For Cardiologists in India #ACC#AHA
New Orleans should be marked as the most scientific meet.
Disproved role of
1. Impella in STEMI
2. Impella in CHIP
3. LAAC vs OAC
4. CTO interventions
All of us from the third world shouldn’t have FOMO. It’s all industry driven there
Median family income in the US increased from $10,000 in 1971 to $106,000 today, a 10x increase.
However, the median cost of homes increased from $25,000 to $445,000, a 17x increase.
And the median cost of cars increased from $3,600 to $50,000, a 14x increase.
The median cost of college increased from $2,900 a year to $45,000, a 16x increase.
And the average cost of healthcare per person increased from $350 to $14,600, a 42x increase.
THIS IS ABSOLUTELY INSANE.
@legen_eth money isn’t everything but having money lessens day to day burden and stress of necessities especially when it can afford wants without blinking. people don’t want to/need to be billionaires or even multi millionaires, they want luxury of not having to look at their bank account
@docmartin22@ValerieAnne1970 doesn’t fit the narrative. simply posting this and believers taking it as hard science and fact. actual data dredging takes work and effort. even @grok discuses lower risk with vaccine 🤦♂️
@RetsefL keeps peddling this lie. Why not acknowledge the USA tried the targeted approach first and it failed?
In 1982, the CDC recommended a birth dose for all babies born to mothers infected with hepatitis B virus. That recommendation did nothing to change rates.
In 1988, the CDC expanded the birth dose to include racial & ethnic groups at highest risk of hepatitis B virus infection (Alaskan Natives and Southeast Asian refugees). That didn't do much either.
So they moved to a universal recommendation in 1991 and that's when we finally saw a real change.
After the 1991 recommendation for universal infant vaccination, coverage in young children rapidly approached about 90% by 2000, and infection prevalence in children fell by roughly two‑thirds to four‑fifths within a decade.
If safer injection, blood screenings & and safer sex were the main causes, you would see similar proportional declines in older, mostly unvaccinated adults but you do not.
Instead, the steepest drops are in vaccinated children & adolescents, while older unvaccinated adults retain higher incidence & chronic infection rates, which directly contradicts the claim that other interventions drove the decline.
Acute Hep-B incidence began falling in the mid-1990s among children as 1991+ birth cohorts entered reporting ages (for example 4-5 by 1995-96), with overall cases dropping 99% in kids/teens over two decades due to birth dosing!
Birth-dose coverage hit ~80% by 1994 and >90% soon after.
Perinatal and early childhood transmission (the main routes in kids) were blocked from day one by the birth dose + series.
By 2005, the age 11 group (born around 1994) largely received birth doses post-1991 rollout, while age 15 (born around 1990) mixed pre/post-policy births but benefited from early series completion enabled by birth dosing, which boosted full immunization rates.
The big drop in pediatric rates happened exactly when the first vaccinated cohorts entered those age groups, not years later.
CDC data confirm plummeting perinatal infections from thousands to single/low-double digits after 1991, directly tied to birth doses reducing transmission by around 70% alone (83-97% with immune globulin), with protection lasting 35+ years.
THIS IS HOW SCIENCE WORKS
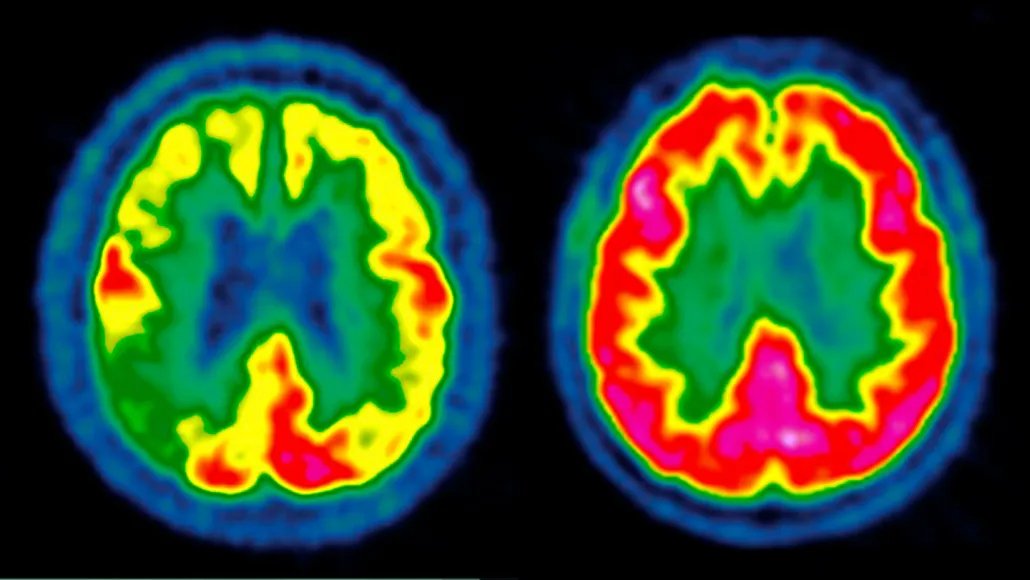
Two huge clinical trials just delivered bad news:
GLP-1 drugs - the Ozempic-style “miracle meds” - failed to slow Alzheimer’s.
