In a new study, Wachtendorf et al. investigated whether the introduction of sugammadex led to higher intraoperative rocuronium doses and whether this impacted postoperative respiratory complications.
💡 Learn more: https://t.co/JpuLK6Bvyx
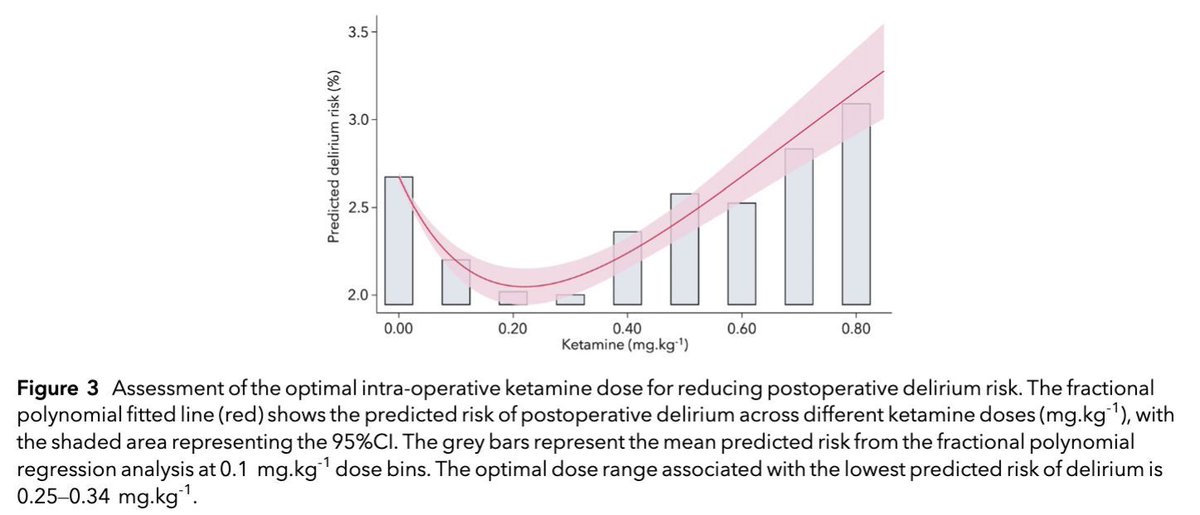
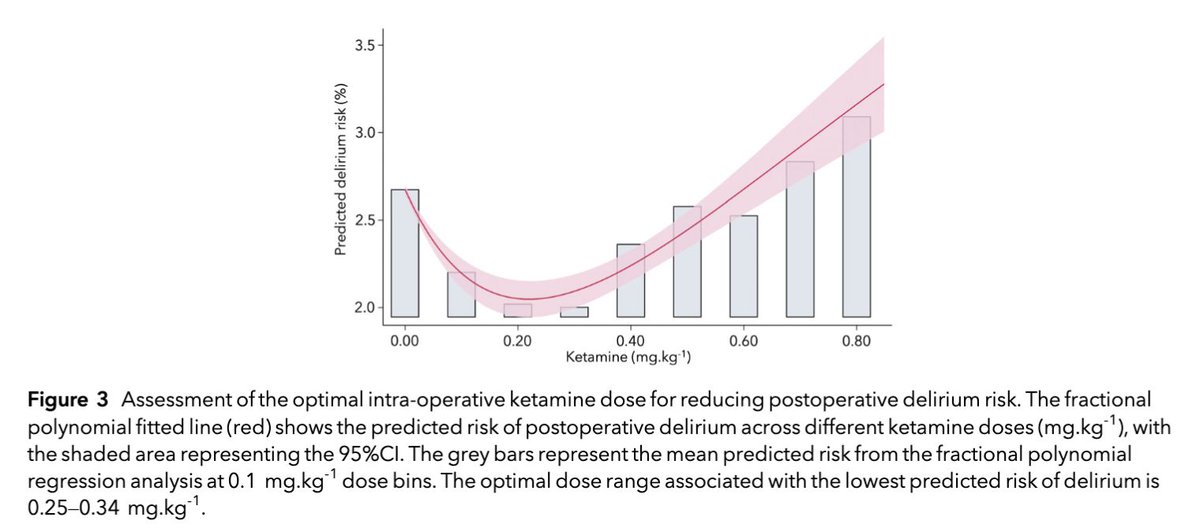
Giving a small dose of dexmedetomidine (between 0.25 and 0.35 micrograms per kilogram of body weight) during surgery may help reduce confusion afterwards but giving more than this does not seem to help.
