Eco🫀: Índice de Abbas. 💢🫁
🔷️El índice de Abbas es un método ecocardiográfico Doppler utilizado para estimar de forma no invasiva la resistencia vascular pulmonar, un parámetro clave en la evaluación de HP y Enf. Vascular pulmonar. En 2003 Abbas et al, realizaron la siguiente formula:
🔷️Fórmula original = Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD).
🔹️Resultados: normal <0.15 / Elevado >0.175; correlación con >2 UW [S: 77%, E: 81%].
🔹️La VRT refleja el gradiente de presión entre VD y AD ➡️ aumenta cuando existe HP. La IVT TSVD refleja el volumen sistólico y flujo pulmonar.
🔹️Al dividir ambos parámetros se obtiene una aproximación de la relación presión / flujo ➡️ base hemodinámica de la RVP.
🔷️Fórmula modificada para convertir a UW = [Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD) x 10] + 0.16
🔴 >2 UW ➡️ HP precapilar. 🫁💥
https://t.co/nhVGJdZS1R
https://t.co/q5nO4Pi2ap
🔍 #EHRATopicWeek on Atrial Tachycardias
Atrial Tachycardia is more complex than we once thought
Traditionally, rapid regular atrial arrhythmias were divided into “atrial tachycardia” and “atrial flutter” based mainly on ECG appearance. Today, high-resolution mapping shows these distinctions are often oversimplified.
