NT-proBNP
🧠 Core physiology
NT-proBNP is released from LV myocardium due to:
• Increased wall stress from volume or pressure overload
• Hypoxia and ischemia
• Neurohormonal activation like Angiotensin II and Endothelin
👉 It reflects hemodynamic stress, not just heart failure
⚙️ Biochemical pathway
Pre-proBNP (134 AA) → proBNP (108 AA) → cleaved into:
• BNP (32 AA) → biologically active, causes natriuresis and vasodilation
• NT-proBNP (76 AA) → inactive but clinically measurable
👉 NT-proBNP is more useful because of stability
⏱️ Kinetics and clearance
• BNP half-life ~20 minutes
• NT-proBNP half-life 90–120 minutes
• BNP cleared by receptors and enzymes
• NT-proBNP cleared exclusively by kidneys
👉 NT-proBNP reflects sustained cardiac stress over ~12 hours
📊 BNP vs NT-proBNP clinical relevance
• BNP affected by neprilysin inhibition
• NT-proBNP unaffected
• BNP less stable in vitro
• NT-proBNP highly stable
👉 In modern practice, NT-proBNP is preferred
🚨 Acute dyspnea: Rule OUT HF
NT-proBNP < 300 pg/mL
• Negative predictive value ~99%
• Effectively excludes acute decompensated HF
👉 Shift focus to pulmonary or systemic causes
2: Rule IN HF using age-adjusted cutoffs
“45-90-18 rule”
• Age <50 → >450 pg/mL
• Age 50–75 → >900 pg/mL
• Age >75 → >1800 pg/mL
👉 Aging myocardium and declining GFR increase baseline levels
🏥 Chronic outpatient setting
NT-proBNP < 125 pg/mL
• Rules out chronic HF in stable patients with mild symptoms
⚠️ Critical concept
NT-proBNP is NOT HF specific
👉 It is a marker of myocardial strain
👉 Always interpret with clinical context, echo, volume status
🚩 Causes of falsely elevated NT-proBNP
Think CARSS
• CKD → reduced renal clearance
• Age → baseline elevation
• Rhythm → AF and tachyarrhythmias
• Sepsis → cytokine-mediated myocardial depression
• Strain → RV strain like PE, PAH
Also seen in:
• Acute coronary syndrome
• Critical illness
👉 Elevated value ≠ always LV failure
📉 Causes of falsely low NT-proBNP
• Obesity → increased peptide clearance
• Flash pulmonary edema → delay in release 2–4 hours
• HFpEF → less wall stretch compared to dilated ventricles
• Constrictive pericarditis or tamponade → restricted stretch
• Severe mitral stenosis → LV underfilled
👉 Normal value does not completely exclude HF
💡 High-yield bedside pearl
Obesity halving rule
• Reduce diagnostic cutoffs by ~50%
• Example: 450 becomes ~225
👉 Prevents missing HF in obese patients
💊 ARNI paradigm shift
Sacubitril inhibits neprilysin
→ BNP breakdown blocked → falsely elevated BNP
👉 BNP becomes unreliable
✅ NT-proBNP must be used for diagnosis and monitoring
💊 Sacubitril/Valsartan dosing
• Starting dose: 24/26 mg or 49/51 mg PO BD
• Target dose: 97/103 mg PO BD
⚠️ Absolute rule
• 36-hour washout after ACE inhibitor
Monitoring
• Hypotension most common
• Hyperkalemia risk
• Creatinine rise up to 30% acceptable
📉 Prognostic and discharge utility
Track admission to discharge change
👉 Target ≥30% reduction
If not achieved
• Persistent subclinical congestion
• High 30-day readmission and mortality
👉 Action
• Continue IV diuresis
• Plan early follow-up within 72 hours
👉 Always correlate with clinical exam, echo, IVC, response to diuretics
🔚 Final takeaways
• <300 pg/mL rules OUT acute HF
• Always apply age-adjusted rule-IN
• Interpret in clinical context, not isolation
• Use NT-proBNP in ARNI patients
• Aim ≥30% reduction before discharge
This is not just a lab value.
