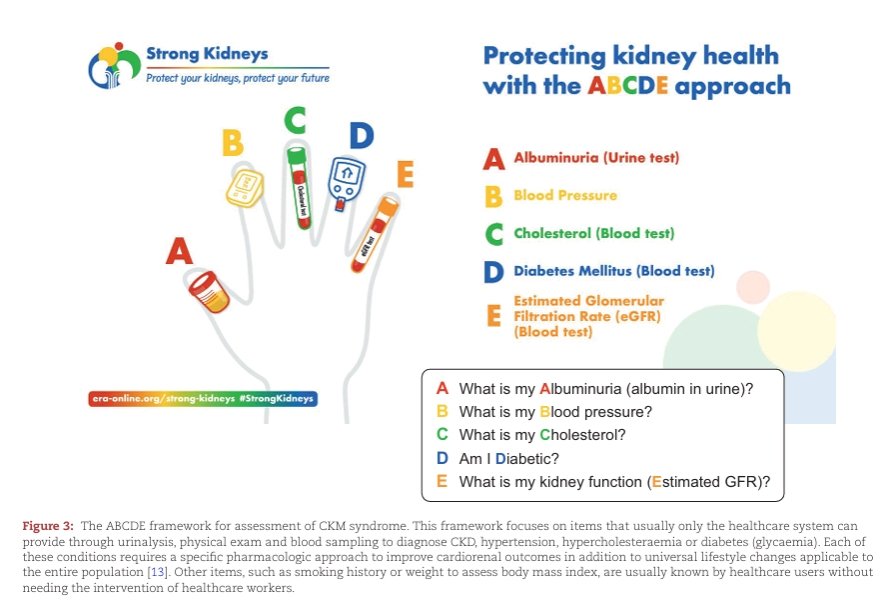
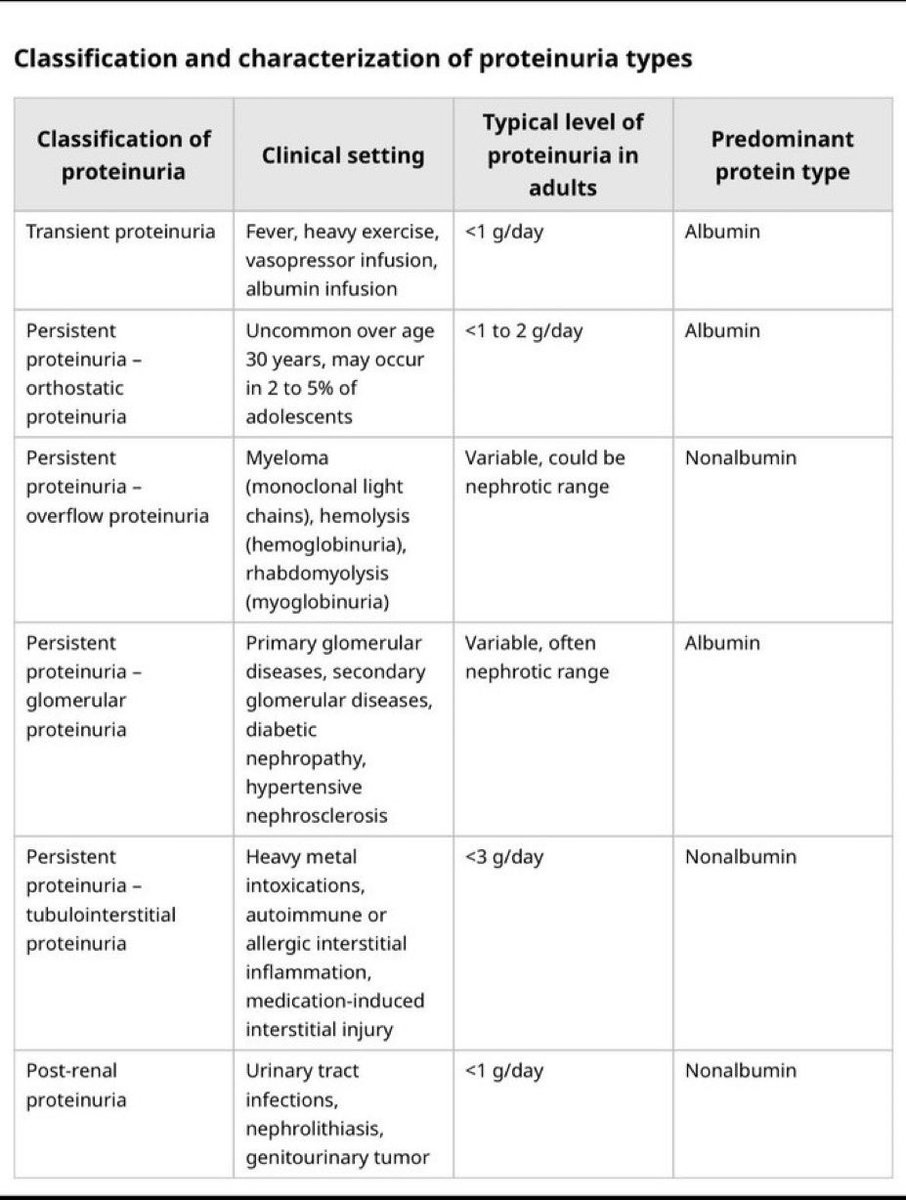
🚨 LA ENFERMEDAD RENAL CRÓNICA (ERC) ya no debe diagnosticarse tarde. Un artículo reciente en Nephrology Dialysis Transplantation 2026 propone cambiar el paradigma: pasar de “tratar diálisis” a “PREVENIR ERC” 🩺🧠. El mensaje es contundente: una creatinina normal NO descarta daño renal ❌🧪, porque muchos pacientes ya tienen albuminuria elevada con TFG conservada 📉. La clave está en el enfoque ABCDE 🔍: A️⃣ Albuminuria, B️⃣ Presión arterial, C️⃣ Colesterol, D️⃣ Diabetes y E️⃣ eGFR. El gran problema actual es que la albuminuria sigue infrautilizada 📋, pese a que detectarla temprano permite iniciar nefroprotección con iSGLT2, IECA/ARA2, finerenona y agonistas GLP-1 💊❤️🩺, logrando retrasar diálisis incluso hasta 20–30 años ⏳. Además, esta revisión introduce un concepto revolucionario: “PRE-CKD” ⚠️, pacientes aún sin ERC formal pero con alto riesgo de desarrollarla, igual que ocurre con la prediabetes. El futuro