@AmericanAir While I understand your declination, I will certainly not fly again in American Airlines and transfer my mileage to a different carrier. Thank you
Another delayed flight on @AmericanAir AA2910 ORD to MIA , apparently “uncontrollable cabin temperature” While we value our security, it would be nice if you could keep passengers updated and facilitate rebooking. Will avoid flying with you in the future
@AmericanAir Thank you! I am unfortunately very frustrated and disappointed with this situation. Your airline has become so unreliable. Flight AA2910 was a mechanical problem so I am requesting a compensation for missing my international connection and losing 5+ hours at the airport
Another delayed flight on @AmericanAir AA2910 ORD to MIA , apparently “uncontrollable cabin temperature” While we value our security, it would be nice if you could keep passengers updated and facilitate rebooking. Will avoid flying with you in the future
Although all 4 trials were done in relapsed myeloma with 1-3 prior regimens, the type of patients varied including by type of prior exposure. So comparing head to head HRs is not advisable.
Patient and disease factors, access, affordability, and shared decision making come into play, especially in first relapse. In second relapse we have to also add belantamab. https://t.co/rMu8MdadmL
Just out: presented at #EHA26 and published @NEJM
Randomized trial of 2 talquetamab combinations vs DPd in relapsed myeloma. The Monumental-3 trial.
Both Talq-Dara-Pom and Talq-Dara beat DPd in PFS and OS.
Choice of a Talq combination vs Tec or Tec-Dara in relapsed myeloma will be driven by patient and disease factors and requires significant expertise. Congrats @RobertoMinaMD@PlasmaCellPete@mbeksac56@paurotero@mvmateos@thanosdimop@RahulBanerjeeMD et al.
https://t.co/DA04B3OjgS
Single arm phase II investigator initiated trials (IITs) used to be easier. Thats how I started my career. Budgets were low and institutions allowed you to open underfunded trials. Now due to a variety of factors the per patient costs of even single arm trials are very high, especially in oncology. Which means either you need industry support or NIH funding.
Industry funded IITs are the most common type but they naturally have to be of some interest to industry for you to get drug and funds. And that means collaborative development with some give and take.
NIH Grants and NIH cooperative group mechanism (ECOG, SWOG , ALLIANCE) is the second route. It’s quite a bit more tougher because there will be a lot of review and funding may not be sufficient. So often you need industry support in addition. But it is a good mechanism for truly important ideas to be tested.
Philanthropy and non profit foundations are a third path. More limited in number of trials that are supported this way.
I think if you are motivated single arm phase II IITs are a good way to start a clinical trial career. I strongly recommend that route. Much easier than trying to launch a career with a phase III. It builds your credibility and makes it more likely that in the future you will be in a competitive position to lead a phase III trial.
Start with a good clinical question and then work with pharma/NIH mechanisms to get a concept that’s mutually acceptable.
Phase I IITs may be a little difficult for young investigators to lead unless you have been involved in the lab development of the drug.
4/ Thank you to all physicians around world who completed survey and to @BrJHaem reviewers!
Special thanks to my partner-in-crime @GKaurMD on this, @VincentRK for encouraging us to push this to finish line, and our 🇦🇺🇮🇳🇨🇦🇺🇸 co-authors!
Link to article:
https://t.co/8XBeUodNUn
Need help keeping up on medical literature. Literally ask OpenEvidence to review major trial results over last three months for any disease you want. No more logging on to multiple journals.
@EvidenceOpen
Final results of the ATLAS trial are out: KRd > R post-ASCT maintenance in both PFS and OS.
Patients with high-risk dz or MRD positivity got 36 cycles of KRd; otherwise, standard risk + MRD negative (after 6 cycles) got only 8 cycles of KRd before de-escalation to R.
The obvious caveats are this was done pre-anti-CD38 era and most received thalidomide (vs len) during induction.
We did not see profound differences in dropout by study arm.
We do see that more is...more in this setting. And that MRD-guided de-escalation works for standard-risk!
#ASH25@End_myeloma moving the field forward with another MASTERful presentation (pun only partially intended).
While we’ve often defined FHRMM as 18 months after induction, times are a-changin’ with quads.
36 mo is the new 18 mo: if relapse ≤ then, go to bsAbs or CAR-T!