It is a dynamic tool for diagnosis, monitoring, and prognosis
❤️ Like + Repost
👉 Follow @DrNikhilMD for more
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
Digoxin in Rheumatic Heart Disease (DIG-RHD)
RCT evaluating digoxin in patients with HF with rheumatic heart disease
❤️ A long-standing therapy now undergoing rigorous evaluation in a contemporary population needed
Key results
💊4% relative risk ⤵️ of primary endpoint driven in those tx with digoxin by ⤵️ worsening HF
💊 Hospitalization for HF was very infrequent (2.8 vs. a mortality rate of 4.9 per 100 patient-years)
💊 1st trial evidence for digoxin as a safe treatment for reducing HF worsening in RHD
#ACC26 #GlobalCardiology #ValvularHeartDisease #LBCT #rheumaticheart
SPIRIT-HF
Mineralocorticoid receptor antagonists are foundational in HF—but gaps remain.
This trial evaluates spironolactone in #HFpEF & #HFmEF
➡️ Key results:
♥️unable to demonstrate a benefit of spironolactone in HFpEF or HFmEF compared with placebo
♥️50% discontinuation of Spiro due to side effects
♥️Underpowered trial
#ACC26 #HeartFailure #MRA #LBCT
🫀Heart failure in 2026: we are no longer treating symptoms. We are redesigning the disease.
The latest evidence update reminds us of something profound:
Heart failure is no longer a single entity.
It is a spectrum, and now, finally, we are treating it as one.
Several paradigm shifts stand out.
1. SGLT2 inhibitors are no longer “add-on” therapy.
They are foundational across the entire EF spectrum.
From HFrEF to HFpEF, the data are now consistent.
Not just symptom improvement, but hard outcomes.
This may be the most important unifying therapy in modern HF.
2. HFpEF is no longer a therapeutic desert.
For the first time, we have real disease-modifying options:
Finerenone → outcome reduction across EF ranges
GLP-1 / dual incretin therapies → targeting the obesity phenotype
Structural and metabolic mechanisms are finally being addressed
We are moving from “HFpEF frustration” → HFpEF phenotyping.
3. Acute heart failure is no longer about stabilization.
It is about early transformation.
The new paradigm:
Start GDMT in-hospital
Optimize rapidly
Treat beyond congestion
Decongestion is still important, but it is no longer the goal.
Disease modification starts on day 1.
4. Decongestion is becoming precision medicine
Urine sodium-guided therapy
Early escalation of loop diuretics
Sequential nephron blockade
Not just “give furosemide”, but measure, adjust, and target response.
5. Devices are no longer rescue therapy, they are integrated care
TEER expanding from mitral → tricuspid
Pulmonary artery pressure monitoring reducing hospitalizations
Remote hemodynamics shaping outpatient management
The boundary between ICU, ward, and home is dissolving.
6. The biggest problem is no longer evidence.
It is implementation.
We already have:
Quadruple therapy
Proven outcome benefits
Yet many patients never reach target doses.
The gap is no longer science.
It is execution.
🤓Final message
Heart failure care has entered a new era:
Mechanism-based therapy
Early aggressive optimization
Phenotype-driven treatment
And perhaps most importantly:
We are no longer chasing symptoms.
We are altering the trajectory of the disease.
📃Reference
Liori S, et al. Heart failure evidence update 2026. Heart Failure Reviews. 2026. https://t.co/T4MVjK0vGd
☝️It’s time to stop overcomplicating this.
👉LDL-C < 55 mg/dL.
For anyone with:
∙✅ Prior MACE (MI, stroke, revascularization)
∙✅ Type 2 diabetes
∙✅ High or very high cardiovascular risk — by any validated score
∙✅ Significant subclinical atherosclerosis on imaging
👉And < 40 mg/dL for:
∙✅ Polyvascular disease
∙✅ Recurrent events despite optimal therapy
📍We have the tools:
💊Statins. Ezetimibe. Bempedoic acid.
