Natural history of asymptomatic moderate or severe aortic regurgitation: a systematic review and meta-analysis
Please read the article and enjoy an in-depth interview between @jhfrudd and the first author, Dr Jwan Naser from The Mayo Clinic in Rochester, Minnesota, USA
Paper: https://t.co/fxWs0bkEiv
Interview: https://t.co/ZGhyrExOAf
The next frontier for prevention of heart and vascular disease isn't targeting lipids. It's about blocking inflammation. These are some of the ongoing clinical trials @NatureMedicine
https://t.co/DSLMoPFqs7
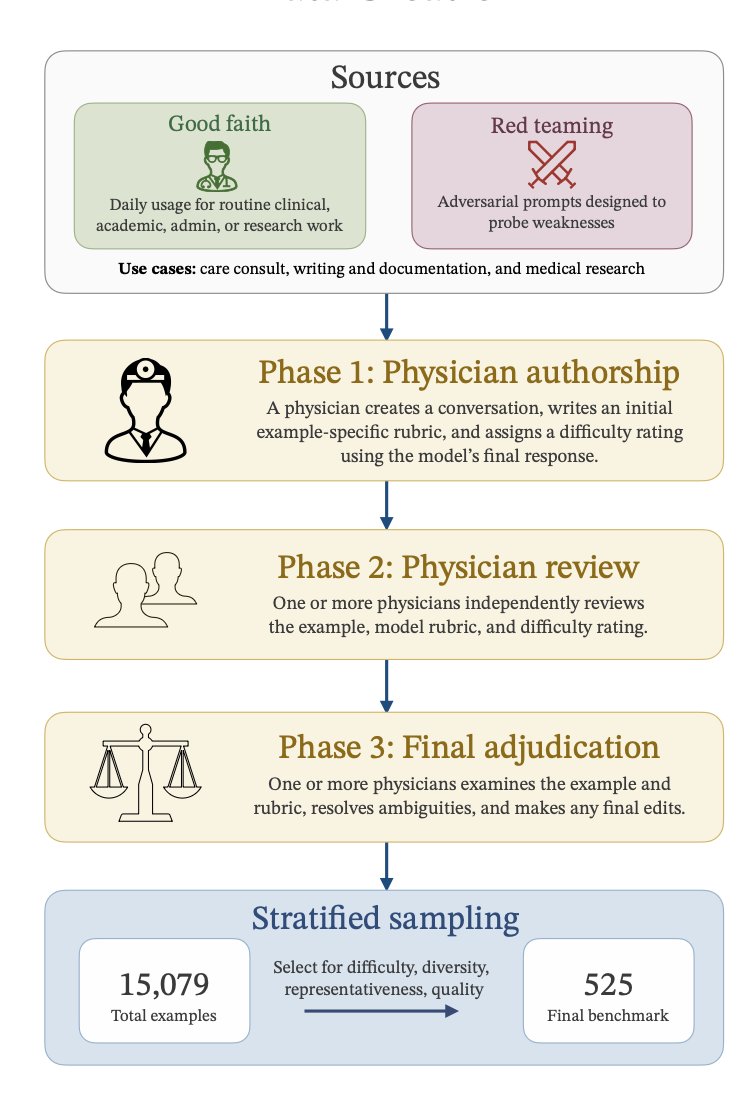
Today @OpenAI introduced ChatGPT for Clinicians, provided free for credentialed HCPs, and HealthBench Professional for benchmarking LLM medical task performance (Figure)
https://t.co/NC3R5JDGCR
https://t.co/ayJLkRtZUt
