Waarom deed je het dan, Károly?
En waarom censureerde je met de Denktank Desinformatie iedereen de moeder die onze kinderen probeerde te beschermen tegen deze waanzin?
"SIDS ‘DISAPPEARED’ In Japan After Raising The Age of Vaccination To 2yrs Old."
~Dr. Pierre Kory, MD
In 1981, Japan delayed the DTaP vaccine until children turned two years old.
Japan holds one of the lowest infant mortality rates, while the US ranks among the highest.
During the 1970s, following only two reported infant deaths linked to the whole-cell pertussis vaccine (DTwP), intense public concern prompted the Japanese government to halt routine DTwP vaccinations.
They later introduced the acellular pertussis version (DTaP) in 1981, but limited its use to children aged two and older.
In 1993, Japan’s Ministry of Health, Labor & Welfare discontinued the combined MMR vaccine after it triggered a significant increase in severe adverse reactions — particularly aseptic meningitis resulting in serious harm and fatalities.
Japan now provides separate measles and rubella vaccines and has never reintroduced the mumps component or the MMR combination shot.
In 1994, Japan revised its Immunization Act, changing all childhood vaccinations from mandatory to voluntary/recommended status.
This removed any penalties for declining vaccines and moved administration from mass public health clinics to individual choice via private doctors — prioritizing personal decision-making and informed consent.
The U.S. continues to have the highest infant mortality rate among 16 other developed nations.
As of 2022, the CDC reports the U.S. rate at 5.6 deaths per 1,000 live births. Japan’s rate remains among the world’s lowest at 1.7 per 1,000 — the U.S. rate is more than three times higher.
I'm a cardiologist. I prescribe cholesterol-lowering drugs every single day. They save lives. That science is settled and I will never tell you otherwise.
But I'm going to say something that will make a lot of my colleagues uncomfortable — because someone needs to say it, and your doctor probably won't.
Too many physicians make you feel crazy when you bring up statin side effects.
You walk into your appointment and say "my muscles ache constantly" — and you're told it's in your head. You say "I'm exhausted all the time" — and you're told it's your age. You say "my sex drive disappeared" — and you get an awkward silence followed by a subject change. You say "I don't feel like myself anymore" — and you're told the benefits outweigh the risks, take the pill, stop reading the internet.
I've watched it happen in my own field for twenty years. The conversation gets shut down. The patient gets dismissed. And then they do the one thing we should be most afraid of — they stop the medication entirely, without telling us, and lose the cardiovascular protection that's keeping them alive.
That is the real cost of not being honest. Not the side effects themselves — the silence that drives patients away from treatment.
In my practice, I see statin-related complications in at least 25% of my patients. Muscle pain. Fatigue that doesn't resolve with sleep. Reduced sexual drive. Brain fog. Cramping. Joint stiffness. Weakness that makes exercise — the very thing we tell them to do — feel impossible.
Some of these improve with CoQ10 supplementation and optimizing vitamin D. Many do not.
I wrote about the diabetes risk of statins in a New York Times op-ed in 2012. The backlash from the cardiology establishment was immediate. I was told I was undermining trust in a life-saving drug class. Fourteen years later, every major guideline acknowledges the risk I warned about. It's in the prescribing information. The physicians who attacked me for saying it now teach it to their residents.
The truth doesn't care about professional comfort. It never has.
Now a paper published this week in Science Advances has finally explained the mechanism behind statin myopathy — and the finding validates what millions of patients have been telling their doctors for years.
Researchers discovered that statins activate the NLRP3 inflammasome in muscle cells — triggering an inflammatory cascade that causes muscle cell death, activates atrophy pathways, and disrupts muscle metabolism. This is entirely independent of the drug's cholesterol-lowering effect.
The muscle damage isn't caused by lowering cholesterol. It's caused by a completely separate pharmacological action through a different pathway.
The critical implication: the side effect can potentially be separated from the benefit.
Blocking NLRP3 or restoring isoprenoids prevented muscle cell death without interfering with cholesterol reduction. Future therapies could preserve the cardiovascular protection while eliminating the muscle toxicity.
Even more striking — the researchers found that background systemic inflammation significantly lowered the statin dose needed to trigger muscle damage. Patients with chronic inflammation, gut dysbiosis, or metabolic syndrome may be experiencing myopathy at doses their doctors consider "too low to cause problems." They're not imagining it. Their inflammatory state is priming the pathway.