📌 Current concepts classify all regular atrial rhythms >100 bpm as AT:
• Non-reentrant AT
• Reentrant AT (localized or macro-reentrant)
Importantly, many arrhythmias previously labeled as “flutter” may actually represent different AT mechanisms.
⚡ Differentiating AT from organized AF can be challenging, especially in scarred atria or after ablation. ECGs, EP studies, intracardiac mapping, and even wearable devices all play an important role in diagnosis.
💡 Precise classification matters — for diagnosis, treatment strategy, and improving ablation outcomes.
Find out more in the #EHRA_ESC Consensus document on Management of patients with atrial tachycardia 🔗https://t.co/T5EGaHI51q
@escardio@EuropaceEiC
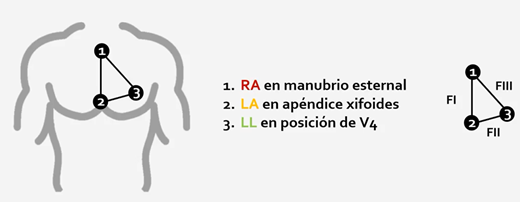
Derivaciones modificadas por Fontaine 👇
➡️Aumentan sensibilidad de ondas épsilon
➡️En ECG la onda épsilon es el hallazgo más específico pero sólo visto en 30% de los pacientes con displasia ventricular derecha arritmogénica
Functional ES mapping using EGM duration prolongation DeEP maps yielded highest accuracy in defining the arrhythmogenic substrate. The inclusion of latency or annotation of NF EGM components doesn't improve functional substrate mapping accuracy. https://t.co/UNaYgiLYm7 #JACCCEP