#anaesthesia#MedTwitter
https://t.co/4TntCdEZf1
Association of intraoperative dexamethasone administration with postoperative delirium and the role of hyperglycaemia
Intraoperative dexamethasone was associated with lower risk of postoperative #delirium, but not in patients with hyperglycaemia
https://t.co/p8uLh0C6vp
We use too much rocuronium. Because we follow the temptation to use sugammadex reversal without measuring neuromuscular transmission function. Too much compliance with industry interests - 🤟clinician scientists @ASAMonitor @MontefioreSurg https://t.co/z9PkMuPr1q
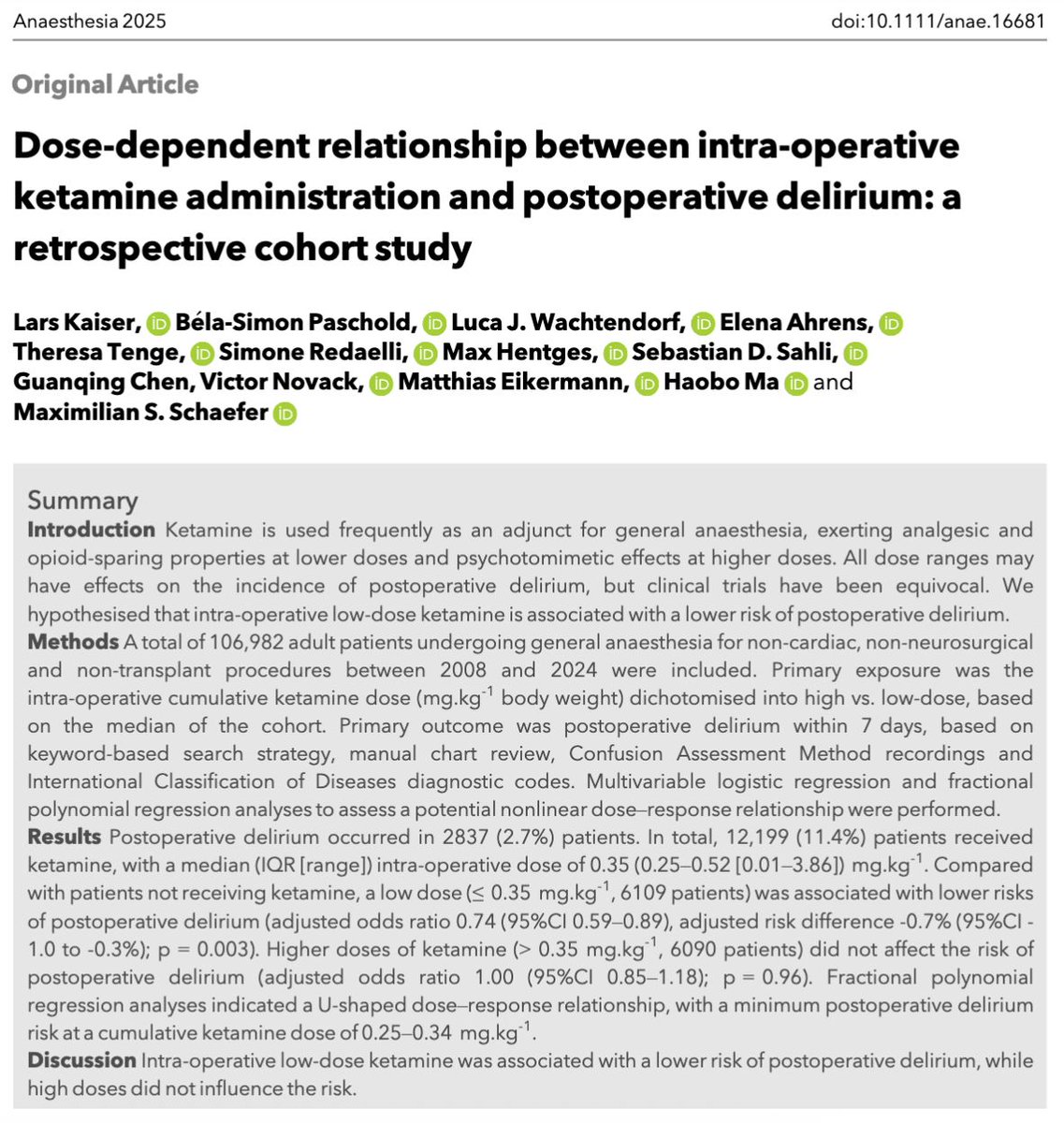
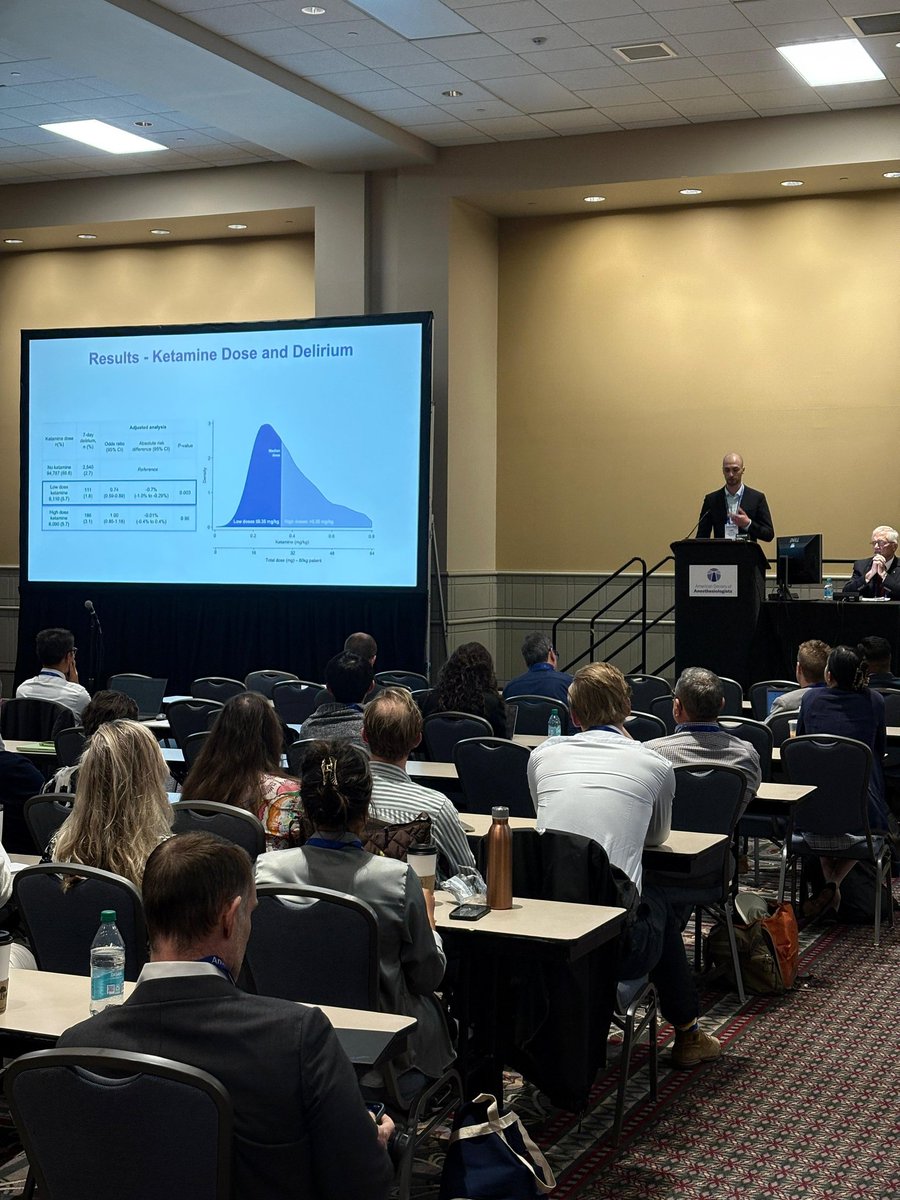
Intra-operative ketamine and delirium
• Low-dose ketamine was associated with a LOWER risk of postoperative delirium.