💉PCSK9 inhibitors. Inclisiran.
📍We have the evidence.
📍We have the targets.
👉Less than 25% of ASCVD patients reach LDL-C < 55 mg/dL in real life.
💊💉That’s not a pharmacology problem. That’s a mindset problem.
📍Simplify the decision. Intensify the therapy. Protect the patient.
📍One threshold. All high-risk patients. No excuses.
🫀 SPORTS CARDIOLOGY: what every cardiologist should know
New review just out 👉
Exercise is medicine… but not always harmless.
⚠️ Key message:
Sudden cardiac death (SCD) in athletes is rare (~1:50,000) but often the first manifestation of underlying disease
🔍 What really matters in practice?
1. Screening works (but not perfectly)
✔️ ECG-based screening can reduce SCD by up to 90%
❗ Still misses ~20% of conditions (e.g. coronary disease, fibrosis)
2. Athlete’s heart ≠ cardiomyopathy
The biggest challenge is NOT finding disease…
👉 it’s not overcalling disease
Physiological adaptations can mimic:
HCM
DCM
ARVC
LV non-compaction
➡️ Requires multimodality approach (ECG + imaging + exercise + genetics)
3. Red flags you should never ignore 🚩
Exertional syncope
Chest pain
Family history of SCD
Abnormal ECG (TWI lateral, ST depression, Q waves)
4. CMR is your best friend
👉 Especially when ECG is abnormal
👉 Detects fibrosis and subtle cardiomyopathy
(Yes… this aligns perfectly with what we see in ACM/arrhythmogenic phenotypes 👀)
5. Exercise prescription is evolving
❌ Old approach: “stop sport”
✅ New approach: shared decision-making
Some key points:
ARVC / desmosomal variants → avoid high-intensity exercise
Low-risk HCM/DCM → may still participate
Myocarditis → no sport for ≥3 months
6. The new frontier: master athletes 🏃♂️
↑ atrial fibrillation (3–5x)
↑ coronary calcium
↑ myocardial fibrosis
👉 Long-term effects still unclear
🧠 Take-home message