Finally, a sham-controlled CTO PCI trial—and it delivers. ORBITA-CTO: small (n=50), but rigor where it matters—blinding, placebo control, symptom-level data. CTO PCI improves angina beyond placebo, with a clear reduction in episodes and more angina-free days. Not prognosis, not hard endpoints, but real symptom benefit—properly measured. #acc26
https://t.co/UgoJVoX87H
Complete revascularization timing in ST-segment elevation myocardial infarction and multivessel disease with heart failure: the OPTION–STEMI trial https://t.co/bxuq8hjWeN
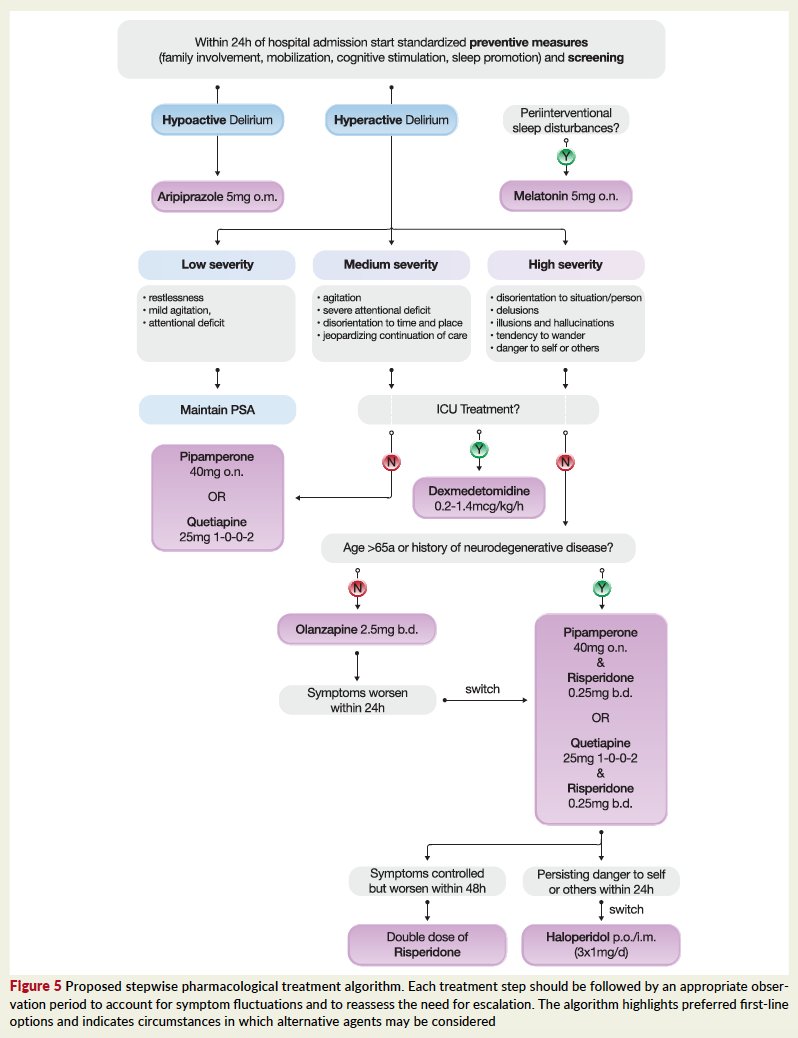
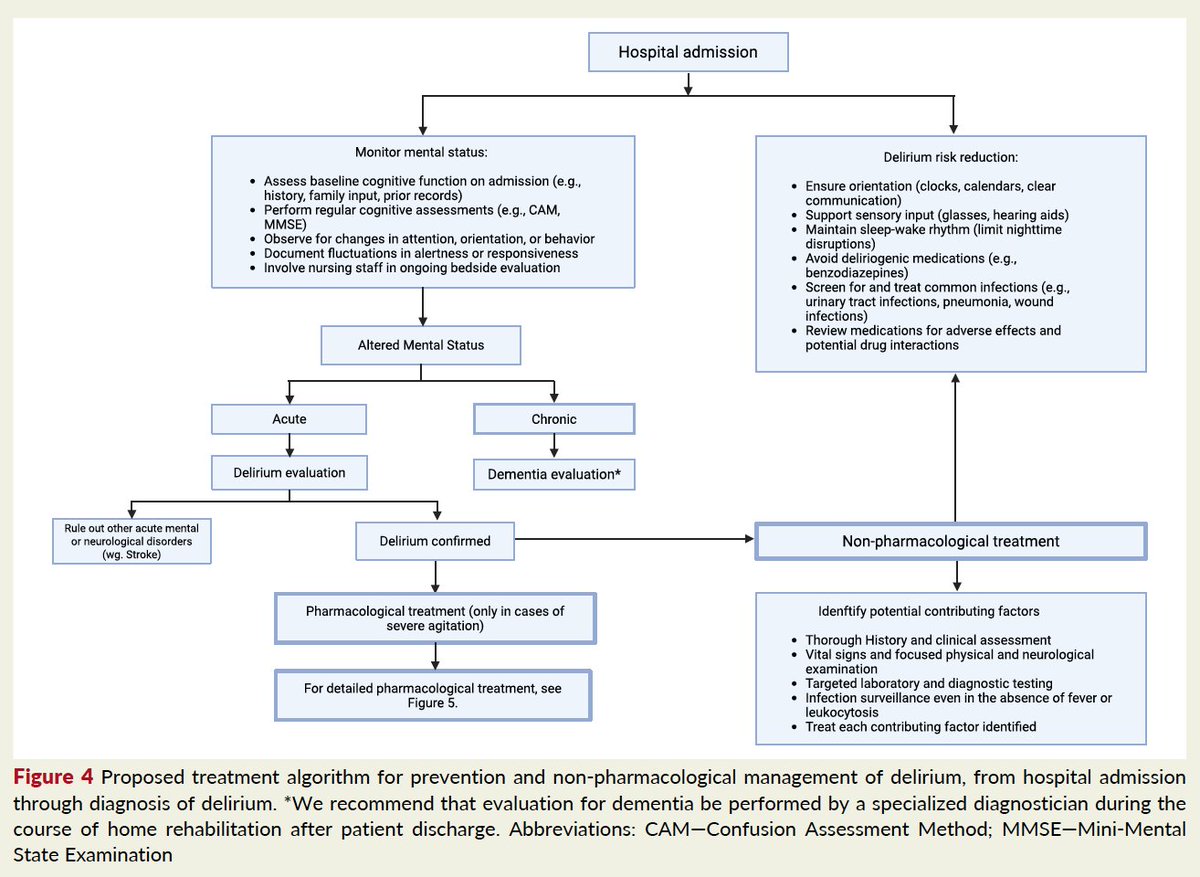
#Delirium is not “just confusion”, it is a major prognostic event in CV medicine.
In our State-of-the-Art Review in #EHJ, we synthesize current evidence on mechanisms, prevention, and management across the CV continuum. 🧠🫀
https://t.co/l4VSzuTQDL
@CekajEndrit et al👏👏
Clopidogrel outperformed aspirin in preventing cardiovascular events in patients with coronary artery disease (CAD), showing superior efficacy across both genders, in PANTHER-2 trial. https://t.co/XqH9rADKHp
🧵 1/ First ever AHA/ACC/multi-society guidelines re: diagnosis & management of acute PE released today!
2 year effort with 38 authors from 10 specialties.
Link attached & summary in this thread:
https://t.co/uUUyUvz3pR
The SCAPIS study published in JAMA
~25,000 🇸🇪 participants, ~8 years follow-up. Adding coronary CT angiography #CCTA plaque information improved event prediction beyond clinical risk and calcium score.
This is the first study showing the added value of CCTA on top of the calcium score for risk prediction.
🎯 What to look for: lipidic soft (non-calcified) plaque.
👀 Practical takeaway: Consider a CT angiography for risk stratification on top of the calcium score.
Link: https://t.co/EOK6DH6PF6
🎥 Posting my avatar summarizing the study.
