Mom, geriatrician, senior medical info officer. Passionate about improving lives of older adults & the use of data science & technology in health. Views my own
Great collaboration with @CarlyWelch_42 and colleagues. Deconditioning is a whole body syndrome affecting cognitive as well as physical function, which needs an interdisciplinary working in both clinical practice and research to reduce adverse outcomes https://t.co/O3R4Gy4iBy
😨 Consequences of #delirium
🏥 Most delirium is present on admission; 1/3 of incident delirium can be prevented. Much of the delirium workload is about treatment.
⭐ Need to do more to limit severity & duration
Recent general review: https://t.co/5hBhqsNb8D
I had NotebookLM create a high-level overview of my 237-page thesis in a 15m conversational podcast https://t.co/n0ODGLWwkq ? the future of knowledge translation. Full text here because we can't forget about that just yet! https://t.co/B3TaM65lNA
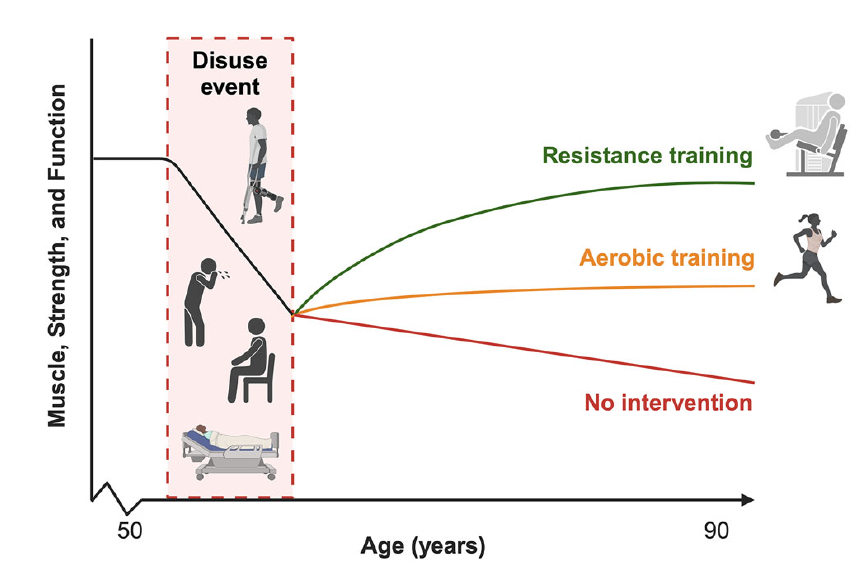
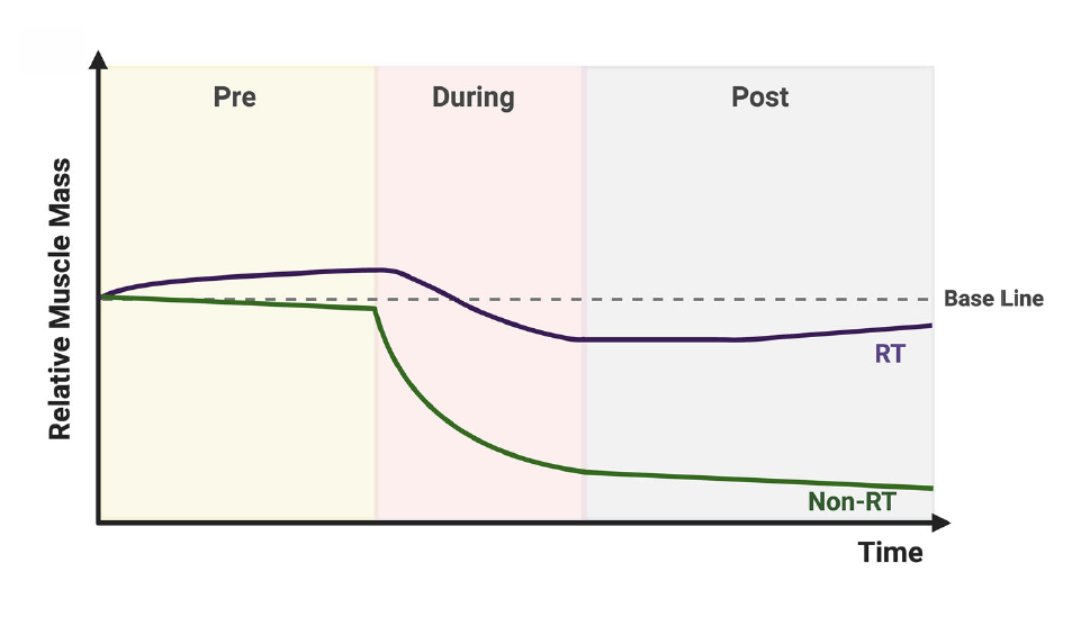
Short periods of inactivity can be disastrous for muscle health, particularly in older adults.
