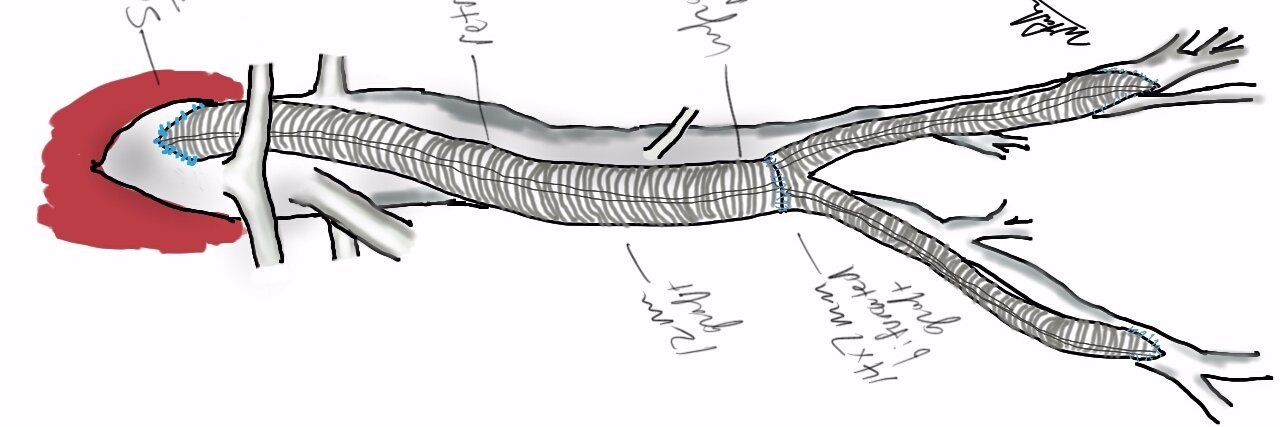
this operation still works -ABF for a small AAA and iliac occlusive disease. #vascsurg Also, Becker's Health posted an article predicting a 38% shortfall of vascular surgeons in a decade!
@ShooterMcGavin practice hitting a 5 iron flipped around left handed -its a useful skill and in this situation, its really just a medium rap with that set up. or one handed backwards putter.
@NUCLRGOLF its a sign of an anguished mind and depends on context. for professsional golf, there should be penalties related to broadcast windows and lost revenues, etc. for country club golf, it's a letter in your locker and loss of tee time privileges. for public golf, there is nothing.
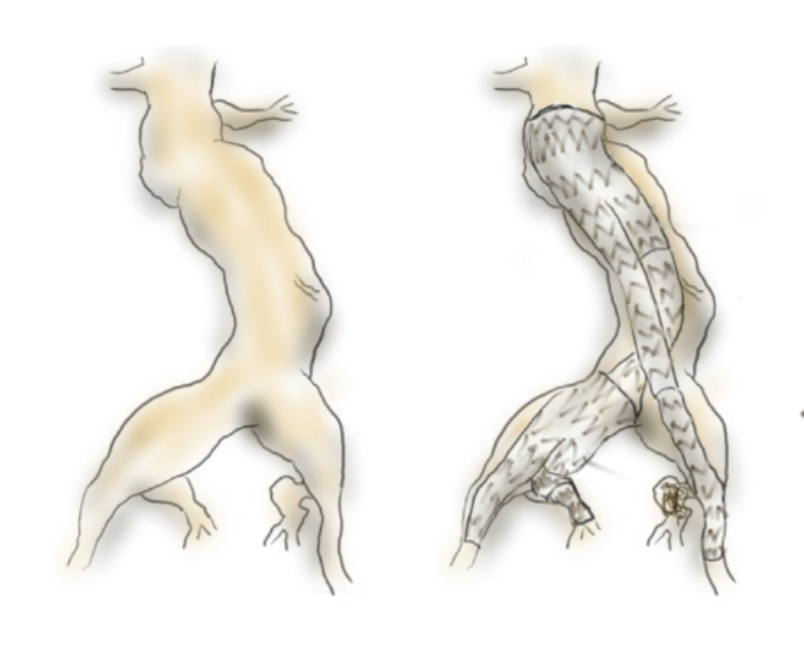
With bilateral CIAA, I still tend to coil and cover one side particularly if suboptimal and IBE the other. Do #vascsurg see a benefit to doing both -ie. bil. IBE?
