Check out our latest commentary on the FONDUE trial, provided by Dr. Georg Schmölzer and Dr. Brenda Law: When does neonatal resuscitation end and NICU respiratory support begin? @CNN_EPIQ
Once residency/fellowship applicants can safely acknowledge their lack of interest in conducting research without torching their job prospects, then we will have entered a new utopia with the perfect balance of physicians, scientists, and physician-scientists. It will be beautiful.
Is atropine really required in addition to fentanyl & succinylcholine prior to intubation to prevent severe bradycardia in neonates?
We found yes...
Severe bradycardia during the whole procedure was signif > in placebo vs atropine group; RR 6.3(95% CI 1.2 - 34.1)
#neotwitter
So true, but sometimes hard to convince your teammates (including parents) that supportive care, patience and time are usually the best courses of action for our preemies.
If you look back at all the research and experience in Neonatology over the past 30 years, what is the main message that emerges? IMO it is “Less is More”. We used to think that more intervention is better, and more aggressive, earlier interventions are better. Instead we have learned the opposite is true.
#neotwitter
In infants born preterm, dexamethasone is associated with improved survival free of cerebral palsy when the risk of bronchopulmonary dysplasia (BPD) exceeds 70%.
As with any medication, it all comes down to risks versus benefits
https://t.co/NU0n2BYf67
#neoTwitter
I visited a NICU once where the staff of the NICU included family practice physicians and psychologists, in addition to the usual neonatologists, nurse practitioners, nurses, RTs, SW, others.
The FP docs' and psychologists' role was to evaluate and treat the health of the parents of the baby (and grandparents as required). They had four outpatient clinics adjacent to the NICU where they provided these services.
Working with the parents' existing physicians if any, they reviewed the prior medical and mental-health history of the parents, treated existing medical problems (such as high BP, diabetes, substance abuse).
They ensured that all their preventive care was up to date, provided counseling about life-style, exercise, mental well-being, smoking cessation, stress management and so on. If the siblings of the baby needed health evaluation and services, these were provided also.
These services for the parents were provided because the leaders of this particular NICU believed that ensuring the health and well-being of the parents was essential to ensuring the health of the baby after discharge. The baby was not treated in isolation separate from the family.
This of course is a fictional NICU. I do not know of any NICU in the world that provides medical care for parents, siblings. But imagine how ideal it would be if we were to provide such care for the entire family unit. And not just for the baby.
#neotwitter #neonatology #NICU