These “disuse events” happen with illness, injury, or hospitalisation.
But what we do around these events can minimise the harmful effects on muscle and physical function:
- Maximising reserves before disuse
- Slowing losses during disuse
- Restoring losses after disuse
Resistance training is a cornerstone strategy across each stage to protect against muscle loss with inactivity.
https://t.co/6yFL5t5JVR
@WHO ..’Rehabilitation continues being wrongly perceived as a non-essential health service for all patients when for many patients it is essential’
#RightToRehab#CovidRehab
“We see people deteriorating in hospital whilst they’re awaiting community beds, and then further deteriorating when they move to community beds without #rehabilitation. This is inhumane.” BGS President @adamgordon1978 via @HSJnews today #RighttoRehab@thecsp
#Delirium is a very common condition in older people admitted to hospital with an overall prevalence of 23%. It is therefore vital that health professionals working with older people have a good understanding of delirium. https://t.co/iqKet7HPPw
Current projections estimate 153 million people will be living with dementia by 2050.
Nearly half of dementia cases could be prevented or delayed by tackling 14 risk factors starting in childhood, suggests new report from a standing Lancet Commission: https://t.co/ZFRBBbIfdZ
Much of dementia—perhaps half—could be prevented or substantially delayed with attention to 14 modifiable risk factors
@TheLancet Commission 2024 report https://t.co/wsphtAfk77
New inclusion of cholesterol and vision loss as risk factors
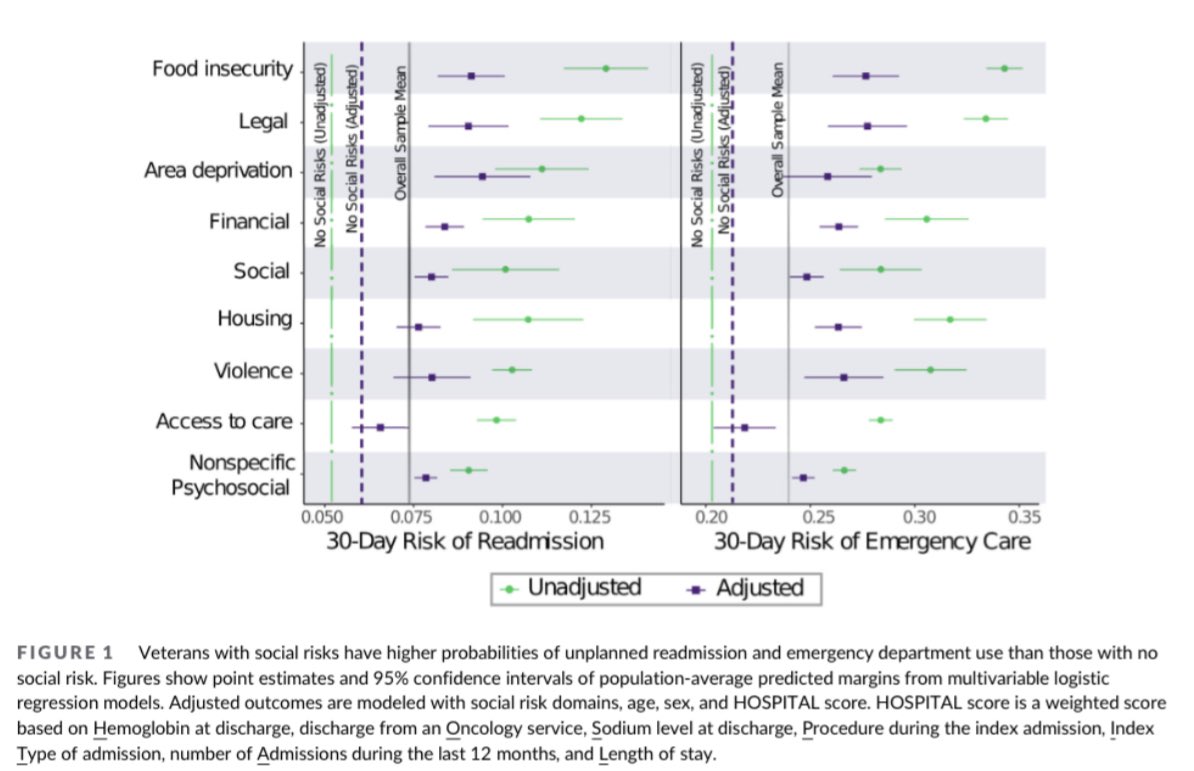
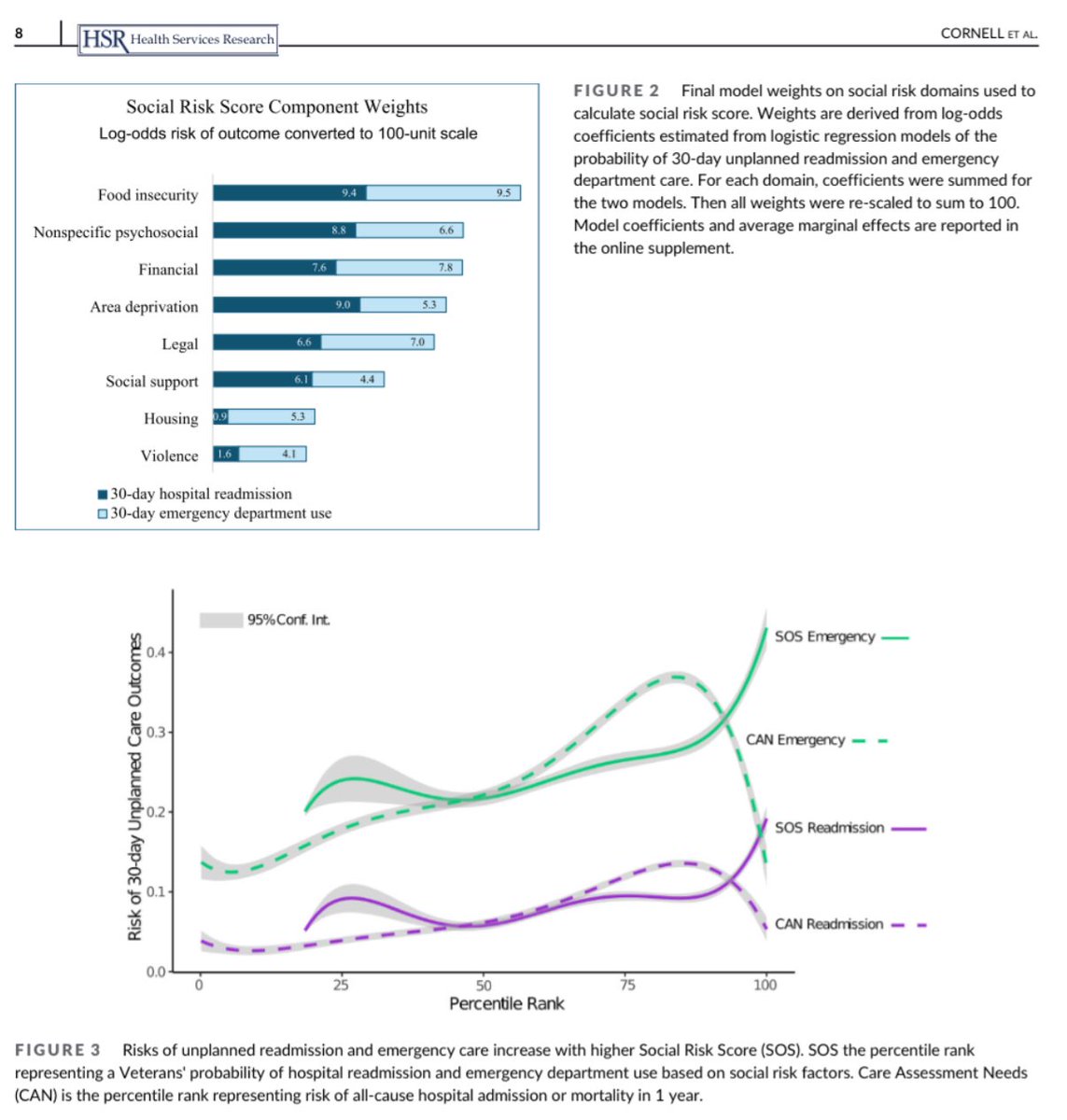
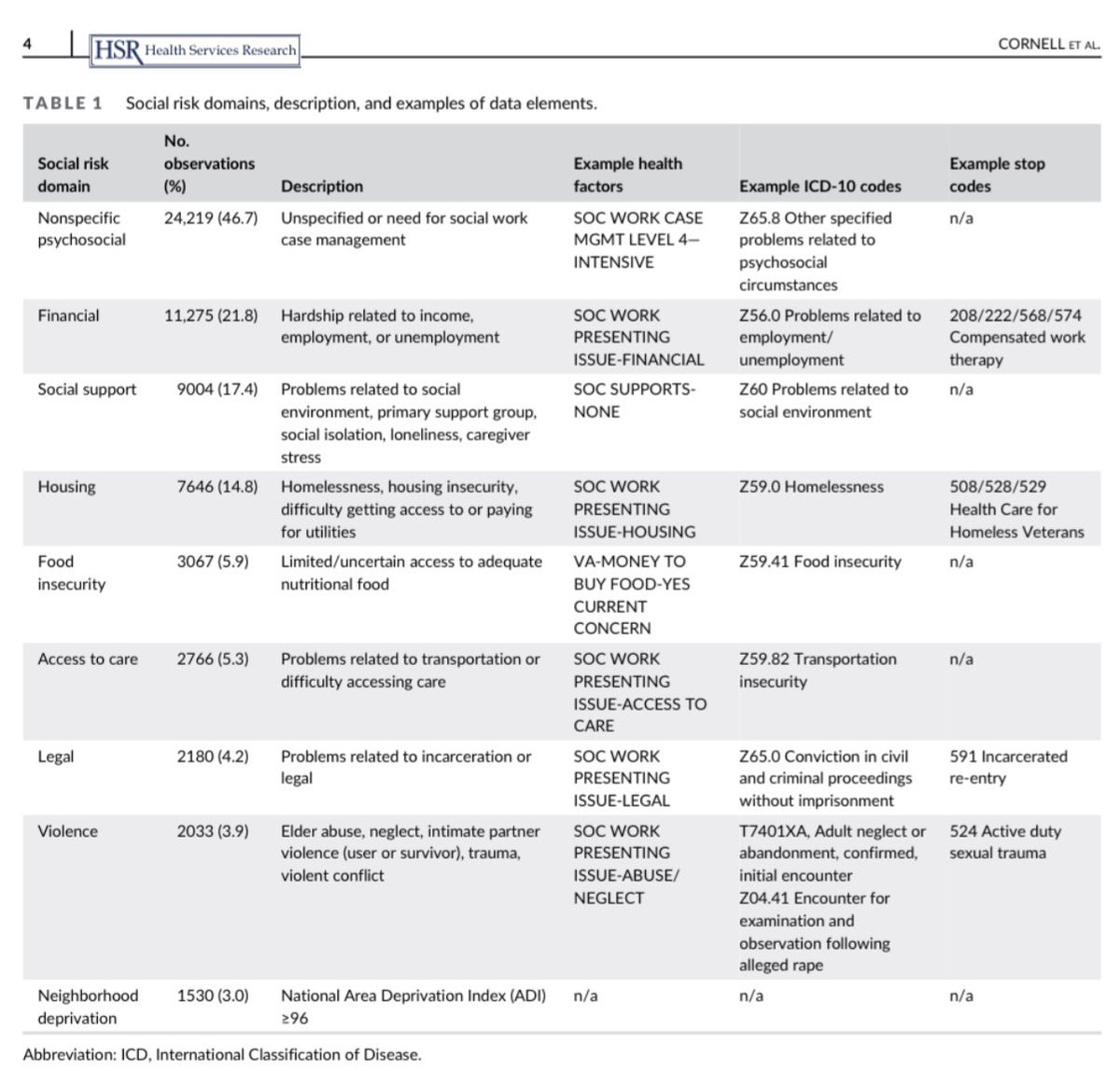
Using social risks to predict unplanned hospital readmission and emergency care among hospitalized Veterans.
https://t.co/8O9WZal9Up
@HSR_HRET #hsr#HealthServicesResearch#SDOH#SocialNeeds
New #EndPJparalysis film!🎦💙
Deconditioning can affect people of all ages and in this clever short film from https://t.co/iaoPrW5qVl and Exec Producer @LyndamHolt, we see that movement matters for all... every single step