is EPICARDIAL ABLATION for flutters unnecessary in PFA times?... unfortunately we don´t think so... here we show an epicardial bridging after an anterior mitral line despite stacking RF (red)+ PFA (blue) below. Epi RF ablation worked
(PVI+PWI were performed right before, for persistent AF)
#EPeeps
Effects of Pacing Sites on Substrate Mapping Using Decrement-Evoked Potential Mapping for Scar-Related Ventricular Tachycardia #OpenAccess
https://t.co/GWYsXPKks1
‘Squeezing the atrial voltage map with a peak frequency tailored approach: when no one knows where the micro-reentrant circuit is’
https://t.co/x8Eno7wvMD
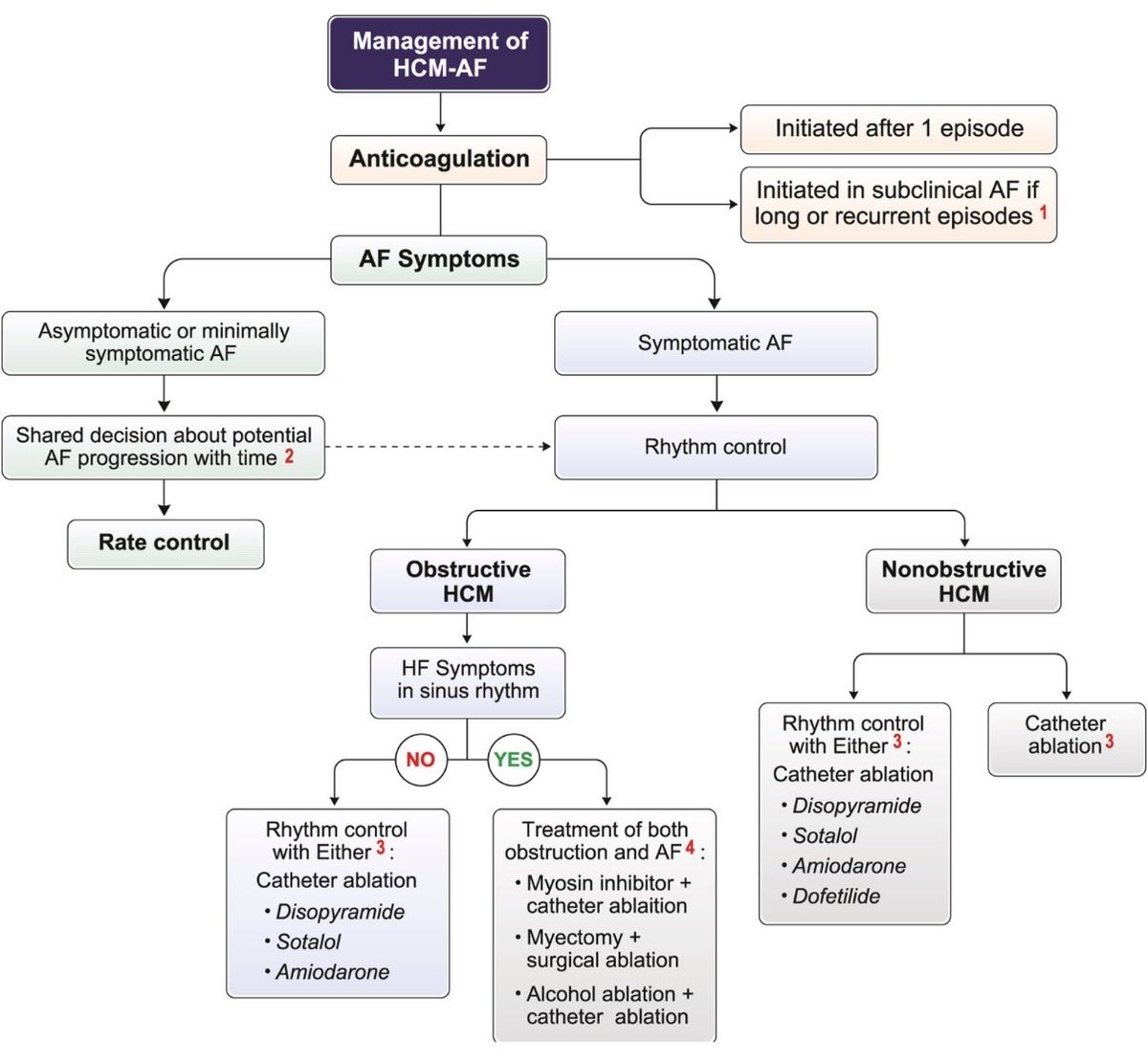
Anyone who has battled stubborn AF in HCM will benefit from reading this review we wrote with colleagues from multiple disciplines within the HCM community. @EthanRowin@MasriAhmadMD
Helpful workflow diagram below:
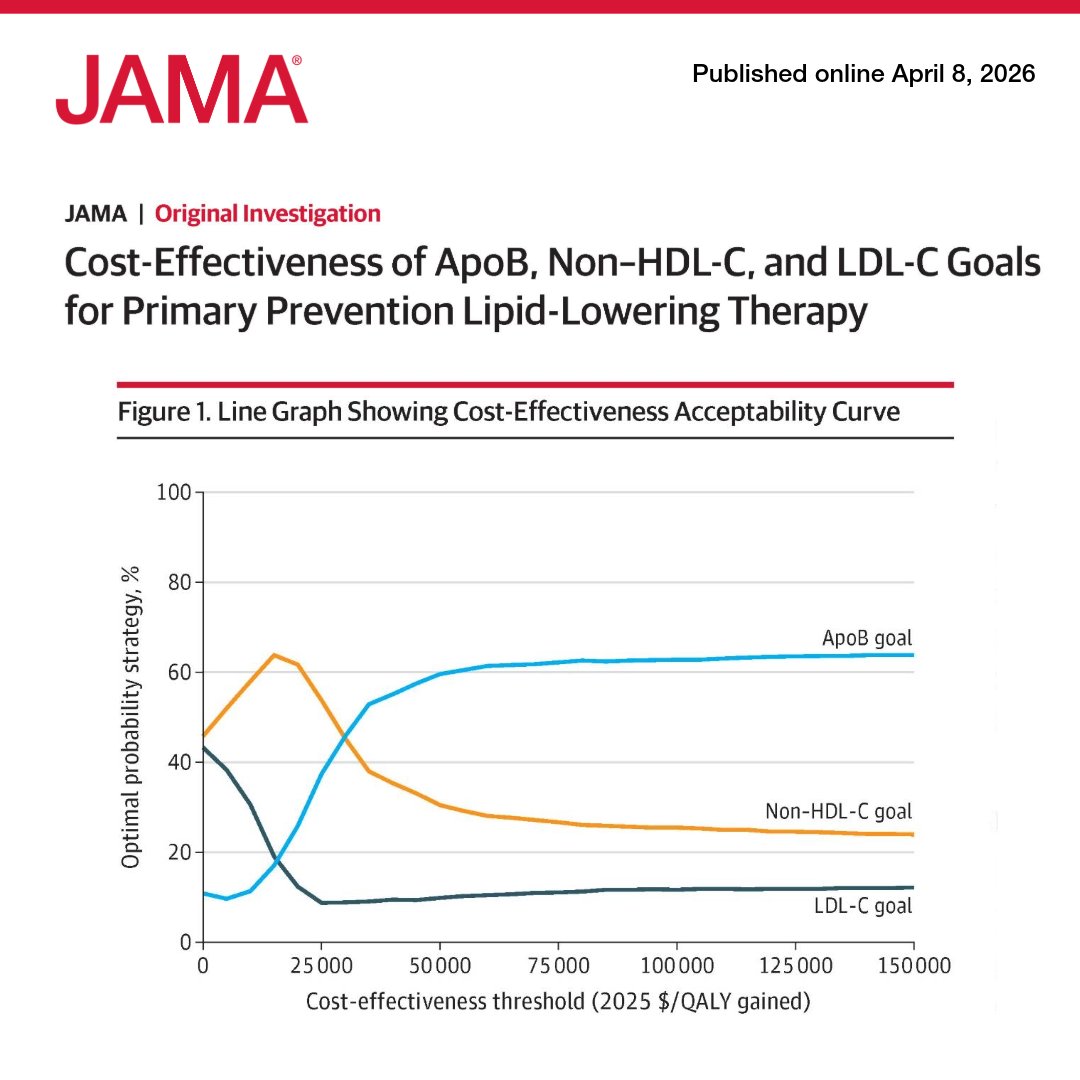
A computer simulation found #ApoB-guided intensification of lipid-lowering therapy provides the most QALYs and is highly cost-effective compared to #LDL-C or #nonHDL-C targets.
