin therapy will be diagnosed with new onset type 2 diabetes.
Research has confirmed over & over that the higher your LDL the longer you live. LDL is a transport molecule for cholesterol & a vital immune system regulator. Lowering LDL thru statin drugs has deadly & deleterious effects.
Vibrant Health Can Start To Be Attained When:
Total Cholesterol is at minimum 200 mg/dL corresponding to a cholesterol level of 5.2 mmol/L in non US countries. Normal total cholesterol in 1960 was 300-350 mg/dL.
Lowering cholesterol does not lower Cardiovascular risk or disease. Saturated fat & cholesterol have no effect on CVD outcomes, including heart attacks, strokes, CVD mortality & total mortality.
There Are No Benefits To Cholesterol Lowering Statin Therapy..Only Risks & Side Effects:
Alzheimer's Disease
Cancer
Pancreatitis
Liver Damage
Diabetes
Depression/Suicidality
Lupus
Parkinson's Disease
ALS (Lou Gehrig's Disease)
Hormonal Deficiency
Brain Damage
Multiple Sclerosis
Muscle Pain & Tearing
Severe Weakness
Neuropathy
Heart Failure
Vertigo
Cognitive Impairment
Dementia
In 1971, a Japanese microbiologist called Akira Endo isolated a compound from a mould called Penicillium citrinum that inhibited the enzyme the human body uses to manufacture cholesterol.
That discovery became the statin class of drugs.
Merck released the first commercial statin in 1987. Cholesterol was, at the time, considered the central villain in cardiovascular disease. Lower the cholesterol, the theory said, and you lowered the risk of heart attack.
What followed was one of the largest pharmaceutical campaigns in history.
The threshold for "high" cholesterol was steadily lowered. In 1984 the cut-off was 240 mg/dL. By 2001 it was 200. By 2013 the American Heart Association had effectively abandoned a numerical threshold altogether and recommended statins for any patient with a ten-year cardiovascular risk above 7.5 percent, which captured roughly a third of American adults over forty.
Lipitor became the single best-selling pharmaceutical product in history. By the time it came off patent in 2011, it had generated approximately one hundred and forty-eight billion dollars in revenue for Pfizer.
The clinical result was less impressive than the financial one.
The most generous meta-analyses of statin trials in primary prevention, the patients who have not yet had a heart attack, show an absolute risk reduction in major cardiovascular events of approximately one to two percent over five years. The "twenty-five percent relative risk reduction" you see on the marketing material is the same couple of percentage points, expressed in a way that sounds bigger.
Mortality benefit in primary prevention is statistically insignificant in most of the major trials. People taking statins for prevention die at roughly the same rate as people not taking them. They simply die of different things.
The side-effect profile includes muscle pain in five to twenty percent of users, cognitive symptoms, increased risk of type 2 diabetes, and a long-running clinical debate about coenzyme Q10 depletion, which is downstream of the same enzyme the drug inhibits.
The drugs are mildly useful in secondary prevention and of debatable value in primary prevention. The pharmaceutical industry, the cardiology associations, and the medical-school curriculum have not significantly updated their recommendations to reflect this.
The reason is structural rather than scientific.
A pharmaceutical industry that generates billions from a class of drugs cannot dispassionately reconsider whether the drugs work. The cardiology associations funded by that industry cannot dispassionately reconsider the guidelines they helped author. The journals funded by its advertising cannot dispassionately publish papers questioning the products on the opposite page.
The question the system was built around was: how do we lower cholesterol.
The question that was never asked, because asking it would have unwound the entire structure, is the more important one.
Does lowering cholesterol actually extend human life.
The answer, across forty years of trials, is "marginally, in some populations, with caveats, and with side effects".
The marketing has been "yes, take this every day for the rest of your life".
The two answers are not the same answer.
One of them paid for an awful lot of glass-walled cardiology departments.
In 2015, three Danish clinical pharmacologists published a paper in BMJ Open.
They did something very boring. They took every placebo-controlled statin trial of more than a thousand patients, plotted the survival curves of the treatment group against the placebo group, and measured the gap.
Not the relative risk reduction. Not the hazard ratio. Not any of the elegant statistical gymnastics the industry prefers.
The actual gap. In days. On average. Within the running time of the trials.