HT @agilecsp@GeriSoc@nhsswft
https://t.co/Al2Z4TrkgC
e.g. the temptation to simply buy more care homes beds ignores the fact that a majority of people waiting for discharge don’t need residential care. And ignores the fact that increasingly people want to (& could) live well at home for longer with support
https://t.co/CicwrzBhUH
Are you someone with personal and/or professional experience with aging in place in Canada? 🏠
Canada’s Drug Agency would like to hear from you.
🔗 Learn more: https://t.co/tyZ72mGzpl
Ageing muscle + inactivity = not a good mix.
Just 6-10 days of inactivity during hospitalisation can reduce leg lean mass by >10%.
Here, multicomponent exercise (2 x 20 min sessions) improved measures of physical and cognitive function in older adults (mean age 87) when performed for 3, 4, or 5-7 days in hospital.
For most outcomes, improvements were greater with higher doses (frequencies) of exercise.
https://t.co/SHoYMCKISP
4. Everyone with delirium gets a basic PINCH ME. People get it like they get sepsis. it’s more common…
5. People take the time to find out WM2M.
These aren’t geriatric medicine things, they’re older person things. And that means they’re most of the hospital things
Dreams.
1. Every older person inpatient has a CFS+4AT and people understand why we do them.
2. Everybody caring for older people with frailty can describe how they normally walk vs how they currently walk
3. Clinicians can explain the gap and understand the need for rehab
1. Older people are the main users of acute hospital care. We have a duty to modernise our healthcare systems to offer more care at home, right size our bed bases (with commensurate MDT staffing) identify and protect those most at risk of hospital acquired harm's
Interesting letter in JAMA.
Even short periods of boarding in the ED can precipitate delirium in pts with dementia.
Effects detectable at 4hrs. Non-linear interactions with wait time and age.
https://t.co/JO1CT6oDTG
@RCEMpresident @adamgordon1978