Perhaps one of the most important shifts in our understanding of Parkinson’s disease:Co-pathologies may be the rule, not the exception.
Tau, β-amyloid, TDP-43 and cerebrovascular pathology all contribute to the clinical heterogeneity of PD.
#ParkinsonsDisease#MovementDisorders
Impaired consciousness ≠ complete loss of consciousness.
Interesting discussion on why responsiveness, awareness and wakefulness should be viewed as complementary dimensions in seizure classification rather than interchangeable terms.
#Epilepsy#ILAE#Neurology
Consciousness, awareness, responsiveness, recall... Do you find these confusing? Read this recently published paper / see the table below.
https://t.co/iAMf6YHsKy
#epilepsy#seizure@FilaResearch
Don’t “BoNT-and-bye”: treat the non-motor load👌
Phenomenology in dystonia extends far beyond posture.
The non-motor syndrome deserves equal attention.
#MovementDisorders#Dystonia
Cervical dystonia has 2 big phenotypes:
-Early onset (35y) = much worse pain/mood/QoL vs later onset (48y) — motor severity differences are smaller.
-Don’t “BoNT-and-bye”: treat the non-motor load. https://t.co/TbYDNbv70S
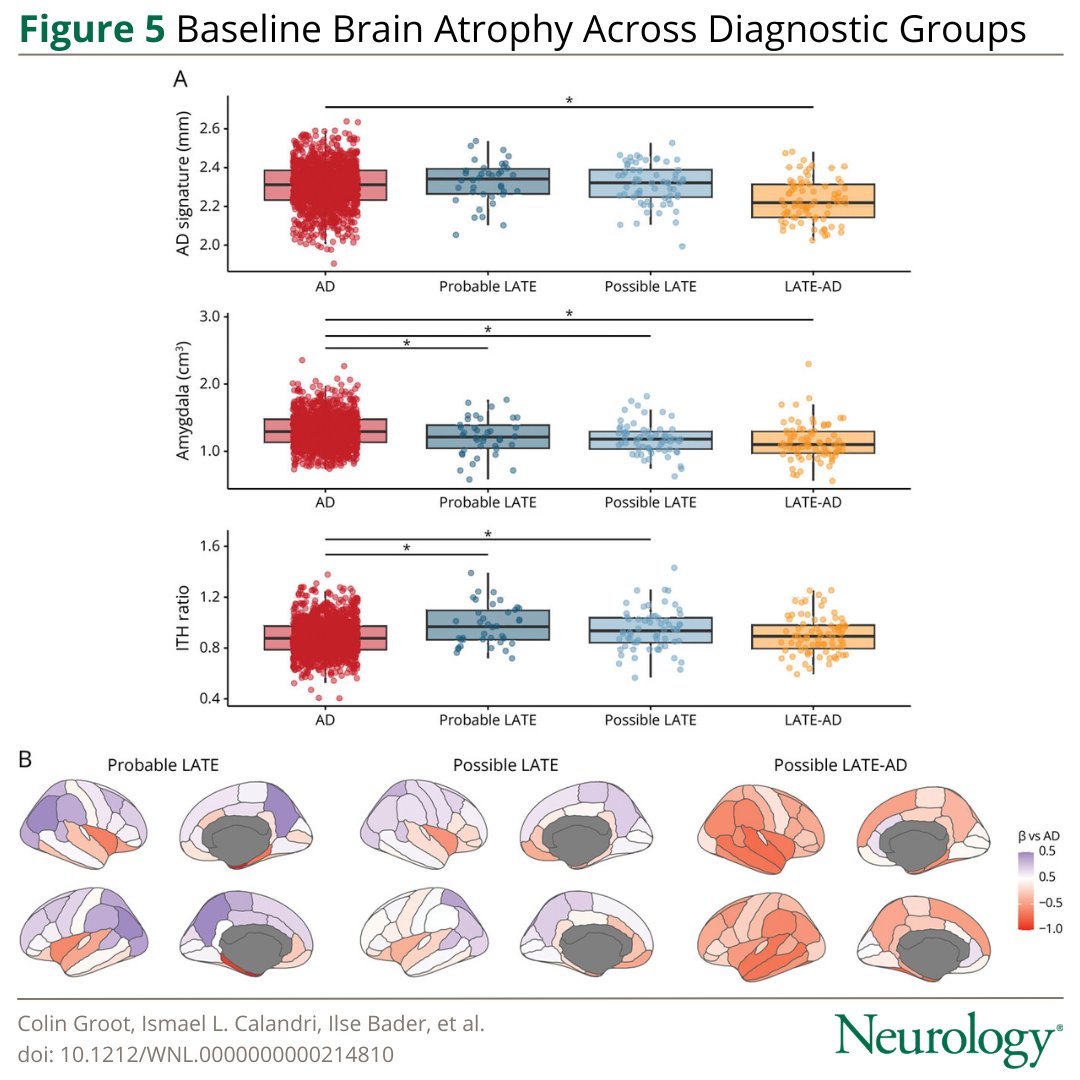
• Probable/Possible LATE showed relatively more limbic-predominant atrophy (higher ITH ratio)
• LATE-AD demonstrated greater cortical atrophy within AD-signature regions
"Not every amnestic syndrome with medial temporal atrophy is pure AD."
