Pediatric radiologist ❤️ultrasound, CTA, neonatal imaging, emergency imaging, emergency neuroradiology, CHD, ped GU and Gyn imaging. Opinions are my own
EASY ONE 🔥🔥
Young adult with severe headache, fever, periorbital swelling, proptosis and cranial nerve palsies (III, IV, VI).
Contrast-enhanced CT BRAIN done.
What is the diagnosis?
#MedX
FINAL ANSWER ;
Ivy Sign in Moyamoya Disease
Diffuse leptomeningeal hyperintensity along the sulci on FLAIR (slow-flow pial collaterals) with corresponding enhancement on post-contrast images.
Classic in children with recurrent TIAs.
NEURO CASE 🔥🔥NEURO ENTHUSIASTS🔥🔥
Child with recurrent transient ischemic attacks and headaches.
MRI Brain (FLAIR axial + post-contrast T1).
What is the name of this classic sign?
What is the diagnosis?
Beautiful illustration of the findings in a patient with congestive cardiac failure .
Findings
1. Cardiomegaly
2. Cephalization or upper lobe diversion
3. Fluid in fissures ( labeled here as effusion)
4. Kerley lines
Enjoy !
1/Do radiologists sound like they are speaking a different language when they talk about MRI?
T1 shortening what? T2 prolongation who?
Here’s a translation w/an introductory thread to MRI.
ADULT EMERGENCY CASE 🔥
A 35-year-old with severe sore throat, high fever, drooling, trismus, neck pain and swelling for 4 days. Difficulty swallowing and voice change.
Contrast-enhanced CT neck done.
Red arrows highlights the lesion.
What is the diagnosis?
Which space is involved?
Why is this a potential airway emergency?
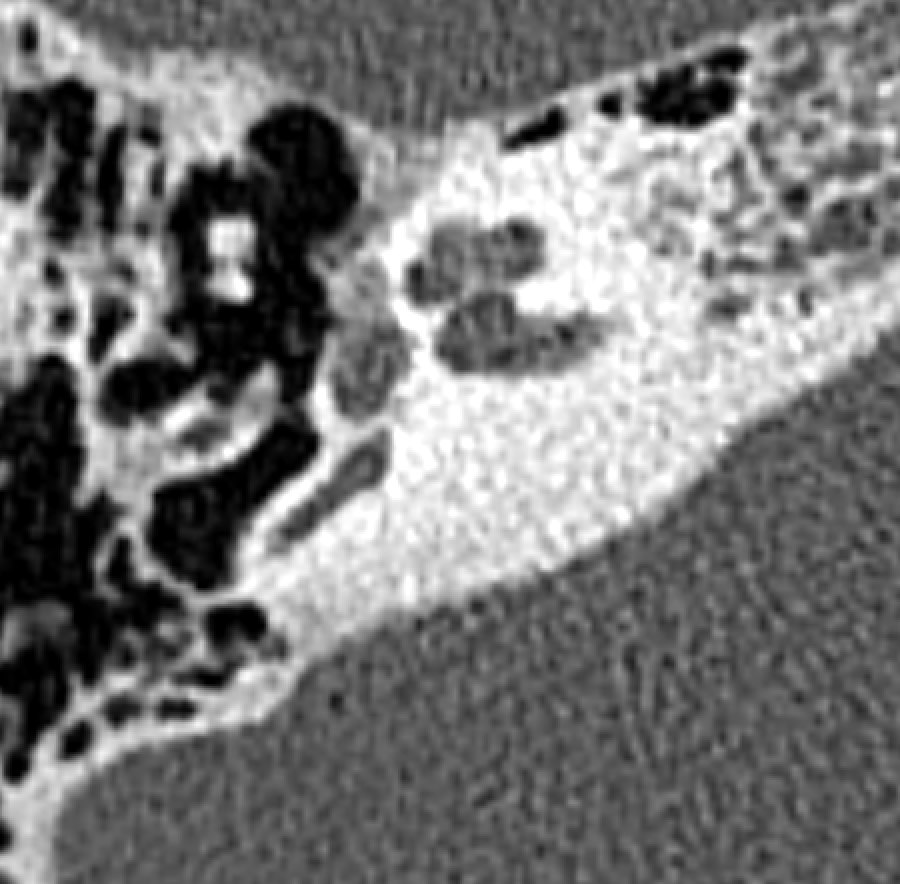
Fenestral otospongiosis! Most common cause of progressive conductive hearing loss in young adults. Female predominance (2:1), peaks at 20 – 40, often bilateral and familial. Look for the classic focal lucency at the fissula ante fenestram (just anterior to the oval window).
The patient developed cerebral air embolism following CPR.
During cardiopulmonary resuscitation, especially with:
vigorous chest compressions
positive-pressure ventilation
possible lung injury or barotrauma
Air can enter the vascular system (e.g., via damaged alveoli or veins) and travel to the brain.