de la nefrología será prevención, detección temprana y protección cardio-reno-metabólica 🌎🫀🧬. Pedir UACR anual en pacientes con HTA, DM2, obesidad o >60 años puede cambiar vidas. #CKD #ERC #Nefrología #Albuminuria #SGLT2 #Finerenona #PrevenciónRenal #CardioRenalMetabólico #KDIGO #MedicinaInterna
📚 Nephrol Dial Transplant. 2026;41:418–427. doi:10.1093/ndt/gfaf151.
🍬🏥Estrategias de Manejo de la Diabetes en Cuidados Críticos
🔰📚Med Clin N Am 2026
https://t.co/Bti1XZqDWT
Enlace a Articulo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
Coffee & CKD ☕🩺
Current evidence suggests moderate coffee intake is probably safe in CKD — and may even offer benefits
https://t.co/gdfPRPeAyN
@NDTsocial
https://t.co/8oXHmJgyc2
Tumia link hapo juu kupata kitabu hiki kitakachokupa elimu kuhusu mtindo wa maisha magonjwa yasiyoambukiza kutoka Wizara ya Afya.
💉DKA is not a glucose problem.
It’s a metabolic collapse.
We often simplify diabetic ketoacidosis as:
❌ “Severe hyperglycemia”
But that’s misleading.
