In EVT treated M2 occlusion stroke, larger Tmax >4 s perfusion deficit was associated with worse 90-day functional outcomes.
Tmax >4 s volume >113 mL best discriminated outcomes.
MAD-MT study by @vsyedavalli@NANConsortium
https://t.co/QCLfSvIu6F
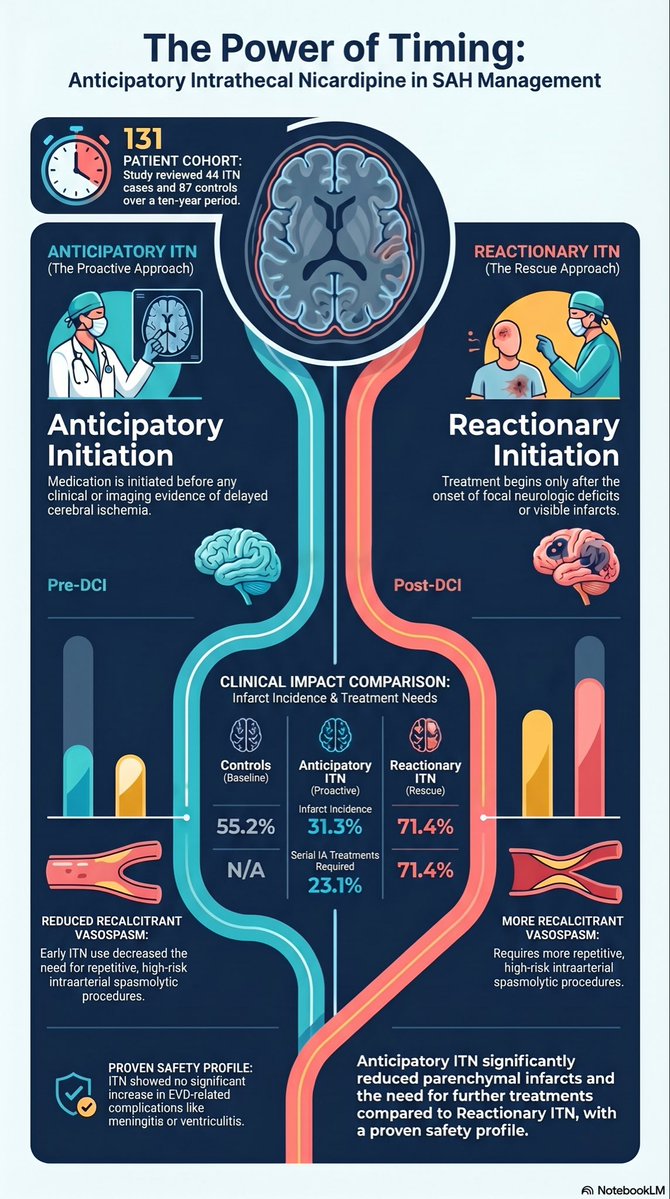
🚨 New study in Clinical Neurology and Neurosurgery on aneurysmal subarachnoid hemorrhage (aSAH) management 🩸 🧠
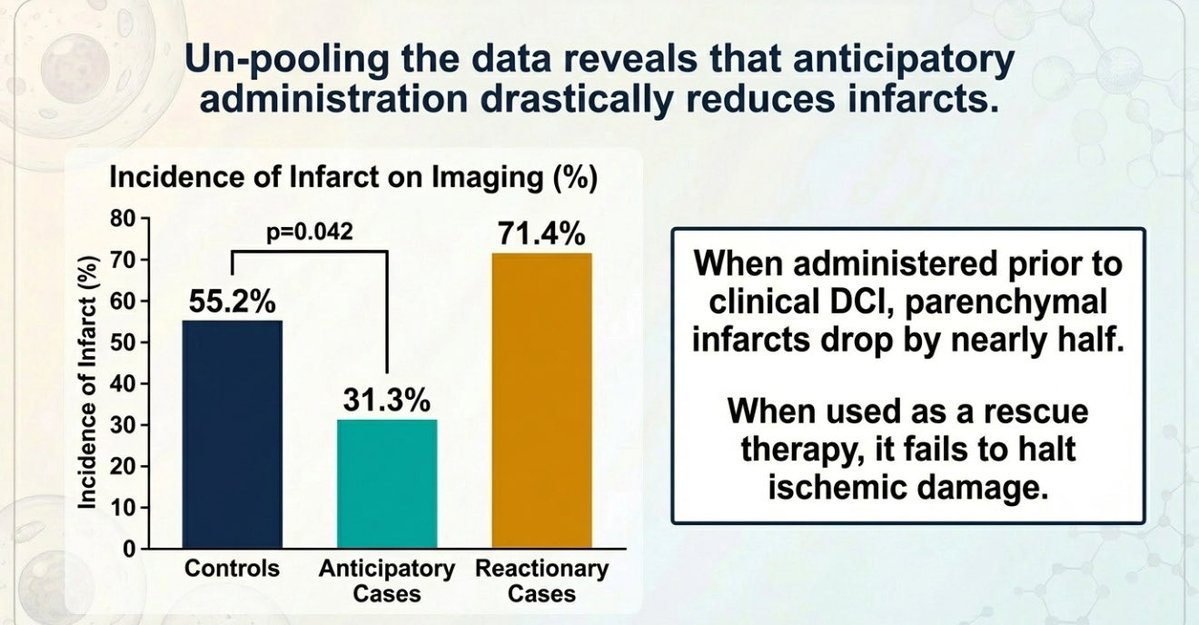