• High doses did not influence the risk.
#anaesthesia#ketamine#FreeForAWeek#MedTwitter#pain
https://t.co/PX1wvkEy4s
Let's talk intraop ketamine and postop delirium
• At low doses (≤ 0.35 mg/kg), there was a lower incidence of postop delirium compared with patients who had not received ketamine.
• No association was observed at higher doses (> 0.35 mg/kg).
#anaesthesia #MedTwitter
https://t.co/W36VSm6HEj
Does the use of intraoperative ketamine affect the incidence of postoperative delirium?
Does the dose matter?
Compared with patients not receiving ketamine, a low dose (≤ 0.35 mg.kg-1) was associated with lower risks of postoperative delirium.
#anaesthesia#pain#MedTwitter
https://t.co/W36VSm6HEj
"A study from Beth Israel Deaconess Medical Center confirmed and quantified the belief of many anesthesiologists that low doses of intraoperative ketamine are associated with lower odds of postoperative delirium compared with high doses. The investigation also defined an optimal dosing range to help prevent postoperative delirium in surgical patients.
“Two factors that can lead to delirium are pain and neuroinflammation, and ketamine might be able to address this by providing analgesia with an anti-inflammatory effect,” said Lars Kaiser, a medical student at the institution. “On the other hand, ketamine—especially in high doses—can lead to nightmares and hallucinations, which in turn could lead to an increased risk of delirium. As such, we hypothesized that there is a dose-dependent association between ketamine and delirium.”
The researchers studied a cohort of 106,982 hospitalized adult patients who underwent noncardiac, non-neurosurgical and non-transplant procedures under general anesthesia at the institution between 2008 and 2024. Next, they assessed the association between intraoperative ketamine administration (dosed as mg/kg of body weight) and postoperative delirium within seven days. Cases of delirium were as identified from nursing and physician discharge notes paired with manual chart review, Confusion Assessment Method assessments, and ICD-9 and ICD-10 codes.
Presenting the findings at the 2024 annual meeting of the American Society of Anesthesiologists (abstract A1207), Kaiser reported that 2,837 patients developed postoperative delirium within seven days of surgery, of whom 297 were given intraoperative ketamine. The median intraoperative ketamine dose was 0.35 mg/kg (IQR, 0.25-0.52 mg/kg).
https://t.co/3CyrpY7DPa
A semi-supervised large-language model approach can save hours of expert labeling work when identifying delirium based on nursing and physician notes: our Dr. Stephen Woloszynek presenting his work at the Anesthesiology Journal Symposium on AI #ANES24@BIDMCAnesthesia@sw424
Lisa-Marie Wichelhaus discusses different PEEP titration techniques during general anesthesia: is the decremental PEEP trial a good gold standard? #ANES24@freezy3173@BIDMCAnesthesia
Low doses of ketamine may prevent postoperative delirium while high doses carry risks: our Lars Kaiser presents at the Best Abstract Session at the #ANES24@lars_kaiser_@BIDMCAnesthesia
What time of day is best to undergo anesthesia? asks Dr. Theresa Tenge and shows higher rates of intraoperative complications at mid-day and late work hours!
#ANES24@t_tenge@BIDMCAnesthesia
Dexmedetomidine might increase postoperative delirium in patients at high risk of hemodynamic instability - Elena Ahrens presents at the #ANES24 annual meeting.
@ElenaAhrens00
@BIDMCAnesthesia
NEW from our lab - Respiratory mechanics in patients undergoing surgery with prior COVID infection - exciting insights first authored by @AimanSuleiman90@BIDMCAnesthesia
Previous Coronavirus Disease-2019 Infection and Lung... : Anesthesia & Analgesia https://t.co/WjS661lHBU
7 Posters, 2 Oral presentations, 1x #iars24 best abstract finalist, 1x #socca24 young investigator award and lots of gettogethers conclude a very succesful meeting for the Perioperative Outcomes Lab! @BIDMCAnesthesia