What happens when low-income Medicare beneficiaries lose subsidized drug coverage (aka the Part D Low Income Subsidy)?
Unfortunately, they are much more likely to die.
And these deaths are likely preventable .
Our new @NEJM study out today
https://t.co/z8cgDgb2lq
Congratulations to all medical students matching today!
Especially excited to welcome the new 2026-2027 Class of @BrighamWomens Internal Medicine Interns!
We are looking forward to working with you all very soon.
@MassGenBrigham@BrighamMedRes
As many as 724,000 service members, their families and veterans may rely on health care at hospitals that face financial vulnerability, partly due to cuts in President Trump's megabill, according to a new analysis. https://t.co/7kJr3245Nw
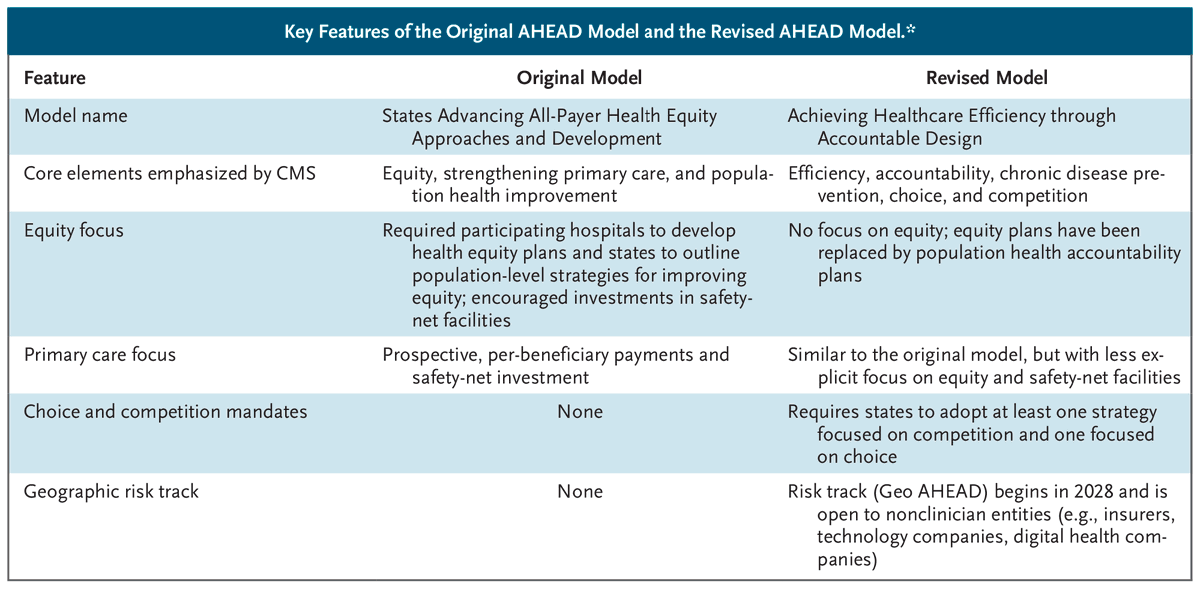
Perspective by Jose F. Figueroa, MD, MPH (@joefigs2), and Ellen Meara, PhD: From Equity to Efficiency — Navigating Changes to the AHEAD Model https://t.co/HWSU1pB9Bq
#HealthPolicy#MedicalEthics
If implemented thoughtfully, LEAD could strengthen care coordination for high-need dual-eligible beneficiaries; If not, it may reproduce familiar patterns in which well-resourced organizations succeed while providers serving the most vulnerable communities face structural disadvantages.| Forefront
William D. J. Roberts, @joefigs2 | @HarvardHSPH
https://t.co/qYAerbhujy
In a new Perspective, Jose F. Figueroa, MD, MPH (@joefigs2), and Ellen Meara, PhD, write that the AHEAD model was intended to slow health care cost growth, improve population health, and advance health equity. But under the new administration, its focus has shifted from equity to efficiency. Learn more: https://t.co/aaItri3gvO
Our new study in @TheLancet leveraged a natural experiment to evaluate the impact of early termination of SNAP emergency allotments between 2021-2022 on all-cause hospitalizations and mortality.