For primary prevention, meaning healthy people with no heart disease taking the drug to prevent something that hadn't happened yet, the median postponement of death was 3.2 days.
For secondary prevention, meaning people who had already had a cardiac event, 4.1 days.
Read those numbers slowly.
Three days. Four days.
That is what you are being sold when they say a statin will reduce your risk by twenty-five percent.
Twenty-five percent of a small thing, spread across thousands of people, averaged over five years of daily pill-taking, amounts to the difference between dying on a Tuesday and dying on the Friday of the same week.
Some patients in the trial range got twenty-seven extra days. Some got negative days. Meaning they died sooner on the drug than they would have without it.
The median of the middle. Three days.
If a plumber told you he could fix your leak by reducing the drip rate by twenty-five percent and the fix cost you twenty pounds a month forever, you would ask for a real number.
The real number is on file at the BMJ.
You will not hear it in the consulting room.
I’m posting this again because we have gained lots of new followers and they may have missed this one.
But this statin post is so shocking. I think everyone needs to view it and share it to all their loved ones. You can read all the science studies.
This drug should be banned, and people should be held accountable
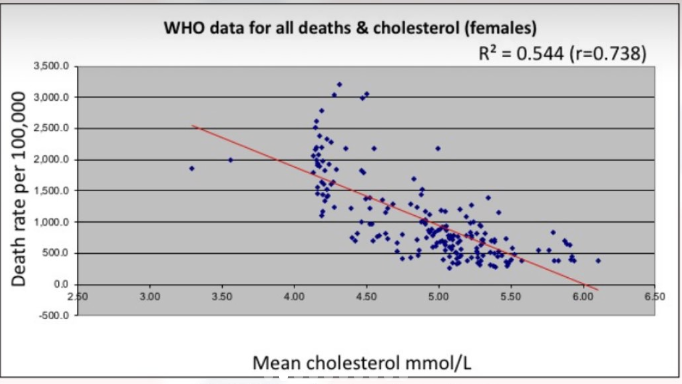
192 countries were studied and cholesterol was NEGATIVELY associated with death rate...
the higher the cholesterol, the lower the death rate
why is nobody talking about this?
To sell statins, we're told cholesterol damages arteries—in reality, it repairs arterial injury. Statins hence don't prevent death and give 20% of users muscle, liver or nerve damage.
Here I show what doctors never tell you about statins and heart disease
https://t.co/I1oBgpxKeR
Lipids simplified!
🧱 Cholesterol – is the material needed for building cell walls, making hormones etc
🛻 Lipoproteins - are basically Trucks transporting Cholesterol along with other things through blood. Depending on size they are of many types.
⛽ Triglycerides – are portable Fuel containers that trucks are carrying along.
🚛 HDL – They are the Recycling Trucks the patrol the roads collecting leftover cholesterol bricks from tissues & arteries, & bringing it back to the liver’s recycling center. HDL- C in your reports is the total leftover bricks in circulation currently.
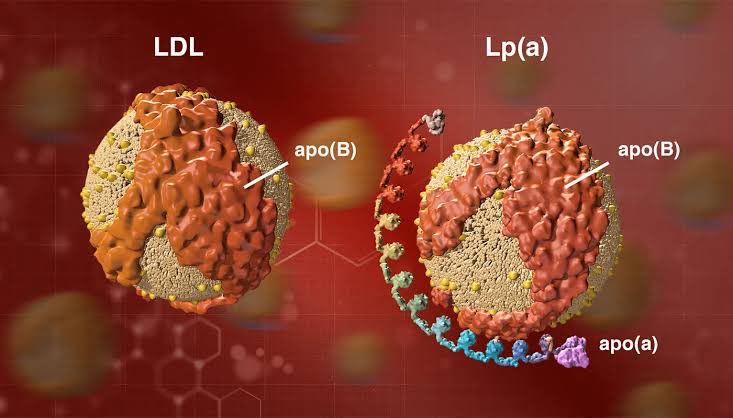
🚚 LDL – They are the Delivery Trucks that deliver cholesterol bricks from the liver warehouse to construction sites (cells) around the body. LDL- C in your reports is the total unused bricks in circulation currently.
🚨 Lp(a) - Some of these LDL delivery trucks have an extra problem. They are wheel that are extra sticky.
