Professor and Chief of Vascular Surgery @michiganstateu, Chair of @VascularSVS Clinical Practice Council, proud mom of two daughters 🐶 Tweets are my own
the anthropic claude for finance lecture is the best free hour in quant AI right now.
bookmark & watch today. It's the most valuable 1 hour in quant AI right now. Then read article below.
BREAKING: A Shelter in Place has been issued in Austin, Texas after 10, yes 10 shootings have taken place since yesterday, which appear to be related.
Multiple people are injured, and there is no information on possible motives. The shootings appear to be random in nature.
Suspects are in their late teens.
A pediatrician added up the hours she had donated to her medical school as a volunteer clinical professor.
Over 2,000.
That is more than a full year of full-time work. Donated. While running clinic, holding leadership roles, and raising three kids. She did not realize what she had done until she ran the math.
This is the conversation about physician burnout that almost never happens.
The wellness committees, the lectures, the residency teaching, the charting at 11 PM, the "leadership" calls at 6 AM, the committee work that gets quietly assigned to whoever will not say no. We call it professionalism. Jessie Mahoney, pediatrician and physician coach, calls it what it is: unpaid labor that has been normalized into the definition of being a "good doctor."
Three things from her argument worth bookmarking:
1. Volunteer work is not generosity if it is expected. It is obligation. The two are not the same thing and medicine has confused them for a generation.
2. The entire medical education system, the clinic schedule, and the leadership pipeline depend on this donated time. Nobody could finish their actual paid job inside their actual paid hours. Not even AI, in her words, could close the gap. The system requires the donation, and trains physicians to feel guilty if they refuse.
3. Nurses do not do this. They get overtime. Mahoney says on the show that she knows of no other profession where people just donate this much time. The physician unpaid-labor norm is a profession-specific defect, not a universal feature of skilled work. We invented it. We can uninvent it.
Her practical line for declining without burning the relationship: "I wish I could, but I don't have capacity for that." Then offer a trade. Time. Compensation. A slot replacing something else. Anything that makes the cost visible.
She also reminds physicians of a useful question to run before saying yes to the next "voluntary" ask: will your future self wish you had spoken up?
One historical note from the show worth holding onto: residency work hours did not get capped because the profession decided to cap them. They got capped because of a lawsuit. The voluntary hours, the unpaid teaching, the off-the-clock leadership, the chart-after-bedtime time, none of that has even been named yet, let alone budgeted. If history is the guide, that floor will not get built voluntarily either.
One more piece of context Mahoney raised on the show: roughly 60 percent of the physician workforce is now women. The unpaid-labor norm was built in an era when it was structurally easier to absorb. It is not that era anymore. The math on who is actually doing the donated work and what they are absorbing at home has changed, and the profession has not caught up.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
How many unpaid hours did you donate last year? #ThePodcastbyKevinMD
Same hospital. Same training. Same contracted hours. Same patients.
If one physician is a man and one is a woman, she earns $21,000 less per year.
That is the result when you control for every confounder administrators use to explain the physician pay gap away.
A recent analysis ran the numbers on emergency medicine and the story got worse at every cut of the data:
Hourly pay, adjusted for workload: women earn $17 less per hour.
Mid-career: $28,000 less per year.
Late career: $40,000 less per year.
Under productivity-based pay: $59,000 less per year.
Over a full career, the compounded lost earnings land between $600,000 and $1,000,000. That is the house, the college tuition, the retirement account that gender quietly stripped.
Jake Horowitz told KevinMD that the male physician replies to this data read like a script. "Not in my hospital." "You must have controlled for hours wrong." "I have never seen that happen." He said the denial itself is the story. These studies have been published in JAMA and Doximity for 25 years. The numbers have not moved.
Emergency physician Resa E. Lewiss offered the remedy: a personal board of directors to pressure-test your compensation, a willingness to publish the gap when internal channels fail, and organizational accountability enforced by medical professional bodies with the power that individuals do not have.
One more point Resa raised that did not appear in the dataset: intersectionality. Race and ethnicity were not in this analysis. When historical studies have run those numbers, the salary disparities are even worse. The $21,000 baseline is an aggregate. For many women in this profession, the actual number is larger.
Jake Horowitz, who is not a physician, framed the stakes in terms every patient should understand. When you walk into an emergency department, you want a doctor who is focused, well-paid, and treated fairly. What you do not want is a doctor who has spent a decade watching the male colleague down the hall earn more for identical work while the institution insists the gap does not exist. That is not a personnel issue. That is a patient safety issue.