This week's SPIN POV: Lysosomal disorders - GM1 gangliosidosis, Krabbe's, and Neuronal ceroid lipofuscinosis must be considered when encountering T2 dark thalami and white matter signal change in a child with neuroregression.
This one's for me!!
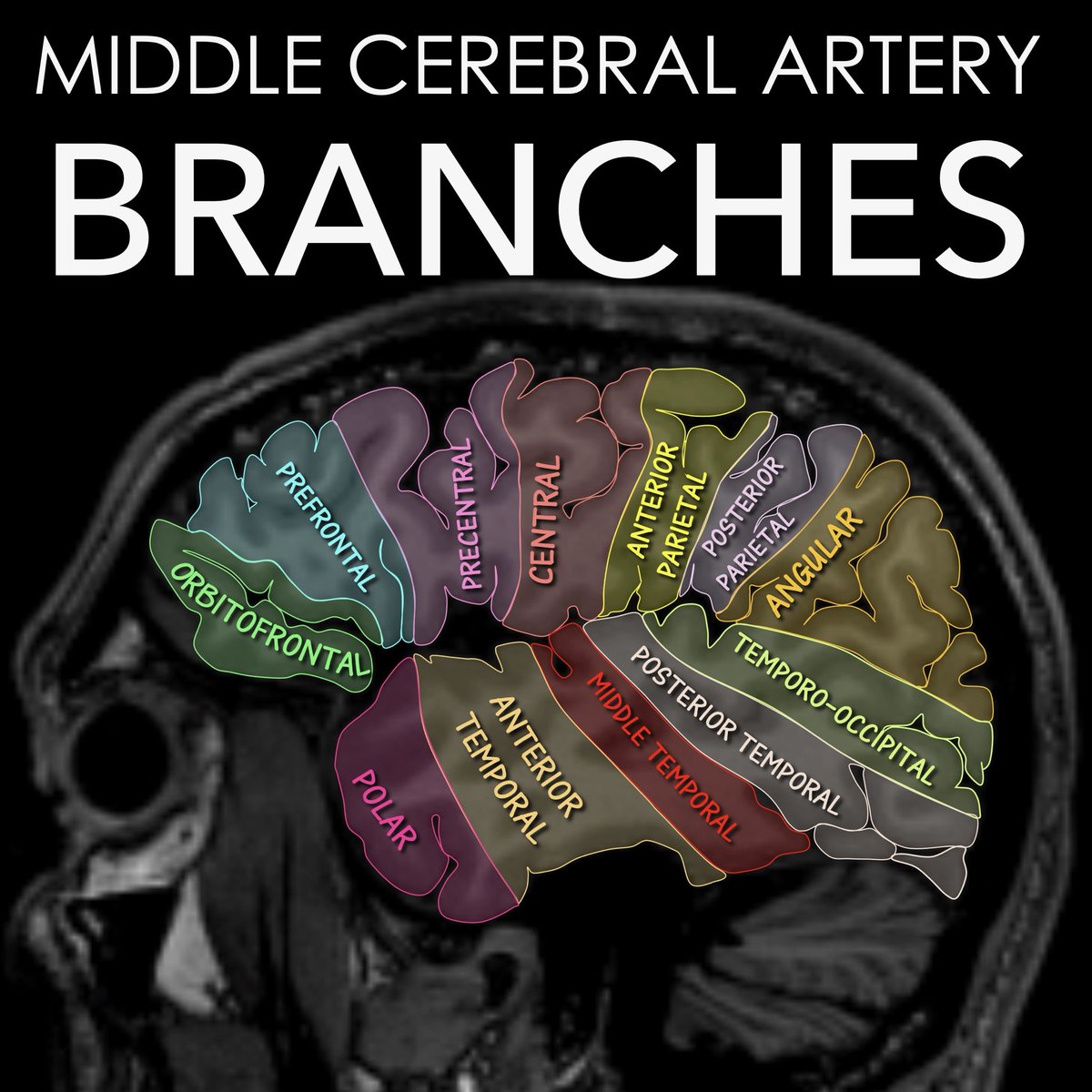
I was tired of seeing small MCA infarcts that were clearly from a branch occlusion& not knowing the name of the branch that was occluded!
I decided I would find a way to remember these territories myself-and then share it w/ you!!
Here's how you can remember the different territories
Start w/4 cardinal territories
-These are the skeleton from which you can remember the rest
Orbitofrontal: Easy, it overlies orbit in the frontal region, like its name
Central: East, it's the territory surrounding central sulcus
Angular: Easy, it literally looks like an angle between parietal & temporal region
Polar: Easy, it's the temporal pole!
Bc it's the MCA, there is an M or two humps between each of these cardinal branch territories & their names reflect the anatomy
Finally, the temporal territories look like fingers on a hand:
Polar is the thumb of the hand: remember polar sounds pollex which means thumb
Middle temporal is literally the middle finger!!
Now you know the middle cerebral branch territories— so your reports will never be middling!