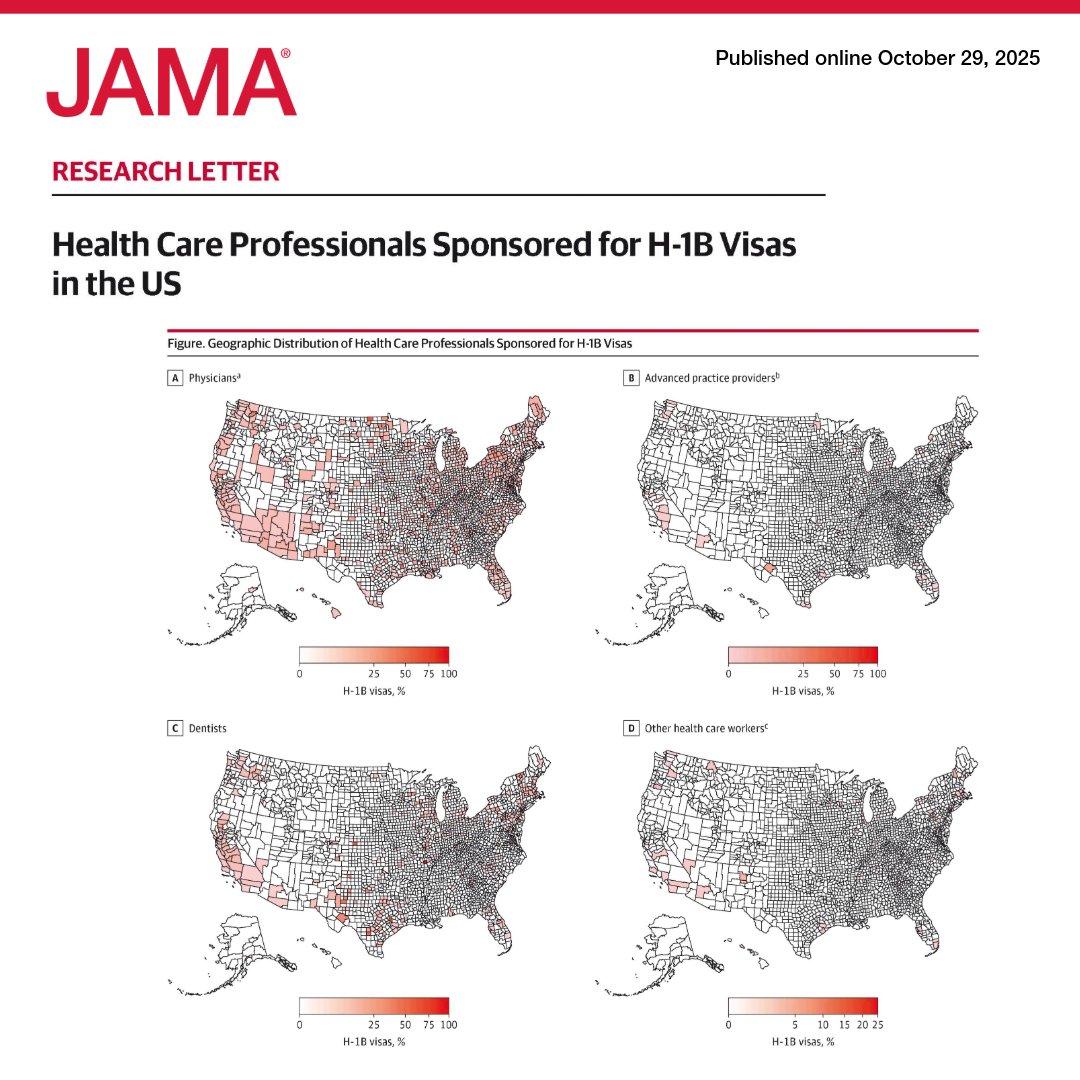
H-1B visa–sponsored physicians are twice as prevalent in rural counties and nearly 4 times as common in high-poverty areas, highlighting the potential harm of rising visa costs to health care access.