The muscle pain was never in their heads. It was in their NLRP3 inflammasome. And we finally have the molecular proof.
Here's what I actually do in my practice — because I refuse to choose between protecting the heart and respecting the patient.
Whenever possible, I avoid statins as my first-line approach for eligible patients by using alternatives that lower LDL through entirely different mechanisms with no muscle toxicity:
PCSK9 inhibitors — Repatha and Praluent. Injections every 2-4 weeks that dramatically lower LDL without touching muscle tissue. No myopathy. No fatigue. No brain fog. For patients who can access them, these are transformative.
Inclisiran — Leqvio. An siRNA injection I administer twice a year in my office. It silences the PCSK9 gene in the liver. Two shots a year. LDL drops roughly 50%. No muscle side effects. No daily pills. Now approved as first-line monotherapy. This is the future of lipid management and I use it aggressively.
When statins ARE clinically necessary — and sometimes they are, especially post-heart attack or in combination therapy — I choose hydrophilic statins like rosuvastatin or pravastatin. These do not easily cross the blood-brain barrier. The cognitive complaints — the fog, the memory issues, the feeling of "not being yourself" — are substantially less common with these formulations because the drug stays out of the central nervous system.
I never prescribe a statin without CoQ10. 100-300mg daily. Statins deplete the cellular energy molecule your muscles and heart depend on. Replenishing it reduces muscle symptoms in many patients. It should be standard practice. The fact that it isn't is a failure of our field.
I check vitamin D and optimize it aggressively. Low vitamin D — which is epidemic — worsens muscle symptoms independently and compounds whatever the statin is doing. Target 50-80 ng/mL, not the bare minimum of 30.
Bempedoic acid — Nexletol — for patients who can't tolerate any statin. Works upstream in the cholesterol pathway and is not active in muscle tissue. Specifically designed to avoid myopathy.
Ezetimibe added to a lower statin dose. Cut the statin intensity, add ezetimibe to maintain the LDL reduction, and halve the muscle exposure.
There is no excuse in 2026 for telling a patient "just deal with the muscle pain." The toolbox is deep. The alternatives exist. The only barrier is a physician's willingness to listen and adapt.
I want to speak directly to every patient who has been dismissed.
Your muscle pain is real. Your fatigue is real. Your cognitive changes are real. Your loss of drive — in every sense of the word — is real. A paper in Science Advances just proved the mechanism. You were never crazy. You were experiencing a documented inflammatory response in your muscle tissue that your doctor didn't have the science to explain — until this week.
And I want to speak directly to my colleagues.
We have to be honest. Not just about the benefits — which are enormous and undeniable — but about the side effects, the mechanism, and the alternatives. Patients who feel heard stay on treatment. Patients who feel dismissed stop their medications in silence — and die from the heart attacks we could have prevented if we'd simply been willing to have an honest conversation and switch the approach.
The cardiologist who tells you statins are flawless is not protecting you. The wellness influencer who tells you statins are poison is not protecting you either. The truth lives in the middle — where it always has.
Statins save lives. The side effects are real. The mechanism is now proven. The alternatives exist. And you deserve a doctor who holds all four of those truths at the same time.
Both things can be true. They always could.
Now we have the science to prove it.
Enquête Telegraaf: Nederlanders vernietigend over asielbeleid kabinet-Jetten:
— Slechts 3% (!) vindt dat kabinet-Jetten de asielopvang goed aanpakt.
— Zes van de 10 beoordelen het beleid als (zeer) slecht.
— 73% spreekt van een asielcrisis.
https://t.co/sF8d94R7iT
Bericht van november 2021 nadat er massaal gevaccineerd werd tegen corona.
Wetenschappers begrepen niet vanwaar de grote oversterfte kwam.
“Oversterfte vier keer zo groot als officiële aantal coronadoden: hoe kan dat?”
https://t.co/PbF6CJdEtH
Leaked video of Mark Zuckerberg where he warned his Facebook execs NOT TO GET VACCINATED with the mRNA (COVID) vaccines because "we don't know the long-term side effects of modifying people's DNA & RNA"
He censored doctors, scientists, and the sick who denounced the ‘Vaccines"
En misschien nog wel het allerergste en het allergrappigste is dat onze frikandellendealer @hugodejonge er niet bij vertelde dat er op dat moment precies nul bewijs voorhanden was dat zijn frikandellen een effect hadden op de sterfte.