Anticipatory initiation of Intrathecal Nicardipine (ITN)—given before clinical or imaging evidence of delayed cerebral ischemia (DCI)—significantly reduces DCI parenchymal infarcts compared to controls (31.3% vs 55.2%).
Key findings:
📉 Starting ITN prior to intra-arterial (IA) spasmolytics significantly lowers the need for serial IA treatments for recalcitrant vasospasm from 71.4% down to 23.1%.
🛡️ It is a safe intervention with no increased risk of EVD-related complications or meningitis.
⚠️ Timing is everything, because reactionary ITN given after DCI onset did not reduce the rate of additional infarcts or the need for serial IA treatments.
Question: Does this article change your practice?
#NeuroTwitter #NeuroCriticalCare #SubarachnoidHemorrhage #Vasospasm #NeuroSurgery
https://t.co/t09vQGuY3W
"Application of High-Resolution Conebeam CT for Evaluation of Endothelialization after Flow Diverter Implantation for Unruptured Intracranial Aneurysms"
https://t.co/22Uw2yBnM6
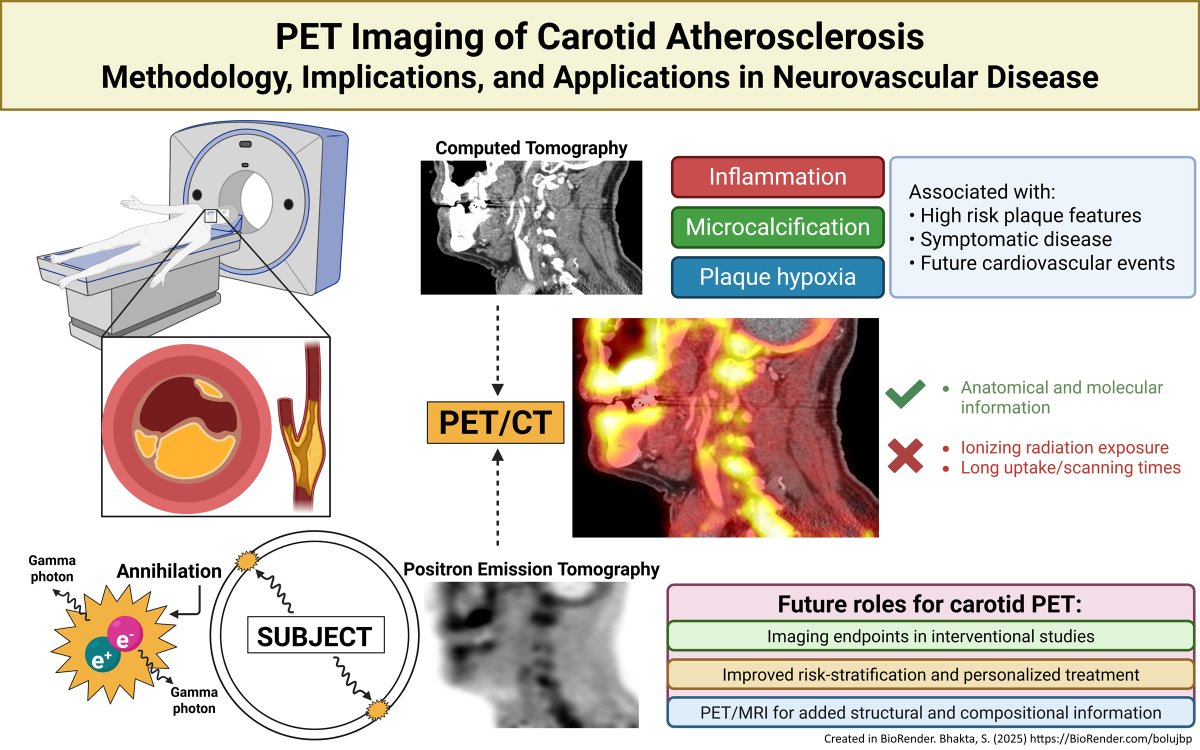