Sports cardiology is not about restricting athletes.
It’s about:
✔️ Identifying risk
✔️ Avoiding misdiagnosis
✔️ Enabling safe exercise
💡 My reflection:
This is exactly where imaging + genetics + phenotype integration becomes critical — especially in early/arrhythmogenic cardiomyopathies.
https://t.co/bQFlrEKZnS
As an interventional cardiologist, I won’t do coronary angiogram in an asymptomatic patient with elevated CAC. To me high CAC score means intensification of the GDMT for CAD.
#cardiox@rblument1@MichaelJBlaha@khurramn1
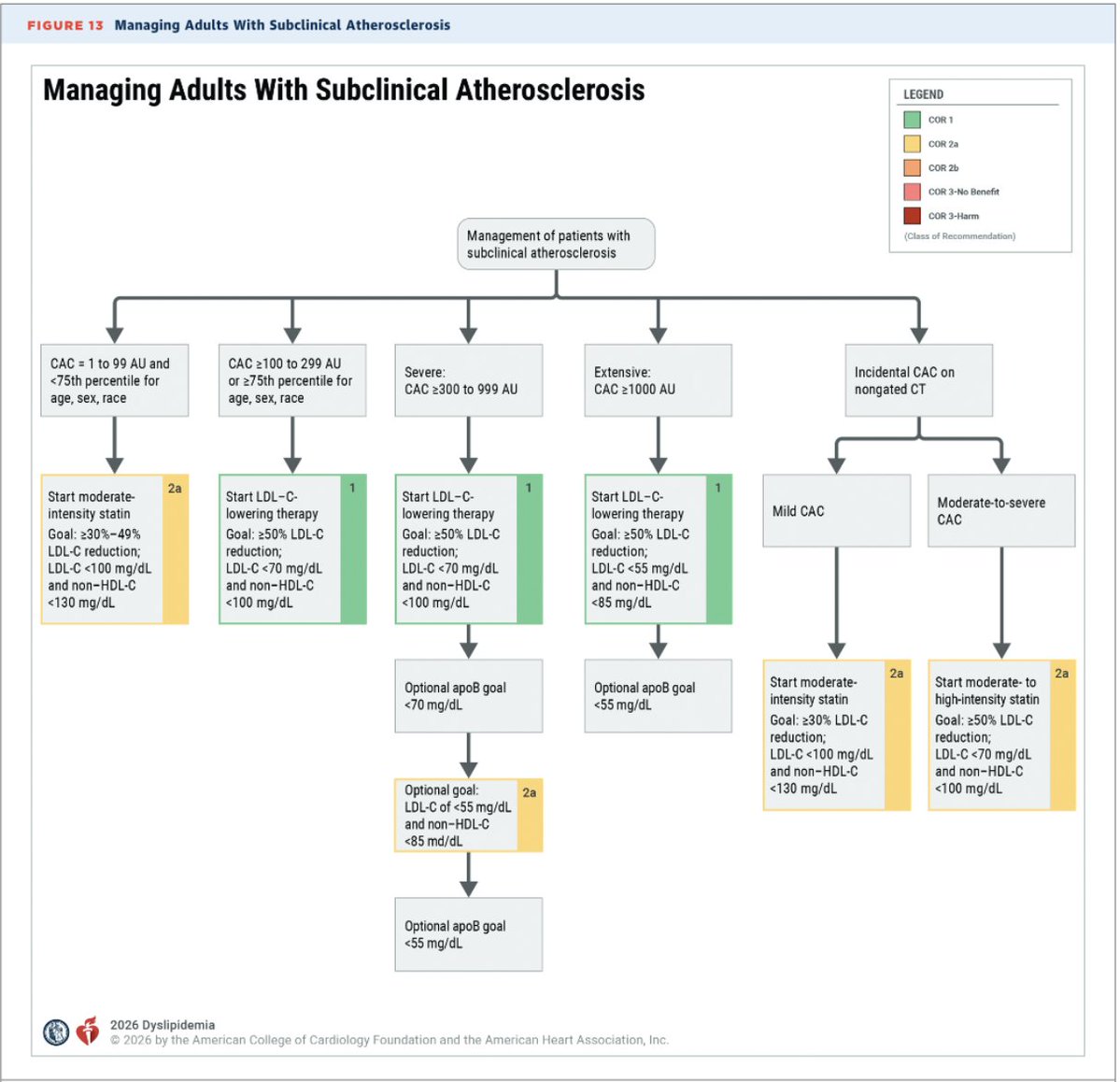
🚨 The 2026 ACC/AHA Dyslipidemia Guidelines are here, and CAC scoring just got a Class 1 recommendation for guiding statin therapy decisions in intermediate-risk patients.
Key updates:
➡️ CAC = 0 may allow withholding statins
➡️ CAC ≥100 AU or ≥75th percentile → statin therapy recommended
➡️ CAC ≥1,000 AU → intensive LDL-C targets
➡️ PREVENT-ASCVD equations now guide primary prevention
➡️ Lp(a) testing at least once in a lifetime
Big shift in how we risk-stratify and treat. Worth reading the full guideline. 👇
🎥 Seorang kiper di liga amatir Istanbul, Turki tidak sengaja menendang bola mengenai seekor burung. 🤕
Beruntung seorang pemain langsung melakukan RJP (resusitasi jantung paru), dan berhasil menyelamatkan burung tersebut. 🫀🕊️
A long-awaited consensus statement on inflammation and heart disease
"We have thus entered an era when the evidence linking inflammation with ASCVD is no longer exploratory but is
compelling and clinically actionable."
@JACCJournals open-access
https://t.co/O828bmLpNZ
Clopidogrel versus aspirin for secondary prevention of coronary artery disease: a systematic review and individual patient data meta-analysis: @TheLancet
🥸Plavix for secondary prevention may be superior to aspirin
😱 Summary
👇👇👇