Er moest een door Pfizer bedachte, door #Pfizer opgezette, door Pfizer uitgevoerde, door Pfizer geanaliseerde en door Pfizer gepubliceerde oorverdovend rammelende studie aan te passen komen om zijn vieze frikandellen aan de man te mogen brengen.
En daarna moest er natuurlijk heel wat bij elkaar gefantaseerd worden door het @rivm en het #Nivel om ons wijs te maken dat de frikandellen toch echt heel veel levens gered hadden.
Maar ja, die #oversterfte, hè. Die #oversterfte. Dat kan Daan de Kortzichtige dan ook maar beter onaangeroerd laten.
#witwasenquete #doofpotenquete.
🚨THIS IS A MAJOR SCANDAL!
Senator Ron Johnson:
“This is a MAJOR SCANDAL! Hundreds of thousands of people are permanently disabled or lost their life because our FDA ignored the COVID injection harms.”
Hundreds of thousands.
Permanently disabled.
Dead.
Because the FDA ignored the safety signals.
The mainstream media still won’t cover it. They’re protecting the narrative instead of the people.
How many more Americans have to be destroyed before we get real accountability?
De kloof in de berichten die mensen in de Verenigde Staten te horen krijgen en wat mensen in Nederland te horen krijgen wordt groter en groter. Ik vraag me af hoe groot die kloof nog wordt voordat de wal het schip keert. Want van de Nederlandse media hebben we niets te verwachten.
Zojuist, op haar laatste dag als directeur van de Nationale Inlichtingendiensten van de VS, declassificeerde Tulsi Gabbard de doofpotaffaire rond COVID-19. Nooit eerder vertoonde documenten. Fauci's vingerafdrukken op de inlichtingendiensten zelf. Een leugen die onder ede aan het Congres werd verteld.
De publicatie schetst drie rollen die Fauci tegelijkertijd vervulde:
* Hij financierde het gain-of-function-onderzoek in het laboratorium in Wuhan.
* Hij adviseerde de inlichtingengemeenschap in het geheim over de oorsprong van het virus. Begin 2020 was dat.
* Hij verscheen op televisie en noemde het lek uit het laboratorium een complottheorie.
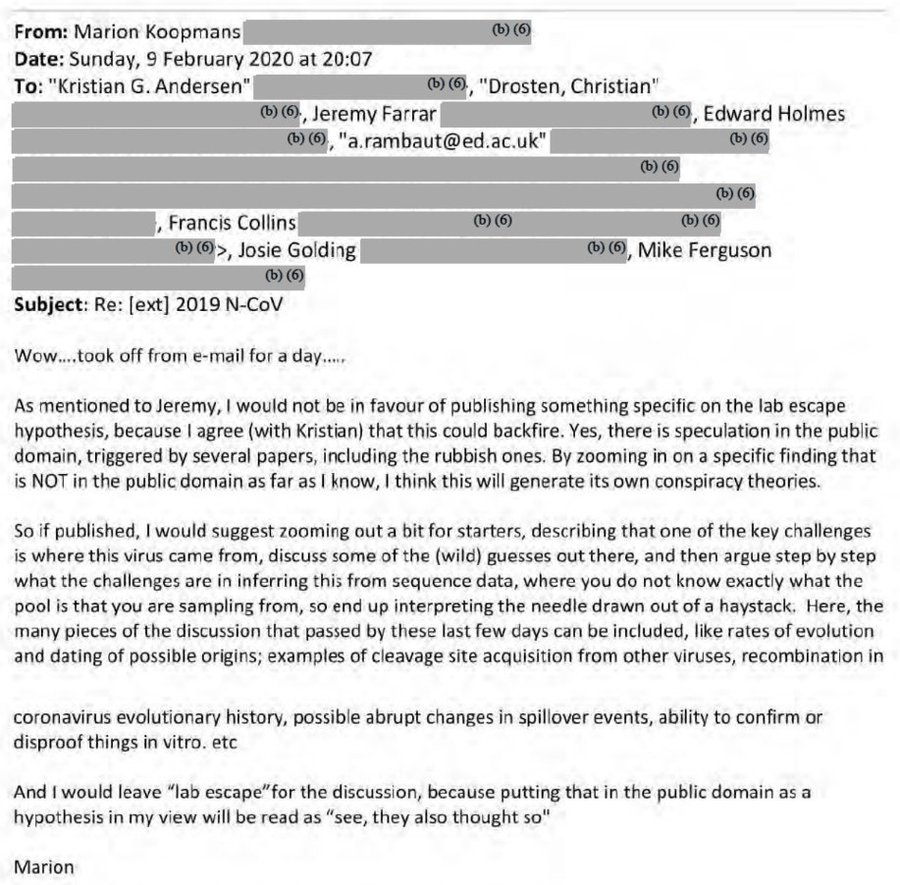
En in Nederland? In Nederland is er niets aan de hand. Als je op had gelet de afgelopen jaren, en verder keek dan wat de main stream media ons wijsmaakten, dan was bekend dat voor Marion Koopmans grosso modo hetzelfde gold als voor Anthony Fauci. Ze was betrokken bij de geheime teleconferentie van 1 februari 2020 en spande zich in om een lablek als complottheorie weg te zetten. Ze had zitting in het OMT en dus invloed op het uitrollen van de Coronamaatregelen en ze had vele andere petten op. Daarbij werd en wordt ze anno 2026 nog steeds als expert opgevoerd in de media. Het is bizar om het te zien.