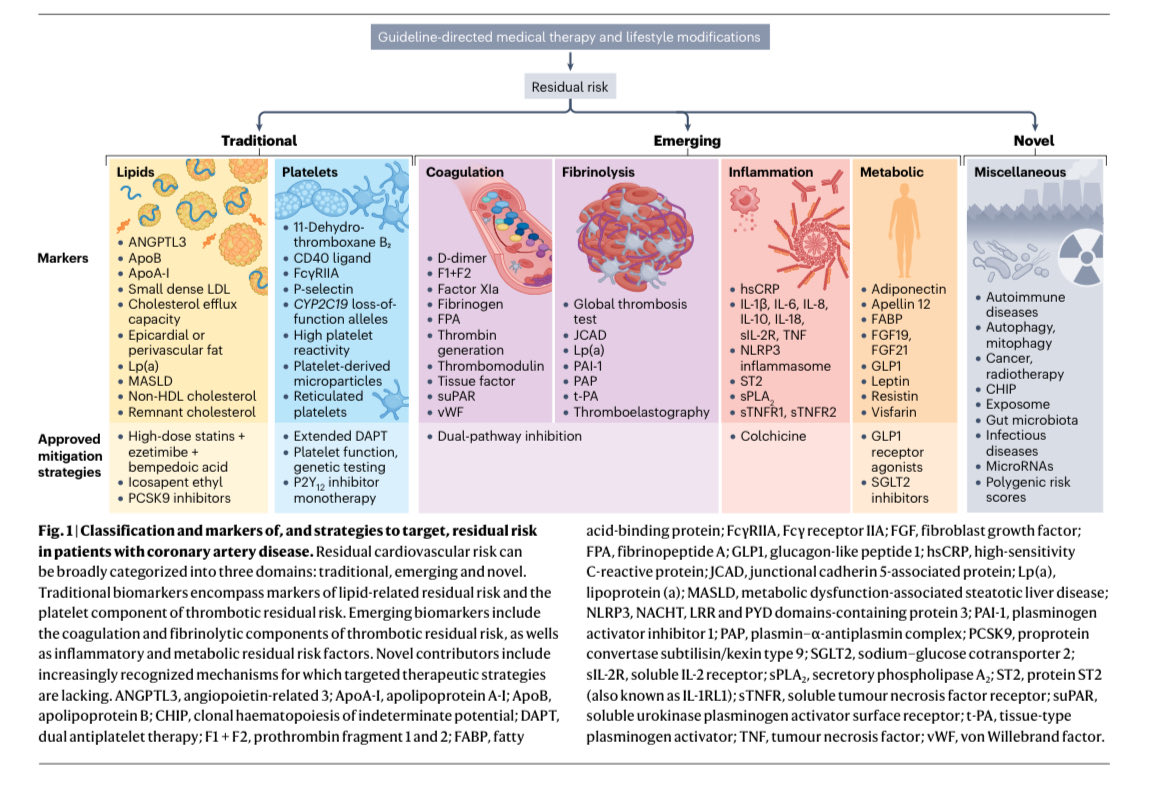
With 561 references, this article—published in Nature Reviews Cardiology—is among the most comprehensive reviews of the pathophysiology, biomarkers, and therapeutic strategies addressing residual risk in coronary artery disease.
Read more at https://t.co/JeH9YWzyLl
Complete revascularization timing in ST-segment elevation myocardial infarction and multivessel disease with heart failure. Read the results of the OPTION–STEMI trial in #EHJ 👉 https://t.co/EEFrKSbySC
@RoccoMontone@ehj_ed#heartfailure
STEMI and cardiogenic shock. A time course analysis of the use of microaxial flow pump (mAFP) and clinical outcomes from the DanGer Shock trial @CardResearchOUH@cardiac_group@RigsHeart https://t.co/Ho8pfamkBm
The risk of high lipoprotein A [Lp(a)] in nearly 28,000 healthy women followed for 30 years. Fortunately, after waiting for decades, we will have drugs vs Lp(a) soon to reduce this risk
https://t.co/SfXTtpaV0i
Plaque rupture with thrombosis drives ACS, and thin-cap fibroatheroma is the archetypal high-risk plaque. There are consistent features of vulnerability across imaging modalities (large plaque burden, small MLA, TCFA, high LCBI, positive remodelling, etc.), with risk increasing when multiple features coexist. Yet absolute event rates remain low, consistent with pathology data showing most plaque ruptures are clinically silent.
So should we prophylactically stent high-risk plaques? According to this Viewpoint, completed trials (PROSPECT ABSORB, PREVENT) suggest no durable reduction in death or MI versus optimal medical therapy—benefits are limited to fewer revascularisations, at the cost of many unnecessary PCIs. With modern medical therapy, a wait-and-see strategy appears safe, avoiding most interventions without adverse consequences. For now, data favor surveillance and aggressive medical therapy over preventive PCI.
READ THE VIEWPOINT: https://t.co/D9nem3KNpd
























![EricTopol's tweet photo. The risk of high lipoprotein A [Lp(a)] in nearly 28,000 healthy women followed for 30 years. Fortunately, after waiting for decades, we will have drugs vs Lp(a) soon to reduce this risk
https://t.co/SfXTtpaV0i https://t.co/PdykVP6nKB](https://pbs.twimg.com/media/G-ErPkyagAEfWg9.jpg)