#Neurology#Dementia#Alzheimers
This study tested whether clinical criteria for limbic-predominant age-related TDP-43 encephalopathy (LATE) can detect a clinical profile of LATE that is distinct from Alzheimer disease in a memory clinic cohort. Read more: https://t.co/xNQSZye6wa
In adults with drug-resistant #FocalEpilepsy, cenobamate was associated with greater seizure reduction and seizure freedom vs brivaracetam, lacosamide, and perampanel, but with more adverse effects.
https://t.co/ZsIC7loxoo
Is dirty air accelerating ALS and motor neuron disease? Particulate matter refers to tiny air pollution particles that can be inhaled deep into the lungs and can enter the bloodstream, potentially triggering inflammation and injury in the brain and nervous system. Elser and Goslinga describe in a new Viewpoint in JAMA Neurology how long-term exposure to air pollution may influence the risk, progression and survival in motor neuron diseases including ALS.
Key Points:
- Higher long-term exposure to PM2.5, PM10 and nitrogen dioxide was linked to increased risk of motor neuron disease.
- Long term particulate exposure was associated w/ faster disease progression, based on functional rating scales.
- Certain pollutants were linked to a higher risk of death or a need for invasive ventilation.
My take: This study strengthens the case that environment matters in neurodegeneration. Genetics may load the gun but there is much more to the study, especially in folks w/o single monogenetic causes. Exposures and brain resilience are likely a very important part of the story. The data also push us beyond risk and into progression, which is where families are urgently looking for answers.
Here are 5 points that resonated w/ me:
1- Motor neuron disease risk is not only about genes, long term environmental exposures play a meaningful role.
2- Air pollution may not just increase risk, it may accelerate decline after diagnosis.
3- Different particle sizes and sources likely matter, and we still do not fully understand which sources are most toxic.
4- Vulnerable folks and communities may be disproportionately affected, raising environmental justice concerns.
5- Reducing air pollution could one day become a modifiable strategy to slow progression while we wait for better disease modifying therapies.
https://t.co/1tjsocSHwe @ParkinsonDotOrg@FixelInstitute@movedisorder@JAMANeuro
🚨 Patients with Normal Pressure Hydrocephalus could now possibly benefit from a new device: the eShunt, through an endovascular minimally invasive procedure by enrolling in the STRIDE trial! @TJUHNeurosurg is the only site in Pennsylvania and today we did the first case in the tri-state area @TJUHospital@NeuroatJeff@JeffersonUniv
Clinical Phenotypes of Neurosarcoidosis
🔹Neurosarcoidosis can affect virtually any part of the nervous system, leading to diverse phenotypes.
🔹Cranial neuropathies are the most common manifestation, with facial nerve palsy affecting 11–50% of patients and optic neuropathy affecting up to 25%. Optic neuropathy is most often unilateral, subacute in onset, and associated with retrobulbar pain.
🔹Central nervous system involvement is present in about 50% of reported cohorts. Potentially affected areas include brain parenchyma with multiple masses, meninges with hypertrophic pachymeningitis, and rarely vascular disease with associated strokes.
🔹Manifestations of encephalic involvement include headache, cognitive and psychiatric disorders, seizure and neuroendocrine dysfunction.
🔹Spinal cord involvement has been described in approximately 15–26% of neurosarcoidosis patients, with lower extremity weakness and paresthesias being the most common presentation.
🔹Peripheral nervous system involvement may include large and small fiber neuropathies, polyradiculoneuropathy and plexopathy:
- Large fiber neuropathy can present as mononeuritis multiplex or painful, often asymmetric, polyneuropathy.
- Polyradiculopathy may be similar in presentation to Guillain–Barre syndrome.
- Small-fiber neuropathy is common, often presenting as distal pain and paresthesias with or without associated dysautonomia.