Amazing patient-centered (and lost new surgeon-centered) signage and map system!!
Type in where you are trying to go and you get a dynamic map AND a link for your phone.
Wow
@UHhospitals
I've only recently seen the @WithAScalpel account, but it is immediately obvious that it has a steady output of high-quality visual teaching aids related to pediatric cardiac surgery and physiology, and also some general technical pointers. It should have WAY more followers. 🧐
I debated not showing up and shouting "April fools!" if someone called me, but instead have officially started and am thrilled to report I was welcomed by 10,000hrs of Epic training.
@SCVS1969 breakfast session. Just heard an insanely cool technique to treat an extent III TAAA with tiny access vessels via transcaval access.
Laser to cross from IVC to Aorta, dilate, place large TAMBE access and deploy.
"Fishing pole" retrograde cannulation + AFX via arterial
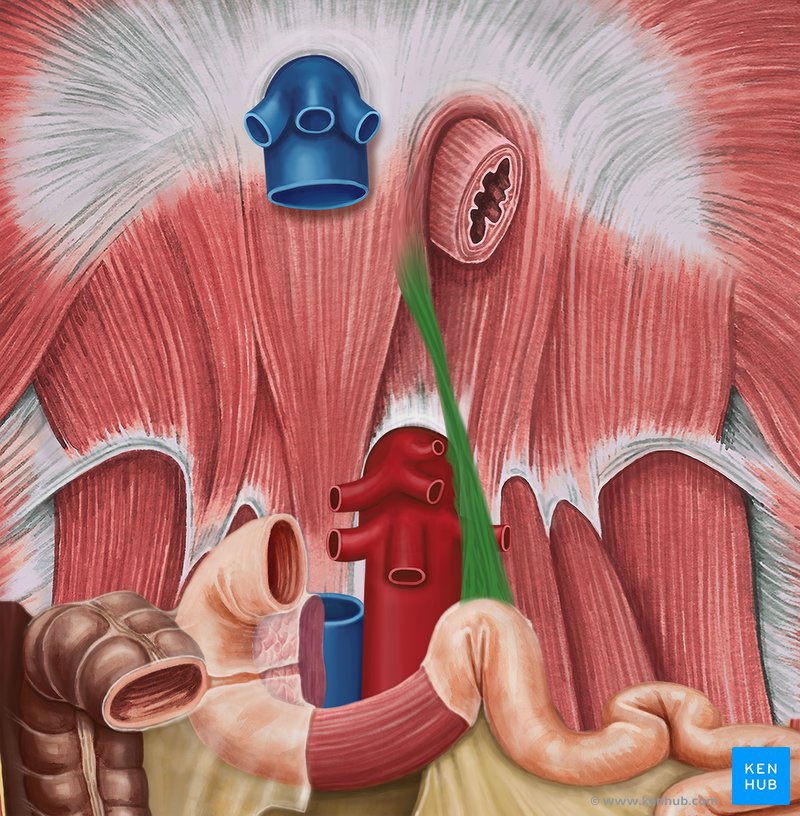
Ever wondered why surgeons obsess over a tiny “ligament” that’s actually a clever muscle hybrid hanging from your diaphragm?
It quietly divides your gut’s bleeding zones and keeps your small bowel from twisting into chaos!
The Ligament of Treitz—more accurately termed the suspensory muscle of the duodenum—marks the precise anatomical transition from the duodenum to the jejunum at the duodenojejunal flexure.
Far from a simple collagenous ligament as its name suggests, this fibromuscular structure comprises a superior portion of skeletal (striated) muscle fibres arising from the right crus of the diaphragm, blending into connective tissue near the coeliac artery, and an inferior part of smooth muscle fibres originating from the third and fourth duodenal segments.
This unique composition allows it to suspend and stabilise the flexure, widening the angle during contraction to facilitate smooth passage of intestinal contents into the mobile jejunum.
Clinically, it serves as a critical landmark: bleeding proximal to the ligament is classified as upper GI (often presenting as haematemesis or melaena), while distal bleeding counts as lower GI (typically haematochezia).
Surgeons rely on it during laparotomy to identify the jejunum for procedures like feeding jejunostomy or measuring bowel length.