👉 You can have normal glucose and still be in DKA
1. What really defines DKA
The classic triad:
Hyperglycemia
Anion gap metabolic acidosis
Ketonemia
But the key driver is:
👉 Insulin deficiency → unchecked ketogenesis
2. The dangerous trap: Euglycemic DKA
Up to ~3% of patients present with:
Glucose <250 mg/dL
Severe acidosis
High anion gap
-Common triggers:
SGLT2 inhibitors
Pregnancy
Starvation
👉 If you wait for hyperglycemia…
👉 You will miss it.
3. Think in triggers: the “5 I’s”
Infection
Infarction
Insulin (non-adherence)
Intoxication
Infant (pregnancy)
👉 DKA is always a consequence, not the disease itself.
4. The physiology most people forget
Total body potassium = LOW
Serum potassium = often NORMAL or HIGH
Why?
👉 Acidosis shifts K⁺ out of cells
Then you give insulin →
⚠️ Potassium crashes
5. The biggest treatment mistake
Stopping insulin too early.
👉 Insulin is NOT for glucose
👉 Insulin is for ketosis ⚠️
Never stop insulin until:
Anion gap closes
Bicarbonate normalizes
6. Fluids matter more than you think
Patients are often:
👉 4–6 liters depleted
And interestingly:
Balanced crystalloids may improve outcomes⚠️
Avoid hyperchloremic acidosis
7. The mindset shift
DKA management is not:
❌ “Lower glucose”
It is:
✅ Stop ketogenesis
✅ Restore volume
✅ Correct electrolytes
✅ Treat the trigger
🤓Final message
If you remember only one thing:
👉 Normal glucose does NOT exclude DKA
📃Reference
Lowie BJ. Endocrinol Metab Clin N Am 55 (2026) 1–10 https://t.co/Vr8jKaeQJt
🫨HHS is not just “very high glucose.”
It’s a dehydration-driven neurological emergency.
We often compare it to DKA…
But the physiology is completely different.
👉 And missing that difference can be dangerous.
1. What defines HHS
Not ketones. Not acidosis.
👉 Hyperosmolarity + neurologic dysfunction
Glucose >600 mg/dL
Osmolality >320 mOsm/kg
Altered mental status
Minimal or absent ketosis
2. The key difference vs DKA
DKA → insulin deficiency → ketosis
HHS → relative insulin → NO ketosis
👉 Enough insulin to suppress lipolysis
👉 Not enough to control glucose
3. The real problem: WATER LOSS
This is what kills the patient.
👉 Volume deficit can reach up to 9 liters
Mechanism:
Hyperglycemia → osmotic diuresis
Free water loss > sodium loss
Rising osmolality → brain dysfunction
👉 It’s a spiral of dehydration → hyperglycemia → more dehydration
4. Why patients present late
HHS develops:
👉 Days to weeks
Not hours like DKA.
So patients arrive with:
Severe dehydration
Confusion / coma
Often elderly, frail, or septic
5. The biggest management mistake
Starting insulin too early.
❌ Treating it like DKA
👉 In HHS, first step is:
FLUIDS. LOTS OF FLUIDS.
1–1.5 L in first hour
Then guided resuscitation
Only after:
✅ Volume restored
✅ Electrolytes checked
→ Then insulin
6. The hidden danger
Lowering glucose too fast.
👉 Rapid drop in osmolality
👉 Water shifts into brain
⚠️ Cerebral edema
Target:
↓ glucose by 50–75 mg/dL/hour
Maintain ~250–300 mg/dL initially
7. Always search for the trigger
HHS is rarely spontaneous.
Common causes:
Infection (most common)
MI / stroke
Dehydration
Medication non-adherence
🤓Final message
If DKA is a metabolic emergency…
👉 HHS is a hemodynamic + neurological emergency
And the treatment priority reflects that.
📃Reference
Lovegrove SS, Endocrinol Metab Clin N Am 55 (2026) 11–20 https://t.co/LoW1AnyKSk