*From: Gosselin, J., Roy-Hewitson, C., Bullis, S.S.M. et al. Neurosarcoidosis: Phenotypes, Approach to Diagnosis and Treatment. Curr Rheumatol Rep 24, 371–382 (2022).
🔗https://t.co/zzwvBwmKmO
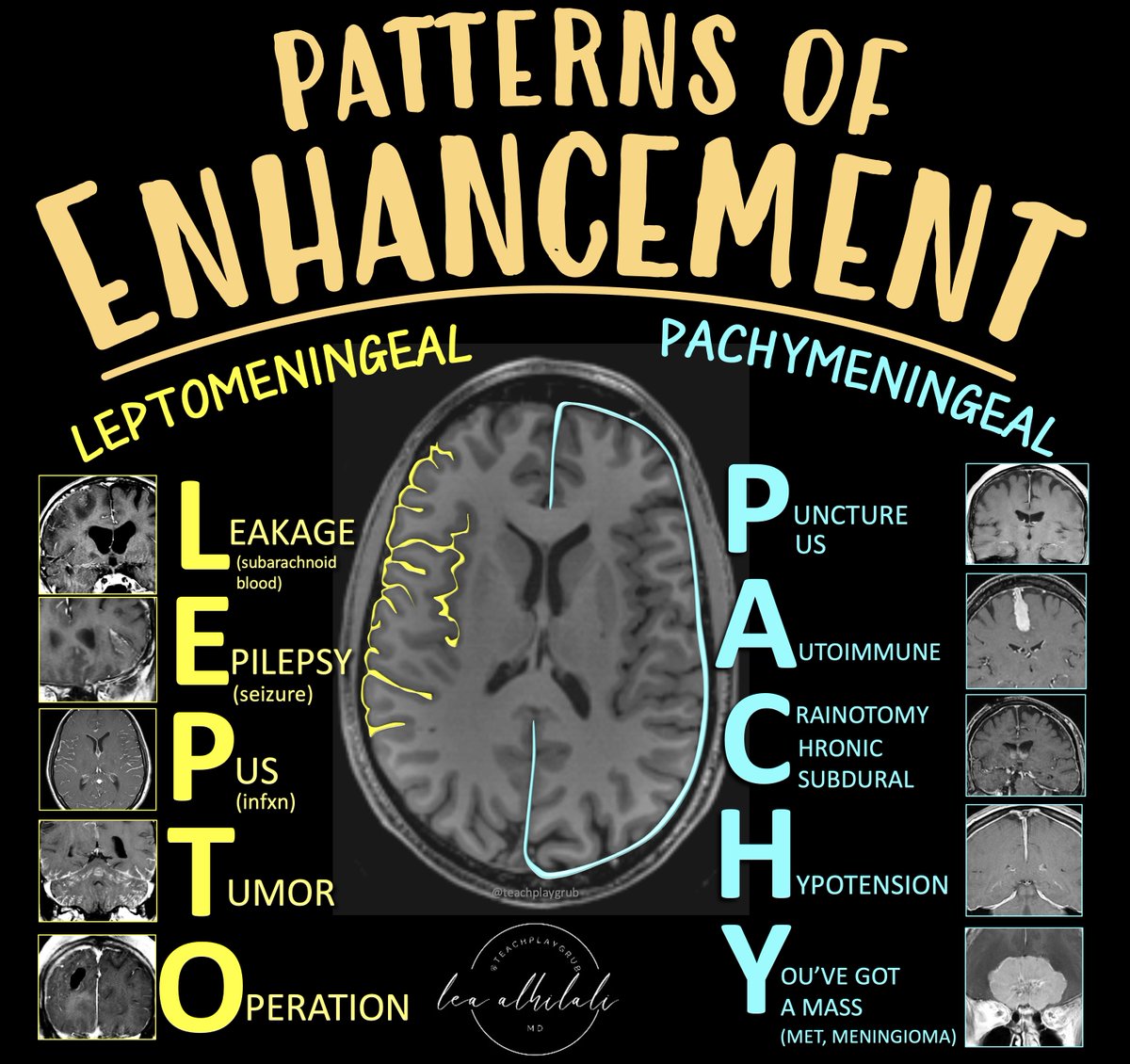
Need a DURABLE way to remember what causes DURAL enhancement?
Feeling left behind when it comes to leptomeningeal disease?