Article Commentary: “PET Imaging of Carotid Atherosclerosis: Methodology, Implications, and Applications in Neurovascular Disease”
In this #BloggingStroke post, Natalie Neale discusses #Stroke article by Bhakta et al. https://t.co/K88JjKpHyn
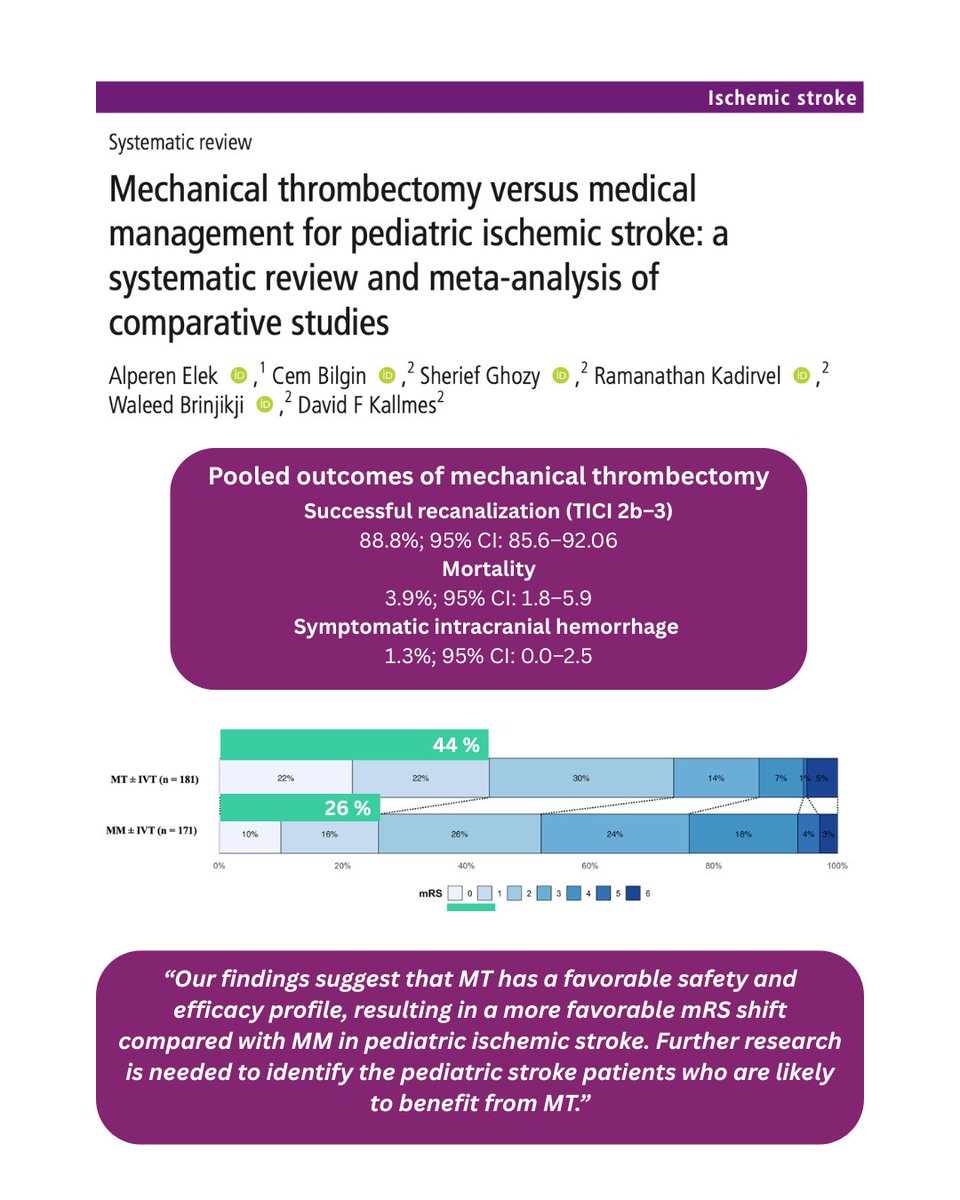
📊 Meta-analysis of 612 pediatric stroke cases suggests mechanical thrombectomy is safe and effective, achieving high recanalization rates and better functional outcomes than medical management—highlighting its promise despite current off-label use. Read more here: https://t.co/Ga9mA9rwDV