https://t.co/hu4lgTeKxV
So sorry to ruin the day of the Social Media cholesterol deniers. They have no clue that plasma cholesterol metrics have no relationship to cellular (including brain) cholesterol
👉 We spend decades arguing about how low to push LDL-C
👆 Almost no one asks the obvious question:
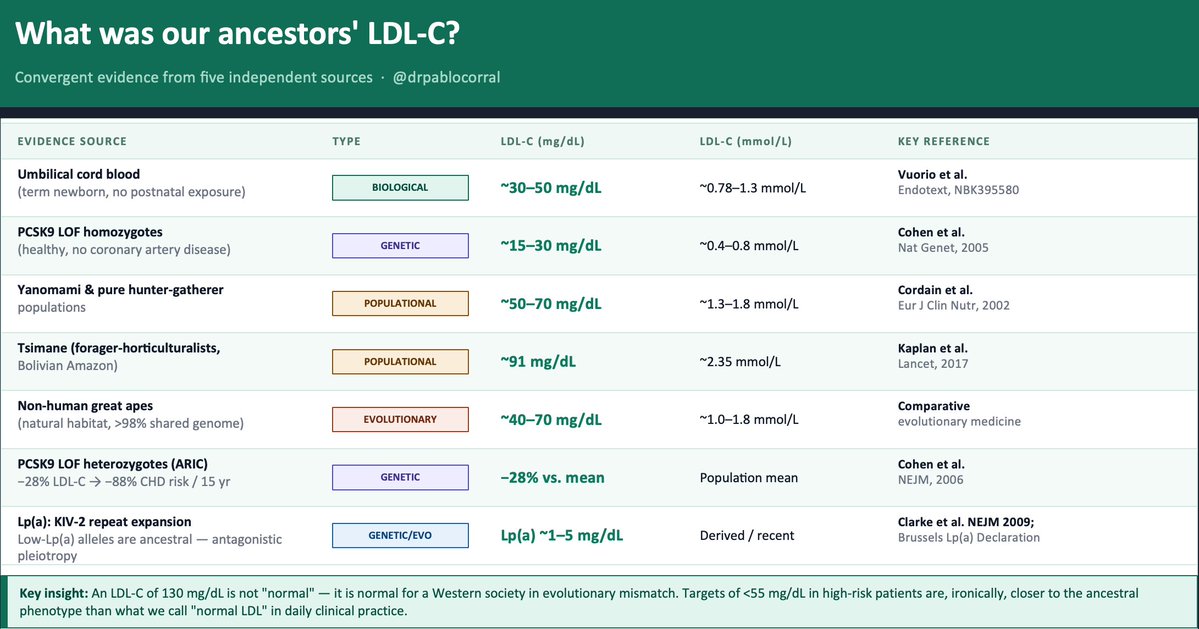
🤔 How much LDL-C did our ancestors actually have?
The evidence exists — five independent lines, all converging on the same uncomfortable answer.
1️⃣ The term newborn. Before any dietary or metabolic influence, a healthy neonate arrives with LDL-C of ~30–50 mg/dL. That is the LDLR operating without environmental interference. Everything that rises after birth is acquired.
2️⃣ The Tsimane (Kaplan et al., Lancet 2017) — forager-horticulturalists of the Bolivian Amazon — have a LDL-C between 70 to 90 mg/dL and the lowest prevalence of coronary atherosclerosis ever recorded in any human population. Five times less than the U.S. in adults over 75. And their LDL is rising as roads and processed food arrive.
3️⃣ PCSK9 loss-of-function variants. African American carriers of nonsense mutations (Y142X/C679X, ~2% frequency): −28% LDL-C and −88% CHD risk over 15 years (Cohen et al., NEJM 2006). Homozygous LOF carriers live with LDL-C of ~15–30 mg/dL. Perfectly healthy. Nature already ran the trial.