Here’s an easy way to remember the differential diagnoses for the two types of meningeal enhancement:
LEPTOMENINGEAL
Remember:
L = Leakage (subarachnoid hemorrhage)
E = Epilepsy (recent seizure)
P = Pus (infection, either bacterial, viral or granulomatous/fungal)
T = Tumor (leptomeningeal metastatic dz)
O = Operation (post operative)
PACHYMENINGEAL
Remember
P = Puncture (recent LP), Pus (subdural empyema)
A = Autoimmune (sarcoidosis, IgG4)
C = Craniotomy (post-op), Chronic subdural
H = Hypotension (intracranial hypotension)
Y = You’ve got a mass (mets, usually from direct bony extension, meningioma)
Now you’ve got a lot information PACH-ed into an easy & memorable mnemonic!
Which DBS target is best for PD patients with dyskinesia? @MichaelOkun
GPi suppresses dyskinesia but STN is associated with greater medication reduction.
#AspenCourse2023
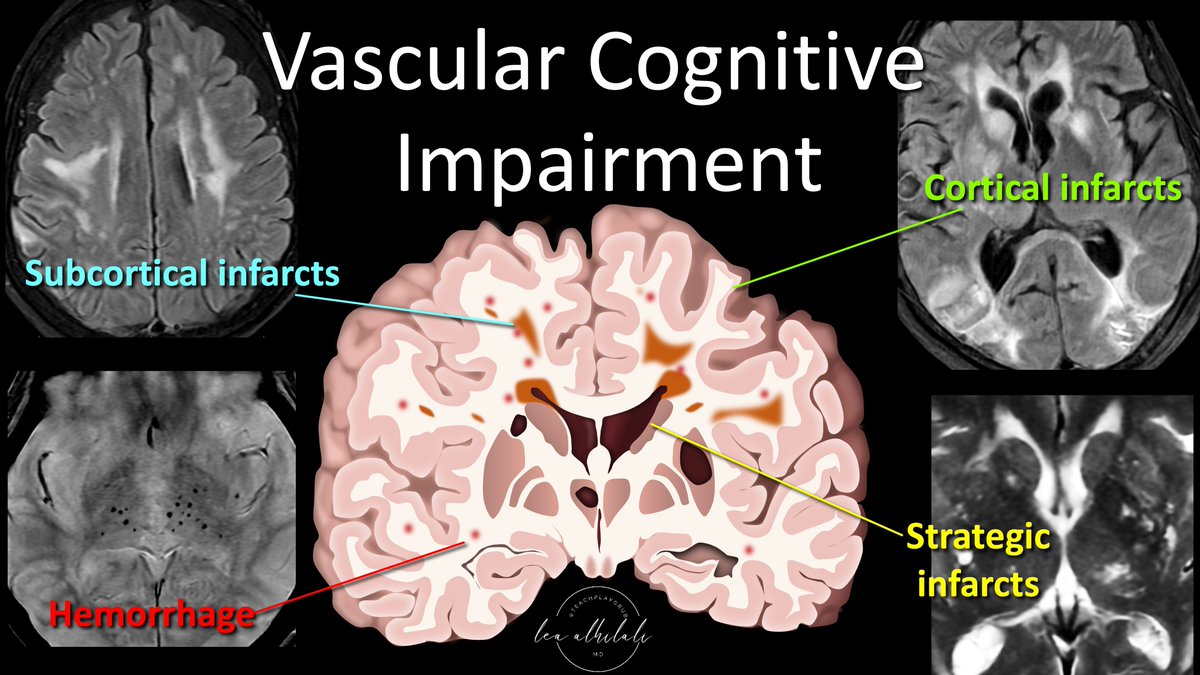
1/Having trouble remembering what you should look for in vascular dementia on imaging?
Almost everyone worked up for #dementia has infarcts. Which ones are important?
Here’s THE FULL #tweetorial this time on the key findings in vascular dementia
#meded#medtwitter#neurotwitter
This year at #AANAM I refrained from attending movement lectures (💔) to refresh my knowledge of other neurology subspecialties.
🧵Here’s 4 quick things I learned in:
1) Epilepsy
2) Headache
3) NCC
4) Neuroimmunology
#MedEd#NeuroTwitter#MedStudentTwitter#MedTwitter
Pearls from Prof @kailashbhatia 's talk on spectrum of autoimmune antibodies targeting surface antigens:
> Isolated Cranio-cervical Dystonia in NMDA
> NMDA as Sydenham chorea mimic in children
> Anti VGKC, Anti DPPX, Anti IgLON5 as MSA mimics
> Anti VGKC as CJD mimic
#AOPMC
Babinski and Friends!!!
“Loss of descending pyramidal control of the reflex arc to suppress extensor withdrawal results in the upgoing toes in the plantar reflex known as Babinski's sign”
1st described by Joseph Babinskiin 1896
#MedTwitter#neurotwitter#EndNeurophobia
1/