I'm not tired of Trudeau and I voted NDP. I think 90% of the "tired of Trudeau" crap is media and CPC generated. The minority govt with NDP support is not perfect but it is far better than the right wing alternative.
PSA FOR FAMILIES
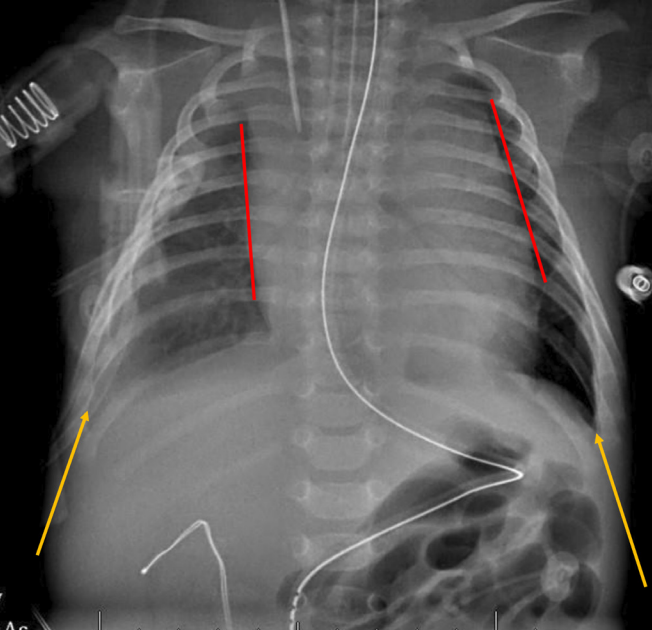
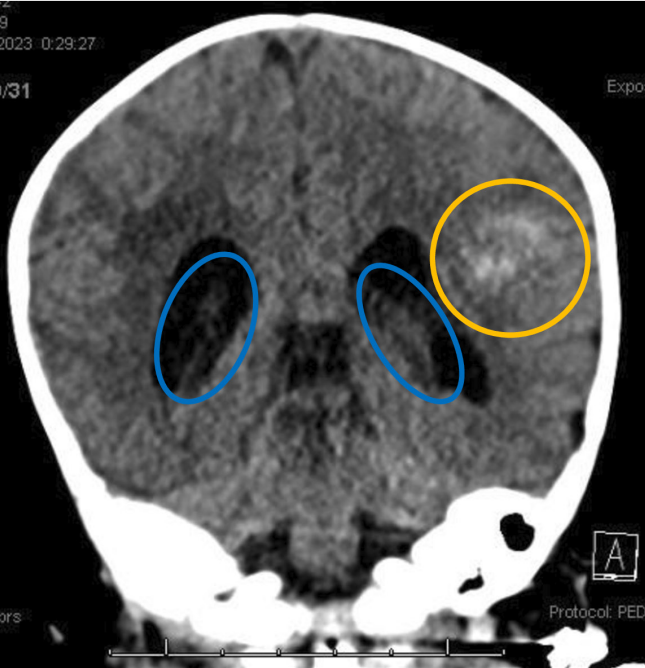
Late onset Vitamin K deficient bleeding in a 6-week-old
Hemorrhages 🩸 in
🤯Thymus
🤯Pleural space
🤯Brain: intraventricular & parenchymal
PREVENTABLE with IM Vitamin K after birth‼️
https://t.co/TxGGKLXfBZ
#neoTwitter
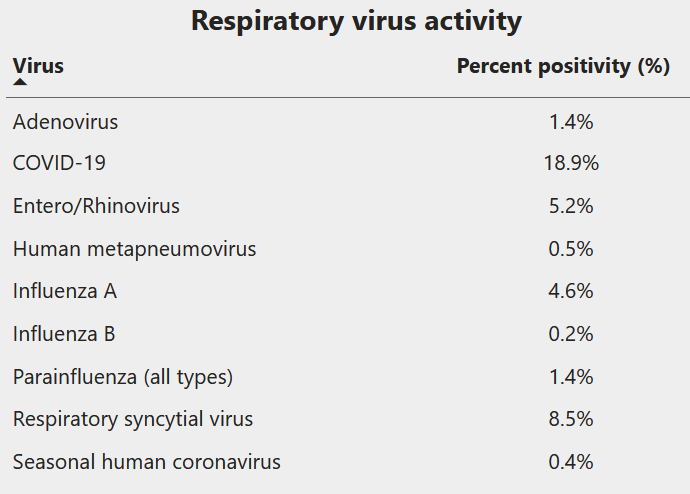
Once again seeing C19, Flu and other viral cases in huge numbers in the ER. Hardest hit are kids <2 and adults >65. Some advice for this season:
Use fever medications
- Every child with a high fever will look terrible. Keep ahead of it with Tylenol/Paracetamol and Advil/Ibuprofen
- Kids will often refuse solid food, but will still drink; give lots of fluids/electrolytes, especially after you bring down the fever. The appetite will usually recover after a day or two with the more benign viruses.
- most cold/flu meds (eg pseudoephedrine, benadryl) are not recommended or approved for kids <6
When to come to see your physician/come to the hospital
(not an exhaustive list)
- fever more than 4-5 days
- not eating/drinking
- lethargic/sleepy even with tylenol/advil
- not peeing, or peeing too much
- rapid or noisy breathing
- Any fever in a child <6 weeks, or in a chemo patient
- focal source of possible bacterial infection - ear pain (ear infection), severe sore throat (strep), pain on urination (UTI), etc.
- if you're worried
Do a Rapid Test
- It is a big help to your physicians to know if you're C19 positive or not. This could mean faster access to antivirals that could save a vulnerable patient's life, or at least prevent a hospitalization. It could also mean you're not prescribed unnecessary and possibly harmful antibiotics. It also helps you keep vulnerable babies or older relatives away from infected family members.
Prevention
- Mask wearing is not popular, but when used in poorly ventilated, crowded places (planes, trains, buses, hospitals, malls full of holiday shoppers) is a high yield activity that might spare you a lot of misery
- If you're sick with any cold symptoms, stay home, wear a mask if you need to go out. Spare someone else a lot of misery.
- It's a hard thing to ask, but don't go to the big family dinner and infect everyone if you're sick
- It's no longer 'brave' or a sign of hard work to show up sick to work. It's a terrible Christmas present that your colleagues will hate you for.
- Get boosted (for C19, flu, and RSV if available), will hopefully prevent some infection and ensure a milder course of illness for most.
To give you an idea of what's circulating out there (in Ontario, Canada) for now:
There are a lot of myths — and straight up bullshit — circulating about gender affirming care.
Let’s debunk some common misconceptions so you can help your loved ones and friends understand the facts.