@ElekAlperen
🔎🧠In 298 aneurysms, jailing vs re-crossing in stent-assisted coiling showed similar procedure metrics, no significant difference in safety events at 12 months, and comparable occlusion rates (89.4% vs 83.9%). Read more: https://t.co/rtDNmJt5eT
@AshuPJadhav@BrianJankowitz@_AdnanSiddiqui
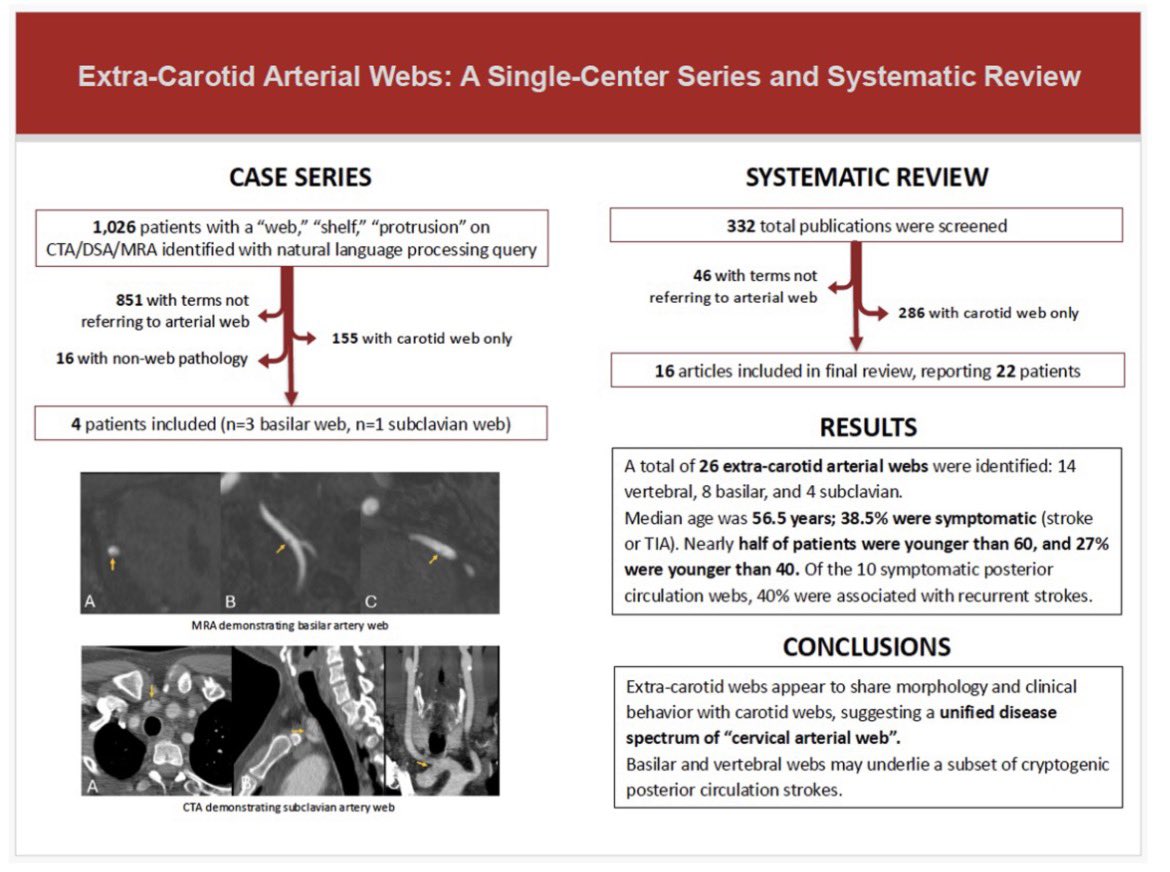
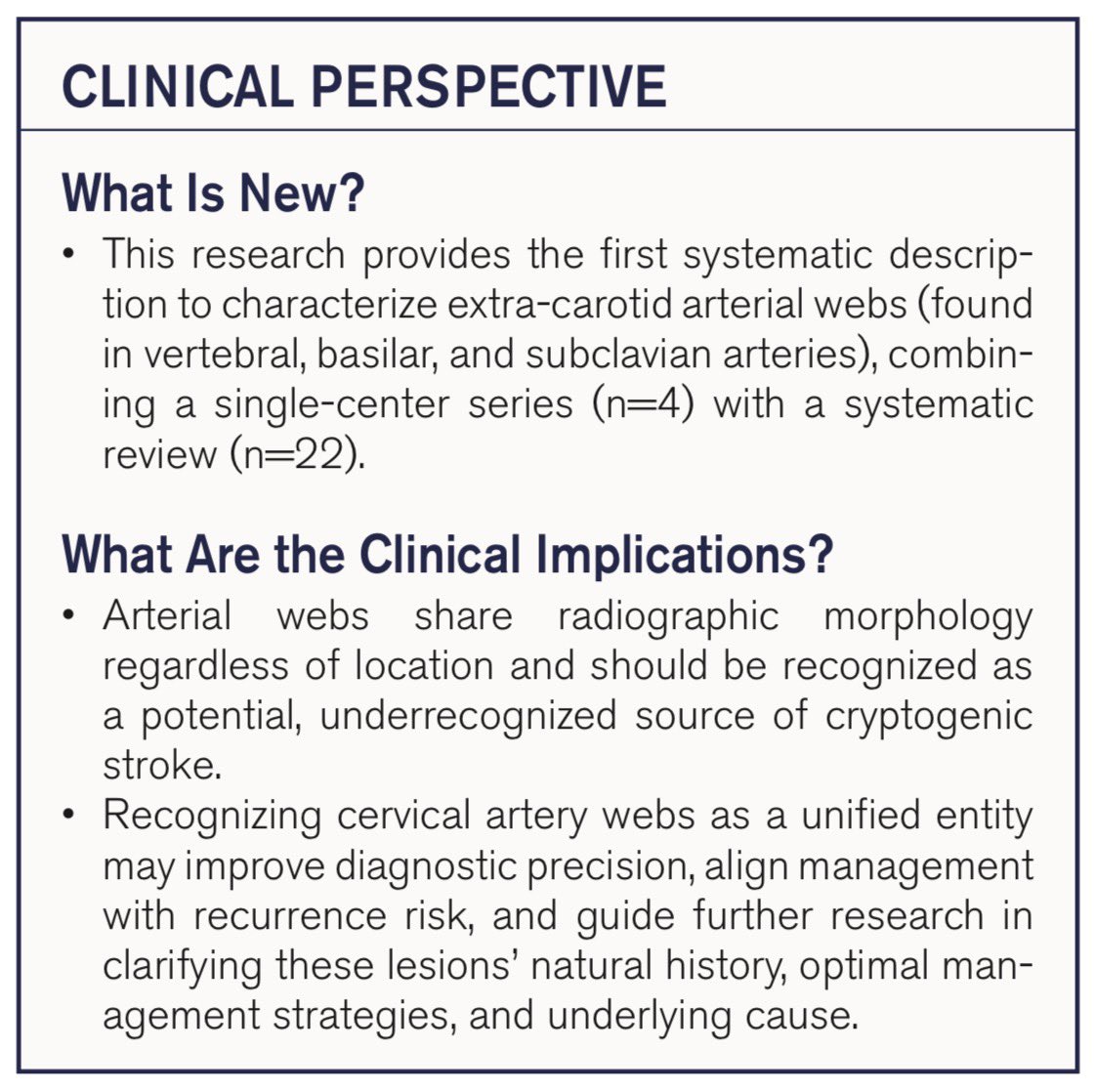
Are arterial webs limited to the carotid?