https://t.co/dtCf8oj8BJ
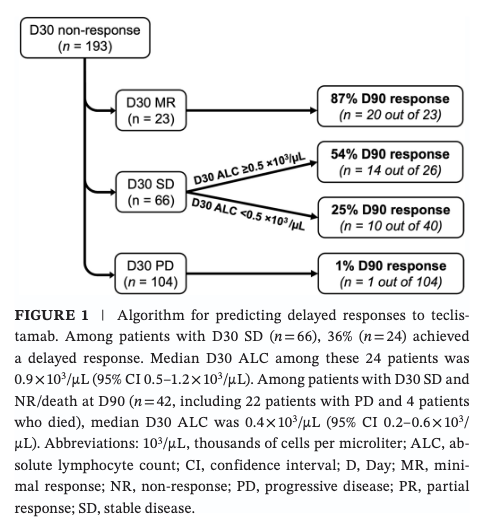
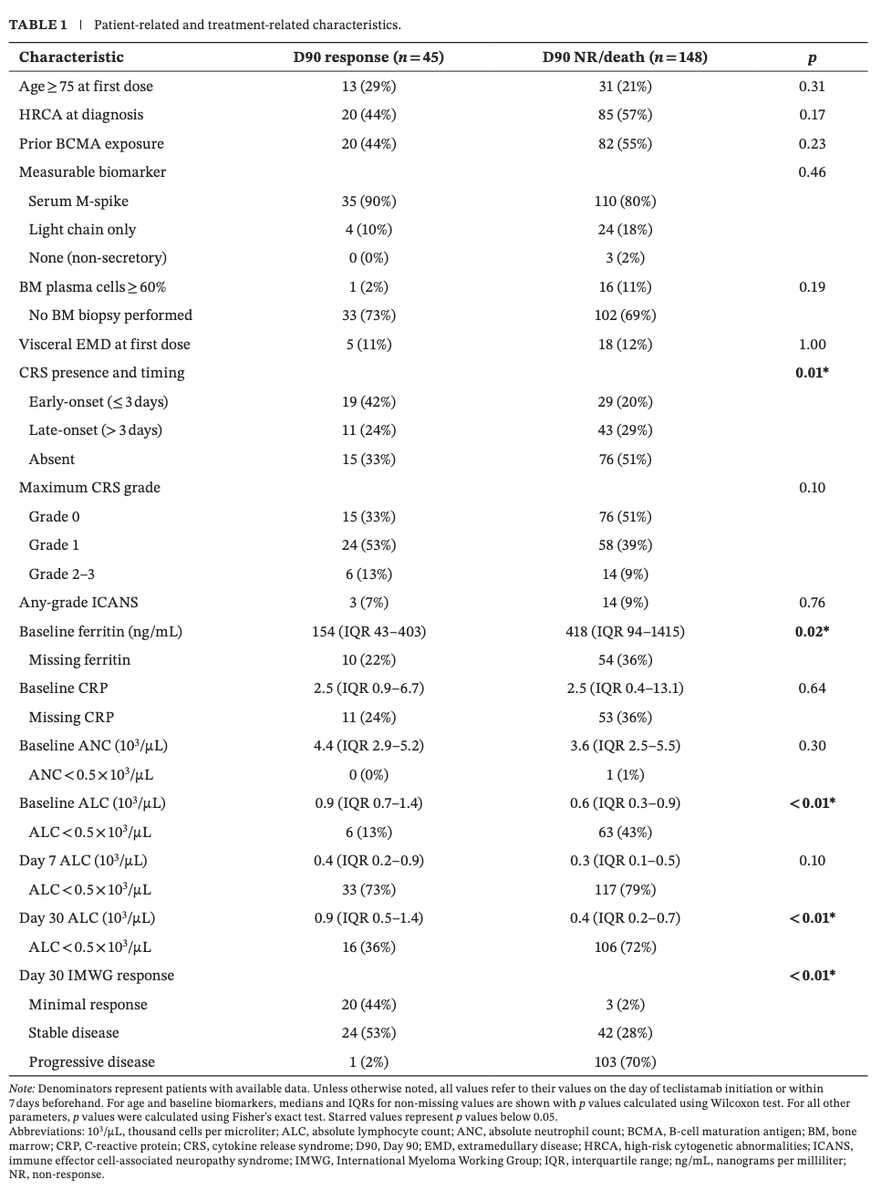
#Myeloma Paper of the Day: Study of delayed responses among D30 non-responders to teclistamab finds 2 predictors: (1) achievement of D30 MR (vs. D30 SD or PD)(CI 3.64–163); and (2) D30 ALC (CI 1.06–8.29); PFS was same for these delayed responders: https://t.co/XUmFo1HZHk. #mmsm
Exciting to see TRIMM-2 in print @BloodPortfolio! BCMA-sparing doublet that works well even in BCMA bsAb/CAR-T exposed.
We'd already heard about B-cell-sparing, but nice new gem in supplement:
Tregs also getting knocked out (likely by dara) ➡️ better efficacy vs tal alone?