Dat dit kon gebeuren en dat wordt gedaan alsof dit volstrekt normaal is geeft aan hoe morsdood de media zijn, hoe ze in dienst staan van lobby-groepen en ook de inlichtingendiensten. Ik ben oprecht benieuwd wanneer de waarheid in Nederland bekend wordt. Want de VS zijn geen klein land. In een democratie zouden de waakhonden ervan, de pers en de Tweede Kamer, allang zijn aangeslagen. Maar het bleken schoothondjes en lakeien van de macht.
Bijlage: e-mail die Marion Koopmans stuurde naar andere deelnemers van de geheime tele-conferentie van dr. Fauci en waarin ze ervoor pleit om het lablek onder de pet te houden.
Follow the science werd dat genoemd. Nou, als mij iets duidelijk is geworden is dat mensen met belangen, waar ze niet eerlijk over waren, een mogelijke oorzaak van Corona onder de pet hebben gehouden. Dezelfde virologen die pretenderen dat ze de mensheid beschermen tegen pandemieën. En als zij er nou eens de oorzaak van waren? Ik maak me oprecht zorgen om die kloof van informatievoorziening in Nederland. Een deel van de mensen gelooft de MSM nog en een deel niet. Je kunt niet eeuwig mensen onwetend houden over de ware toedracht, zeker niet in deze tijd van het internet en social media.
A Japanese immunologist spent 20 years proving that the chemicals trees release into the air walk into your bloodstream, hunt down your stress hormones, and arm your immune system in ways no therapist or pharmaceutical has ever matched, and most of the data has been sitting in Japanese medical journals for two decades waiting to be translated.
His name is Qing Li.
He is a clinical professor at Nippon Medical School in Tokyo and the president of the Japanese Society of Forest Medicine. The Japanese government has been funding his research since 2004, and the body of work he has produced is the reason forest bathing is now an officially prescribed clinical therapy in Japan and Korea.
The story actually starts in 1982, when the Japanese Ministry of Agriculture, Forestry and Fisheries coined the term shinrin-yoku to describe the practice of slow, mindful walking in a forest. They did it for a practical reason.
Japan was urbanizing fast, stress-related illness was climbing, and the country had thousands of square kilometers of forest sitting unused. The idea was to give people a reason to walk into the trees... They had no idea what was actually happening to the human body during those walks until Qing Li ran the first proper experiment in 2005.
He took twelve healthy adult men on a three-day, two-night trip to a forest park. They walked for a few hours each day. Nothing strenuous. No prescribed routes or breathing exercises. They simply walked slowly through the trees, breathing the air, looking at the forest.
Li drew blood and urine samples before the trip, on the second day, on the third day, on day seven after returning home, and again on day thirty.
The numbers that came back from the lab were not what anyone expected.
The activity of a specific type of immune cell called the natural killer cell, which is the cell your body uses to hunt down cancer cells and virus-infected cells before they can spread, had jumped by roughly 50 percent during the forest trip. The actual number of natural killer cells circulating in the bloodstream had increased significantly.
Three different anti-cancer proteins that those cells produce, called perforin, granzymes, and granulysin, had all risen sharply. And the effect did not disappear when the men went home. The immune boost was still measurable on day seven and was still partially present on day thirty.