Bookmark this. The next time a health system tells you they "fixed this years ago," you will have the receipt to prove that the published academic literature has said otherwise for a quarter century and counting.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
If you are a female physician who found out a male colleague earns more, what did you do next?
#ThePodcastbyKevinMD
Same hospital. Same training. Same contracted hours. Same patients.
If one physician is a man and one is a woman, she earns $21,000 less per year.
That is the result when you control for every confounder administrators use to explain the physician pay gap away.
A recent analysis ran the numbers on emergency medicine and the story got worse at every cut of the data:
Hourly pay, adjusted for workload: women earn $17 less per hour.
Mid-career: $28,000 less per year.
Late career: $40,000 less per year.
Under productivity-based pay: $59,000 less per year.
Over a full career, the compounded lost earnings land between $600,000 and $1,000,000. That is the house, the college tuition, the retirement account that gender quietly stripped.
Jake Horowitz told KevinMD that the male physician replies to this data read like a script. "Not in my hospital." "You must have controlled for hours wrong." "I have never seen that happen." He said the denial itself is the story. These studies have been published in JAMA and Doximity for 25 years. The numbers have not moved.
Emergency physician Resa E. Lewiss offered the remedy: a personal board of directors to pressure-test your compensation, a willingness to publish the gap when internal channels fail, and organizational accountability enforced by medical professional bodies with the power that individuals do not have.
One more point Resa raised that did not appear in the dataset: intersectionality. Race and ethnicity were not in this analysis. When historical studies have run those numbers, the salary disparities are even worse. The $21,000 baseline is an aggregate. For many women in this profession, the actual number is larger.
Jake Horowitz, who is not a physician, framed the stakes in terms every patient should understand. When you walk into an emergency department, you want a doctor who is focused, well-paid, and treated fairly. What you do not want is a doctor who has spent a decade watching the male colleague down the hall earn more for identical work while the institution insists the gap does not exist. That is not a personnel issue. That is a patient safety issue.
Bookmark this. The next time a health system tells you they "fixed this years ago," you will have the receipt to prove that the published academic literature has said otherwise for a quarter century and counting.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
If you are a female physician who found out a male colleague earns more, what did you do next?
#ThePodcastbyKevinMD
Vascular surgery is an essential yet overlooked part of healthcare systems. It drives better outcomes, reduces complications and generates revenue—all while enabling higher-acuity care across service lines. Learn more: https://t.co/9Oj2djVkAT #HighwaytoHealth#BeckersHealthcare
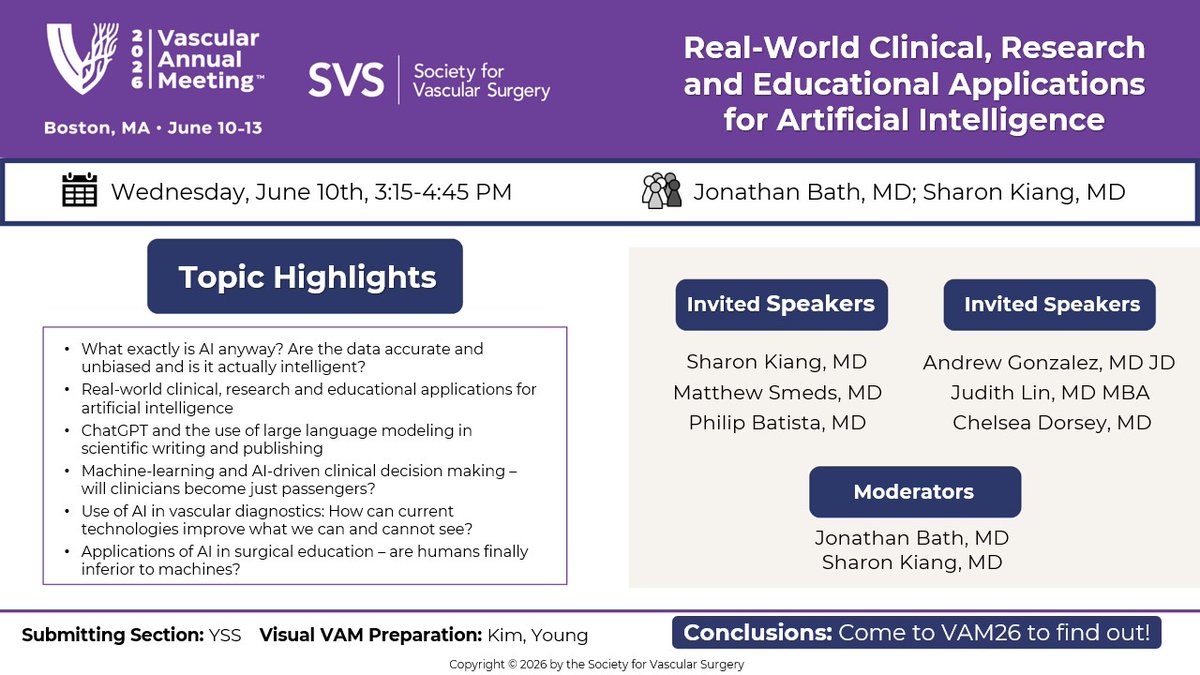
This week’s #VAM26 Visual VAM highlights a session focused on real-world clinical, research and educational applications of artificial intelligence.