4️⃣ Evolutionary genetics. Recent positive selection signals exist on gain-of-function PCSK9 variants that raise LDL-C — likely adaptive in food-scarce ancestral environments. Modern hypercholesterolemia is not "normal." It is an ancestral survival advantage turned pathological by evolutionary mismatch.
5️⃣ Great apes in natural habitat: ~40–70 mg/dL LDL-C. Same genome. Different environment.
👆 Bonus — Lp(a). The KIV-2 repeat expansion that raises Lp(a) is a derived, recent variant. Low-Lp(a) alleles are ancestral. Elevated Lp(a) is a textbook antagonistic pleiotropy signal — possibly protective against bleeding early in life, atherogenic over decades
📍The convergent estimate: ancestral LDL-C was ~30–70 mg/dL.
📍An LDL-C of 130 mg/dL is not "normal." It is normal for a Western society in evolutionary mismatch. Targets of <55 mg/dL in high-risk patients — which still feel aggressive to many clinicians — are, ironically, closer to the ancestral phenotype than what we call "normal LDL" in daily practice.
🤔 The question is not "is it safe to lower LDL this much?"
The question is: why did we let it rise this high?
@society_eas@nationallipid
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
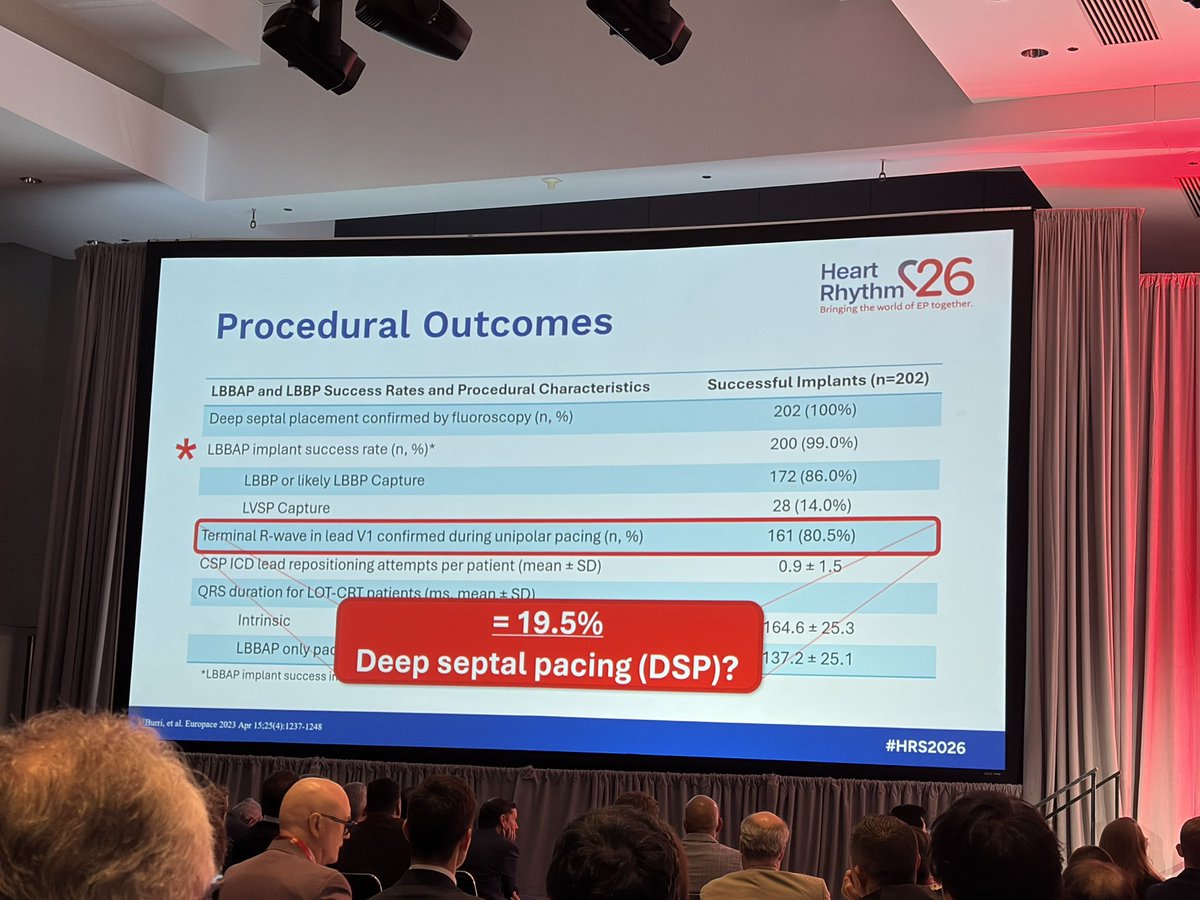
💡 After 5 years from early Steering Committee discussions, our PhysioSync-HF trial was published this March in @JAMACardio, with a simultaneous editorial and coverage across Medscape and ACC News
Hot topic 🔥 who benefits from CRT — and the fundamental importance of achieving adequate capture in conduction system pacing
Grateful to be part of this effort to improve care for patients with #HeartFailure🫀

![javier20ch's tweet photo. Eco🫀: Índice de Abbas. 💢🫁
🔷️El índice de Abbas es un método ecocardiográfico Doppler utilizado para estimar de forma no invasiva la resistencia vascular pulmonar, un parámetro clave en la evaluación de HP y Enf. Vascular pulmonar. En 2003 Abbas et al, realizaron la siguiente formula:
🔷️Fórmula original = Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD).
🔹️Resultados: normal <0.15 / Elevado >0.175; correlación con >2 UW [S: 77%, E: 81%].
🔹️La VRT refleja el gradiente de presión entre VD y AD ➡️ aumenta cuando existe HP. La IVT TSVD refleja el volumen sistólico y flujo pulmonar.
🔹️Al dividir ambos parámetros se obtiene una aproximación de la relación presión / flujo ➡️ base hemodinámica de la RVP.
🔷️Fórmula modificada para convertir a UW = [Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD) x 10] + 0.16
🔴 >2 UW ➡️ HP precapilar. 🫁💥
https://t.co/nhVGJdZS1R
https://t.co/q5nO4Pi2ap](https://pbs.twimg.com/media/HI4qNGsW4AENj6L.jpg)



























![javier20ch's tweet photo. Eco🫀: Índice de Abbas. 💢🫁
🔷️El índice de Abbas es un método ecocardiográfico Doppler utilizado para estimar de forma no invasiva la resistencia vascular pulmonar, un parámetro clave en la evaluación de HP y Enf. Vascular pulmonar. En 2003 Abbas et al, realizaron la siguiente formula:
🔷️Fórmula original = Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD).
🔹️Resultados: normal <0.15 / Elevado >0.175; correlación con >2 UW [S: 77%, E: 81%].
🔹️La VRT refleja el gradiente de presión entre VD y AD ➡️ aumenta cuando existe HP. La IVT TSVD refleja el volumen sistólico y flujo pulmonar.
🔹️Al dividir ambos parámetros se obtiene una aproximación de la relación presión / flujo ➡️ base hemodinámica de la RVP.
🔷️Fórmula modificada para convertir a UW = [Velocidad máxima de Regurgitación Tricuspídea (VRT) / IVT del Tracto de Salida del VD (IVT TSVD) x 10] + 0.16
🔴 >2 UW ➡️ HP precapilar. 🫁💥
https://t.co/nhVGJdZS1R
https://t.co/q5nO4Pi2ap](https://pbs.twimg.com/media/HI4qNHZXYAASQrT.jpg)