🚛📦 VLDL – They are the Fat Cargo Trucks that mainly transports big boxes of triglycerides (fat) from the liver to storage sites.
🪪♦️ApoB (Apolipoprotein B) - All the main delivery trucks (LDL, Lpa, VLDL..) have a common license plate called ApoB. Counting them gives an idea of the no of trucks on road currently. More means too many cholesterol bricks & extra fuel (Tg) are being transported
🪪🔹ApoA1 (Apolipoprotein A1) - The recycling trucks have a different license plate called ApoA1. If more of these license plates are in action means more cleanup is done.
—————
What to Target?
▶️ Total Cholesterol:
This number is important, but the break up is more important (usually high means more LDL, VLDL… hence a problem)
- Total Cholesterol of around 200 with the right breakup is ideal 🟢
- Too Low & Too High is not ideal 🔴
▶️ HDL-C:
More cleaned up bricks is always better
- For men > 40 mg/dL 🟢
- For women > 50 mg/dL 🟢
▶️ Triglyceride:
Lot of portable Fuel being transported means excess energy/calories in the system.
- Ideal: < 100 mg/dL 🟢
- High Risk: > 150 mg/dL 🔴
▶️ VLDL:
More of portable fuel trucks is indirectly saying more portable fuel is produced.
Hence It is not directly measured, but estimated as 20% of triglycerides
- VLDL < 20 mg/dL 🟢
▶️ LDL-C
More unused bricks in circulation is a concern as more delivery trucks can cause a traffic jam (plaque)
- Ideal: < 130 mg/dL 🟢
- High Risk: > 160 mg/dL 🔴
▶️ Lp(a):
The more unused bricks in circulation especially inside those trucks with sticky tired is a big cause of concern. But it’s not under your control.
- Optimal: < 20 🟢
- SubOptimal: 20- 50🟡
- High risk: 50- 100🟠
- Very high risk > 100🔴
▶️ ApoB:
You want less of trucks with these license plate on the road. They are either carrying unused bricks or extra portable fuel, either way not good.
- Optimal: < 80 mg/dL (high risk patients)
: < 90 mg/dL (general population) 🟢
- High: > 120 mg/dL 🔴
▶️ ApoA1:
You want more of cleanup trucks with these license plate on the road.
- Optimal: < 0.6 🟢
- Acceptable: < 0.8 🟡
- High risk: > 0.9 (men), > 0.8 (women) 🔴
▶️ ApoB / ApoA1 Ratio:
This ratio reflects the balance between Delivery trucks & Clean up trucks. More clean up trucks is always better
- Optimal: < 0.6 🟢
- Acceptable: < 0.8 🟡
- High risk: > 0.9 (men), > 0.8 (women) 🔴
▶️ Triglycerides / HDL Ratio:
This ratio reflects the balance between large Cargo trucks specifically & Clean up trucks. Again more clean up trucks & less portable fuel on the road is always better
- Excellent: < 1 🟢
- Good: < 2 🟡
- At risk: > 2 🟠
- High risk: > 4 🔴
Muscle loss is the #1 side effect of GLP-1s. I wrote the "GLP-1 Muscle Manual" to help you stay strong while losing weight.
It’s FREE for the next 48 hours! 🚨
Check the first reply below for the link. 👇
#GLP1#FreeEbooks#WeightLoss#Fitness
I know there is a lot of disagreement on the role that cholesterol lowering plays in heart disease but can we finally acknowledge that’s statins are the worst option for lowering your cholesterol if that is your goal
@LDLSkeptic@DrAseemMalhotra@nicknorwitz
🧵 Thread on my statin research 👇🏼
Our analysis in @JAMAInternalMed
21 statin trials, 143,532 participants
The benefits of #statins were minimal & most trial participants who took statins, derived no clinical benefit.
Reducing LDL-C with statins showed an inconsistent/weak relationship with MI, stroke & death
https://t.co/oAi5IxbFyx
Taking statins for 5 years extends your life by 3.4 days.
Read that again.
Five years of daily medication. Five years of side effects. Five years of pharmaceutical dependence.
For 3.4 days.
That's the actual data from the NNT (Number Needed to Treat) calculations.