Two hours a day in a forest had upgraded the immune system for a full month.
Li ran the same experiment with women a year later and found nearly identical results. Then he ran it with a control group who took a three-day trip through an urban area with the same amount of walking, the same hotel quality, and the same diet.
The urban group showed no measurable change in natural killer cell activity at all. The forest was doing the work, not the vacation.
The mechanism turned out to be a class of airborne molecules called phytoncides. Trees produce these compounds to defend themselves against insects, bacteria, and fungi. Pine, cedar, oak, and cypress trees release them in particularly large amounts, especially in warmer weather and after rainfall.
When you walk through a forest, you are inhaling those molecules into your lungs and absorbing them through your skin, and once inside your body they appear to directly stimulate the production and activity of the very immune cells Li was measuring in his lab.
Roughly 50 percent of the health benefit of a forest walk, according to Li's data, comes from the chemistry of the air itself. The other half comes from what the forest is doing to your nervous system.
This is where it stops being only about the immune system and starts being about stress.
A separate Japanese research team measured cortisol, the body's main stress hormone, in 84 participants across 35 different forest sites. They drew samples before and after a 30-minute walk in each forest and compared them to control walks in matched urban environments. The cortisol levels of the people who walked in the forest were lower than the cortisol levels of the people who walked in the city by a significant margin. Their heart rates were lower. Their blood pressure was lower.
The activity of their parasympathetic nervous system, which is the part responsible for rest and recovery, had gone up. The activity of their sympathetic nervous system, which is the part that drives fight or flight, had gone down.
Then a researcher at the University of Michigan named MaryCarol Hunter ran the cleanest version of this experiment ever done. She recruited participants from a city and told them to take a nature pill three times a week for eight weeks.
They were free to choose the time, the place, and the duration of the nature experience, as long as it was outside, in daylight, and free of phones, conversations, and aerobic exercise. They sent her saliva samples before and after each session so she could measure cortisol changes accurately and rule out the normal daily drop in stress hormones that happens to everyone.
The result was that participants experienced a 21.3 percent drop in cortisol per hour spent in nature, with the biggest payoff happening between minutes 20 and 30 of the walk.
After that, the cortisol kept dropping, but more slowly. The threshold dose for measurable stress relief was just 20 minutes outside in something that looked and felt like nature.
What none of this means is that nature is a substitute for therapy or for medication when someone genuinely needs them. Therapy treats different things than a walk does, and Li himself has been careful in interviews to call forest bathing a complementary intervention rather than a replacement for clinical care.
But what the research has settled is that the human body has a physiological response to being among trees that operates on the same biological systems modern medicine is trying to reach with drugs and clinical protocols, and that response is fast, measurable, and free.
The strangest part of Li's work is the implication he keeps repeating in interviews. The average person now spends more than 90 percent of their life indoors. Their cortisol stays elevated. Their natural killer cells stay sluggish.
Their parasympathetic nervous system rarely gets a chance to take over. The system that was tuned by millions of years of life under a canopy of trees is being asked to run permanently inside a box made of drywall and screens.
Your body has not forgotten what it is supposed to do in a forest. It is waiting for you to walk into one.
On 22/10/2020 the FDA as part of the Covid vaccine approval process made a 9 hour slide presentation public. One slide was skipped over at Timestamp: 2:33:40 being on screen for a fraction of a second.
Below is that slide.
The FDA deliberately tried to hide the side effects.
Na het ontluisterende verhoor van @hapelensrob komt vandaag de Inspectie Gezondheidszorg en Jeugd tekst en uitleg geven. @mauricedehond en ik bespreken het vanavond om 21 uur met @BumblebeeJoe, die het als neuroloog ook aan de stok had met de autoriteiten.
#CoronaEnquête https://t.co/eBLr3xkr2z
Elens vertelt aan dhr Huidekooper (D66) wat er in een frikandel zit. Hij begrijpt niet waarom Elens het over frikandellen heeft. Nou Dion, omdat de minister destijds die vergelijking maakte en tot op de dag van vandaag niet weet wat er in mRNA vaccins zit en wat de lange termijn effecten zijn, terwijl hij iedere kritische vraag hierover afdeed als desinformatie en artsen als Elens ermee schoffeerde. Dat Elens alle frikandel ingrediënten opsomt doet er dus wel degelijk toe.
Elens, wat een baas. RESPECT! 👌🏼