Yes, failed.
And this is exactly what real science looks like.
For years, anecdotal reports + early studies hinted at something exciting:
• People said they felt “sharper” on GLP-1s.
• Small trials hinted at cognitive benefits.
• Animal studies looked promising.
• Real-world data suggested protection.
Hope was real - and reasonable.
But hope ≠ evidence.
So scientists did what responsible scientists do:
They ran two massive, well-designed, placebo-controlled trials.
Nearly 4,000 patients, followed for two years, all early-stage Alzheimer’s.
The question:
Can semaglutide actually slow the disease?
The answer: No. Not in this population, not at this dose, not in this form.
There were tiny biomarker changes - signals that something might be happening biologically.
But clinically?
Zero difference.
No better memory.
No slower decline.
No measurable benefit.
A clean, unambiguous result.
That’s what gold-standard data does: it cuts through noise.
And yes - this is disappointing.
Researchers who helped invent GLP-1s hoped this would work.
Patients hoped.
Families hoped.
But science doesn’t care about hype or headlines.
It cares about truth.
And today’s truth is simple:
GLP-1s don’t slow Alzheimer’s - at least not like this.
Is this the end?
Not at all.
Scientists are already asking the next questions:
• Wrong dose?
• Wrong timing?
• Wrong population?
• Not enough drug reaching the brain?
• Maybe GLP-1s help prevent, not treat?
• Or maybe we need better molecules entirely?
Each “failure” narrows the path toward a breakthrough.
This is the opposite of pseudoscience.
No excuses.
No YouTube gurus.
No cherry-picking.
Just data → conclusion → next hypothesis.
It’s slow.
It’s painful.
It’s frustrating.
But it’s honest.
The Alzheimer’s field didn’t collapse today.
It adjusted.
It recalibrated.
It moved forward.
Real science isn’t a straight line.
It’s a messy, disciplined climb toward answers that actually help people - not ones we wish were true.
So yes, GLP-1s stumbled.
And that’s fine.
Because this is how science works:
We test big ideas.
Most fail.
Some don’t.
But every trial - even the disappointing ones - pushes us closer to something that will work.
Putting “no risk” in all caps does not magically turn it into a medical fact. The newborn Hep B recommendation exists because when transmission does occur—especially undetected maternal infections—the outcomes are catastrophic. That’s why every major medical association supported universal vaccination, and why countries that tried selective screening ended up reversing course once preventable infections surged. Pretending the ACIP vote is a triumph of science instead of the result of political pressure and a gutted advisory process is the sort of thing you say when you want to cosplay as a public health visionary without doing any of the work.
And the idea that the childhood vaccine schedule has been some reckless gauntlet of “72 jabs” is a talking point straight out of Famine’s merch store. It deliberately ignores dose grouping, decades of safety data, and the basic reality that vaccines replaced the diseases that used to fill pediatric ICUs. If this administration’s new strategy is “other countries do less, so maybe we should too,” then buckle up, because that logic works great until the outbreaks arrive. Science is not a vibe check, and national health policy should not be reverse-engineered from the comments section.
dark days ahead with rise in diseases that were suppressed minimized with current standards. darwin said it best and we will c some of this pan out in decades to come. reversing decades of progress in one fell swoop. what a time we live in