Happy to share the news that our E-cadherin article received enough views to be a Top Viewed Article in Histopathology.
Read it here https://t.co/r02lExjV9J #TopViewedArticle@wileyinresearch@RezaTaha_
NOT a germinal center.
Beware high-grade invasive carcinoma with the (no longer recognized) medullary pattern. Lymphoepithelioma-like carcinoma is another somewhat quaint term used on occasion.
#breastpath
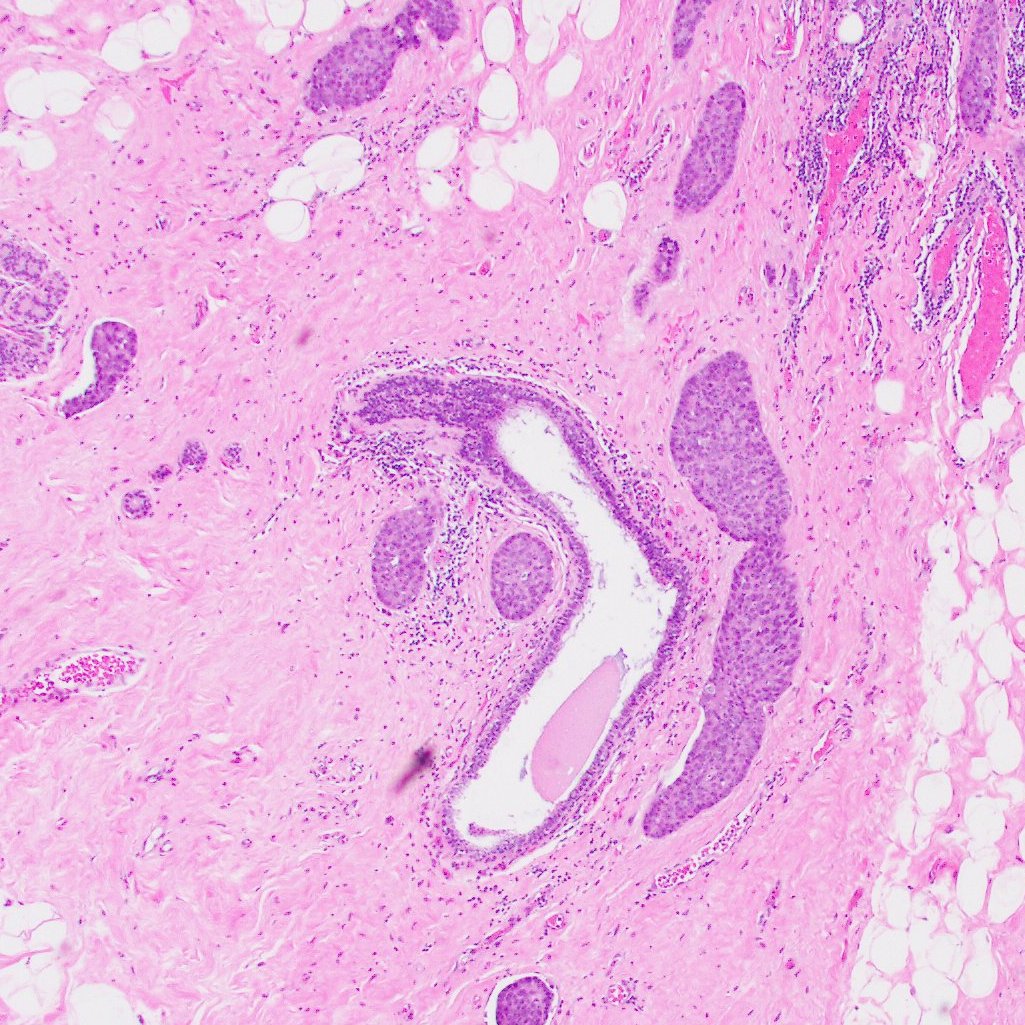
When large nests of tumor surround a completely normal duct, they are much more likely to be invasive cancer or lymphovascular invasion than DCIS. A useful pattern to remember on a biopsy
#breastpath
Sorry for the long silence. This is a quick in-house case I had to share.
Breast mass, 2 cm. High grade, central fibrosis, lymphoid infiltrate, ER/PR/HER2 negative. Classic TNBC. Correct?
Incorrect. History of melanoma, discovered by chance, not mentioned anywhere in the pathology requisition, casually buried in a random note.
How scared should we be? How often should we work-up triple-negative tumors in search of some odd metastatic lesion? How many of you would have worried about this and investigated it further in the absence of history? I certainly wouldn't have.
Good luck staying safe and cautious without spiraling down into the abyss of obsession and paranoia.
IHC: Melan-A
#melanoma #breastcancer #breastpath @washupathedu@washu_pathology
In my training, I heard two different thought processes regarding how to approach signing out cases. I would like to hear from experienced pathologists which one they follow: Do you prefer knowing the pt’s hx before looking at the slide, or no hx?#PathX#PathTwitter#Pathology