🔗 Register today: https://t.co/3nEG2cLyji
#VascSurg#AI#ChatGPT@YoungKimMD
JUST IN: 🇨🇳🇹🇼 26 Chinese warplanes and multiple naval vessels detected near Taiwan, signaling the return of Beijing’s military pressure after a two-week pause.
Source: Reuters, ShanghaiEye
🚀 Join us at #VAM26 for a unique opportunity to dive further into vascular surgery while learning from the leaders advancing the field, discovering the latest research and exploring new technologies.
📅 Boston, MA | June 10-13
�� Register: https://t.co/bA6o4OGHXx #VascSurg
BREAKING: Authorities are responding after shots were fired at a synagogue in West Bloomfield, Michigan, according to the Oakland County Sheriff's Office.
Read more: https://t.co/JLypLdwbCg
URGENT‼️CLASS ACTION LAWSUIT🙏 PLEASE SHARE.
I know 30+ doctors who have died by suicide in these so-called "physician health programs" and now 2 brave physicians have filed a class-action lawsuit against the WPHP Washington Physician Health Program (one of the most aggressive at violating the rights of doctors who need CARE & not discipline and financial extortion).
In short, WPHP has placed profit ahead of participant safety and recovery, imposed requirements that lack foundation in evidence-based science and standards, obstructed access to records and other participant information, and interfered with Plaintiffs’ and Class Members’ ability to work. This has resulted in significant harm to Plaintiffs and the Class.
Plaintiffs both graduated from medical school. Both were well into their residency programs, on their way to becoming fully-fledged doctors ready to help the Washington community, when they were trapped by WPHP. Rather than helping Plaintiffs, WPHP upended their lives and careers.
Today, neither of these doctors remains in their residency programs at the University of Washington (“UW”). They have both lost years of their careers as doctors, and our community has lost years of their service, because WPHP held them prisoner, acting as their judge, jury, and jailer.
If you wish to be part of this class action lawsuit or want to read the 24-page legal document or need any help at all please reach out to me (happen to be hosting a free retreat in East Lansing Michigan this weekend if you want to join us). https://t.co/3C804pd3fH
May God bless these 2 courageous physicians for standing up for their human rights and for the rights of all vulnerable doctors who end up punished for seeking mental health help. ❤️🩹
PLEASE SHARE. 🙏
A suspect is dead after a shooting and vehicle ramming incident at a Detroit-area synagogue, according to the FBI, which said it is investigating the incident as a targeted act of violence against the Jewish community.
"If you think you can target the Jewish community in this county or anywhere in this state, you're wrong," said Oakland County Sheriff Michael Bouchard.
Read more: https://t.co/gJSQlRB2zt
BREAKING: 31% of all hospice and home health companies in the U.S. are registered in L.A. County, and they receive millions in taxpayer money.
So I went to the addresses listed in the Valley.
What I found: No clinics. No patients. No healthcare providers.
Just vacant offices.
To all Michiganders currently in Mexico: please sign up for the Smart Traveler Enrollment Program if you haven’t yet. This program will allow the State Dept. to quickly contact you in case of an emergency.
https://t.co/MwZAKoaUoW
@docpark@jmills1955@HeartOTXHeartMD I remember doing 3-5 appendectomy each night on call at a level I trauma hospital in NYC. It’s great if we can manage with IV antibiotics for acute appendicitis. It’s bad for surgical training.
NCSD will be closed on Thursday, January 15, 2026 due to treacherous road conditions and declining temperatures. Updates on afterschool activities will be communicated midday by those who oversee those activities.