You need to treat 100 people with statins for 5 years to prevent one cardiovascular event. 99 people get no benefit. 20 experience serious side effects.
But they'll put you on them at 35 "just to be safe."
The pharmaceutical industry looked at those numbers and decided they were good enough to medicate half the adult population.
So, one of my brothers had Parkinson's disease. He had it for 20 years. At the 15 year mark, his PD symptoms were barely noticeable. He was doing several holistic remedies, and they were working. Then his doctor said his cholesterol was a little high. He was prescribed a statin. Fast forward 5 years later, he was falling and saying his knees would just give out. After a fall, and being on the floor for 6 hours unable to get up, we found him and took him to the ER. The doctor there looked at his prescriptions I brought with us, and he saw the Simvistatin. He yelled, "WHO IN THE HELL PRESCRIBED STATINS TO A PARKINSON'S PATIENT?!" He told us that the years on statins did irreversible damage and muscle loss. My brother did not have high BP or any heart issues whatsoever. I will NEVER take a statin, EVER!
Statins INCREASE diabetes risk by 46% & could SHORTEN your life...while Big Pharma rakes in trillions!
Dr. Jeffrey Barke, MD exposes the harmful truth about cholesterol lowering drugs like Crestor.
Key facts:
- Every 30mg drop in cholesterol = 22% HIGHER all-cause mortality! ⚠️
- LDL below 70mg/dL = 3X stroke risk!
- Statins add just 3.2 DAYS to life? Big Pharma is scamming us.
Diving deeper: Statins cause NEW-ONSET Type 2 Diabetes! 📈
From the 2015 METSIM study: 46% increased risk after 6 years.
And lowering cholesterol? The Minnesota Coronary Experiment (1968-73) showed it's DEADLY—22% higher death risk per 30mg drop.
Why risk it? Cholesterol protects your brain & hormones!
Common Statins to AVOID: 🚫
- Crestor (Rosuvastatin)
- Lipitor (Atorvastatin)
- Zocor (Simvastatin)
- Lescol (Fluvastatin)
- Mevacor/Altoprev (Lovastatin)
- Livalo (Pitavastatin)
- Pravachol (Pravastatin)
Non-statins with similar risks:
- Repatha
- Zetia
- Nexletol
SERIOUS side effects list:
- Muscle pain/tearing (Rhabdomyolysis)
- Autoimmune diseases
- Dementia/Alzheimer's
- Cancer
- Type 2 Diabetes
- Depression
- Parkinson's
- Stroke
- Neuropathy
- Heart failure
Saturated fats & cholesterol DON'T cause heart issues—it's a myth! Focus on low triglycerides & high HDL via diet & exercise.
Real heart health: Cut sugar/seed oils, eat animal sourced foods! The goal is low insulin, glucose control which equals inflammation control.
Saturated fat has ZERO effect on CVD. Keep triglycerides/HDL for heart health ratio under 1.5 by eliminating sugar, seed oils & processed foods.
Have you ditched statins? What's your story?
Statins are not the hero they are sold as.
They deplete CoQ10 which is critical for heart and mitochondrial function, increase insulin resistance, and have not reduced cardiovascular deaths even in high risk groups.
In the real world, 20 to 50 percent quit within 2 to 3 years due to brain fog, fatigue, and muscle pain.
LDL alone is not the problem. High triglycerides are the real red flag. Start there. Cut high glycemic carbs. Eat whole foods. Raise HDL with DHA EPA or black seed oil.
Before statins, red yeast rice shows better outcomes in trials with fewer side effects.
What doctors think statins do:
- Lower dangerous cholesterol
- Prevent heart attacks
- Reduce mortality
- Safe for long-term use
- Worth the minor side effects
- Necessary for anyone over 190 LDL
What statins actually do:
- Block the mevalonate pathway upstream of cholesterol
- Also block CoQ10 (heart energy), Vitamin K2 (bone/arterial health), dolichols (cell signaling)
- Extend life expectancy by 3-4 days over 5 years
- Cause muscle pain, liver damage, cognitive decline in 20% of users
- Treat a symptom while ignoring inflammation and insulin resistance
- Create lifetime pharmaceutical dependency
You're not getting a cholesterol drug.
You're getting a metabolic wrecking ball that happens to lower one number on a panel.