Excited to share our newesr manuscript! Great collab w/ US Myeloma Immunotherapy Consortium showing impact of Flu LD exposure on CAR-T outcomes! Need prospective studies to validate model but even more 👀 on personalized chemo dosing! https://t.co/dCzmwKpax0
Bela-maf ODAC - votes against approval of blenrep in early relapse MM
1 in favor, 7 against for bela-Pom-dex
3 in favor, 5 against for bela-velcade-dex
— significant concerns with optimal dosing and ocular toxicity
I am not as surprised
#mmsm
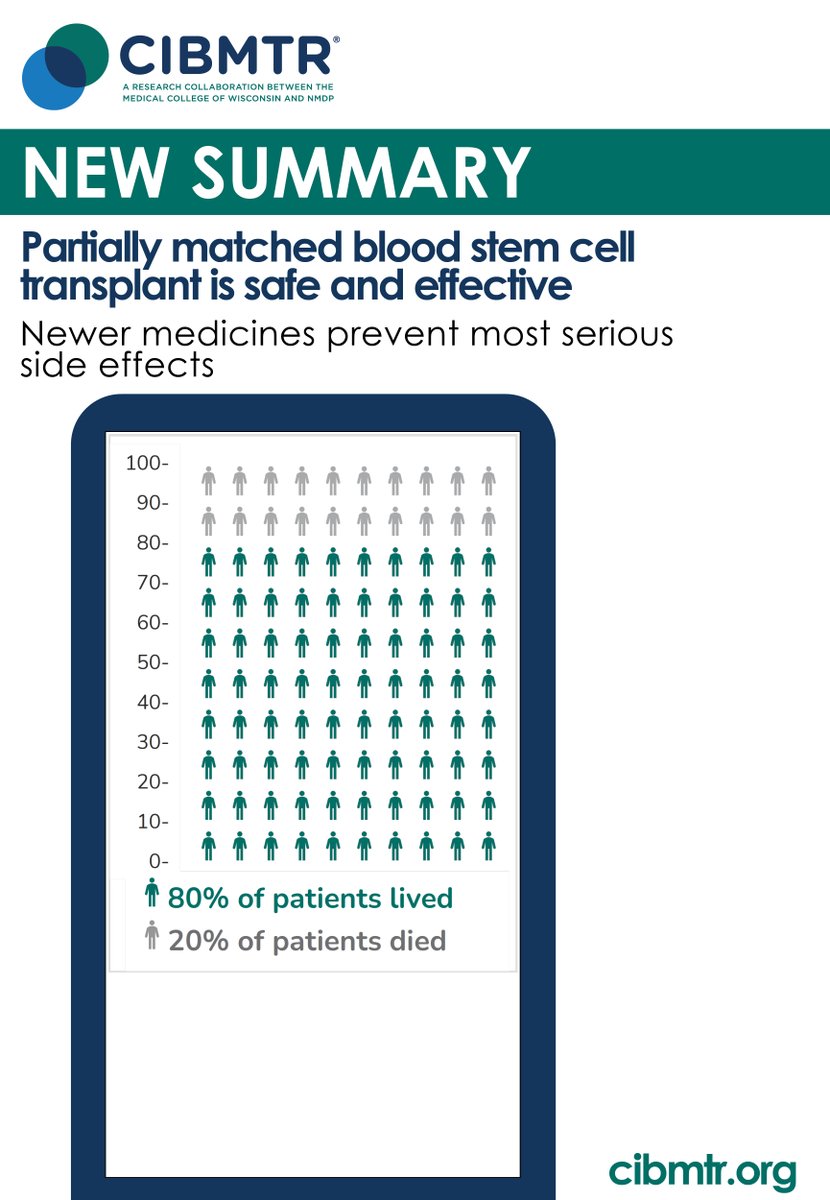
After a partially matched transplant, #GVHD can result. Previously, partially matched donors caused more GVHD than fully matched donors in cancer patients. A new approach, using cyclophosphamide, can prevent most GVHD. Read more: https://t.co/wPbdV37KB2
Excited to share findings from the multicenter ACCESS trial, supported by @CIBMTR & @nmdp_org . PTCy-based GVHD prophylaxis improved survival after MMUD HCT. Grateful for this collaboration advancing equitable transplant access. #ADonorForAll
https://t.co/1UJKPnOBM6
Another challenge with trial enrollment.
Most trials restrict enrollment to patients who have an M spike of 1 g/dL or free light chains of at least 10 mg/dL to enable full response adjudication.
But patients with ‘oligosecretory’ disease are excluded.
This becomes especially challenging with CAR T - if a patient responds to bridging therapy such that they no longer meet measurable disease criteria, and they may no longer be able to proceed on study.
With MRD taking focus over traditional response criteria, I don’t see why we need to abide by these precedents. The numbers are largely arbitrary anyway!