https://t.co/auo3xCd6VI
@SmithBIDMC@BidmcCvi@BIDMChealth@joefigs2@rkwadhera
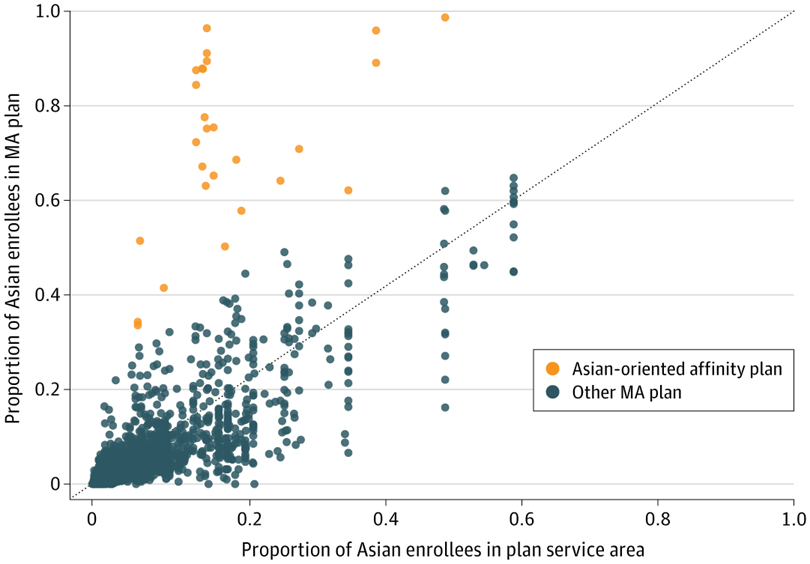
While Medicare Advantage Asian-oriented affinity plans offered more culturally relevant benefits and favorable premiums, these plans had narrower physician networks, lower Medicare Star Ratings, and reduced coverage of certain traditional benefits. https://t.co/7Ia6UZmwcB
Big picture:
Strong performance on prevention *within* the health care system isn’t enough to protect us if prevention *outside* it remains weak.
Work in collaboration w/ Irene Papanicolas @BrownUniversity + Tania Sawaya + @DrBleich@HarvardChanSPH@HarvardHPM
We often hear that the U.S. underinvests in primary care and prevention—and that this explains why Americans live shorter, less healthy lives.
In new @TheLancet Public Health study, we take a closer look at this issue.
https://t.co/hnPLvEdSc5
3. Public health policies lag far behind — the US has much weaker regulation of food, tobacco, alcohol, and firearms.
At same time, we eat more calories, have higher obesity prevalence, and more illicit drug/opioid use. This is why Americans are more likely to die prematurely.
In their new Forefront article, Rebekah Stein, Yanlei Ma, Jessica Phelan, and @joefigs2 from @HarvardHSPH examine ongoing enrollment growth of chronic condition special needs plans (C-SNPs) overall and among the dual-eligible population. https://t.co/wEpo3NmIvw
Some federal funding finally sent to Harvard for about 200 grants totaling $46 million.
Ends a 4-month federal funding freeze — but not all grants restored yet.
https://t.co/kmZXR3Bhpj
Just wow. A new GAO study found that Georgia's work requirements cost $54 million in administrative costs in first four years! More than spent on enrollees' healthcare!
Work requirements are a boondoggle that will worsen bureaucratic bloat in healthcare
https://t.co/pvQMBoXxnC
Viewpoint: #Medicaid is vital for low-income, dual-eligible adults and people with disabilities, but coverage disruptions due to administrative barriers increase health risks. https://t.co/eij4tby4wd
Thank you @RepMarkTakano for the opportunity to share our research (with @joefigs2 and HQO Lab) with @VetAffairsDems
As VA shifts to community care, important to monitor quality of care veterans are receiving.
https://t.co/GTaUvIrHl6
@BrighamSurgery@HarvardHPM
And so the Medicaid cuts begin..
Right before Labor Day weekend the state of Idaho announced 4% cut in Medicaid provider rates for EVERY category except tribal providers effective 9/1
Idaho has lots of provider shortages in rural areas already. This won't help.
As a doctor, I know there isn’t always a treatment for every illness, but the prescription for homelessness is clear. Housing has an outsized benefit in helping patients experiencing homelessness improve their health.
Sign of a broken US health care system when patients with cancer feel like this:
“I always told myself the stress of dealing with insurance was worse than the cancer.”
Insights from patients dealing with prior authorizations in @JAMANetworkOpen study https://t.co/VyyIJZO8E2
In their new Forefront article, @joefigs2, @eric_t_roberts, Jessica Phelan, and Kenton Johnston from @HarvardChanSPH, @PennMedicine, and @WashU discuss how, as CMS sets its agenda under new leadership, there are critical opportunities to develop integrated care models for dual-eligible beneficiaries in non-integrated Medicare Advantage plans and traditional Medicare. One potential strategy, they write, is to consider expanding Medicaid-risk accountability to the flagship value-based payment model in traditional Medicare—the Medicare accountable care organizations. https://t.co/ky9ClEoB8Y