In our case series + systematic review, we describe extra-carotid webs and propose the term “cervical arterial web”—a unified entity that may represent an underrecognized cause of cryptogenic stroke. @ENossek@BellevueHosp@nyugrossman@nyulangone@svinsociety@SVINJournal@AHAScience
https://t.co/H3P5Czy6op
Left Atrial Appendage Closure or Medical Therapy in Atrial Fibrillation @nejm
“Among patients with atrial fibrillation at high risk for stroke and bleeding, left atrial appendage closure was not noninferior to medical care mgmt with regard to a composite end point of stroke, systemic embolism, major bleeding, or cardiovascular or unexplained death.”
Translation: patients randomized to LAA closure did worse then those treated with anticoagulation
https://t.co/wEC3tp2KgY
🧠 Dyslipidemia Management in Stroke Prevention
✍ Current evidence and a phenotype-guided, individualized framework for dyslipidemia management across stroke subtypes
Read the review here! 👇
https://t.co/ZOyzCKrVQm
Crossed cerebellar diaschisis (CCD) explains this phenomenon, where a unilateral supratentorial cortical lesion causes contralateral cerebellar hypometabolism or hypoperfusion.
It is a functional disconnection of the cerebrum-ponto-cerebellar pathway, typically seen following acute stroke or seizure.
This image compares cerebral blood flow patterns associated with Crossed Cerebellar Diaschisis (CCD).
https://t.co/TLbEY6YPHe
🧠🔬 Neuro-dedicated intravascular OCT is emerging as a promising tool for intracranial vascular imaging. By enabling microscopic, high-resolution visualization of vessel wall pathology and therapeutic devices, it may expand our understanding of cerebrovascular disease and improve neurointerventional diagnosis and treatment strategies. 📖 Read more (open access): https://t.co/uGur9YugEj
@Cure4Stroke@_AdnanSiddiqui@Fie0815@vitorpereiraca
🧠💉 In TNK-treated LVO stroke patients eligible for EVT, thrombus migration occurred in 36% and made EVT impossible in 26% vs 4% without migration. Thrombus migration significantly reduced rates of complete reperfusion but did not affect functional outcomes. Read more here: https://t.co/vv9lXmlFx3
@jildazz
The economics of VSS Versus VPS for IIH :
(propensity-weighted, cost lens) our superstar research fellow @VictorGabriel_H has some numbers for you in this recent paper in @JNIS_BMJ@SNISinfo :
💰 Initial costs = twins
😵💫 Complications = 3.5% vs 37.7%
🏥 30d readmissions = 1.3% vs 33%
🚑 30d ER visits = 11.1% vs 36.6%
🔧 Reops = 1.3% vs 30.9%
All the extra 💰 goes on complications, readmissions and reoperations in the VPS arm! @TJUHospital@TJUHNeurosurg
https://t.co/B3a2E5qvAu
#STROKE: First-in-human study to enable live visualization of intracranial, including stents, flow diverters & thrombectomy, without complications. https://t.co/Ts4XGDjmM3
#MondayTip
Hypoperfusion Intensity Ratio
#HIR may be the most practical collateral biomarker in AIS
⬆️High HIR (>0.4) → rapid core growth, ↑ hemorrhage risk, worse mRS.
⬇️Low HIR → robust collaterals & better EVT outcomes.
https://t.co/wRfh2VnWQ8