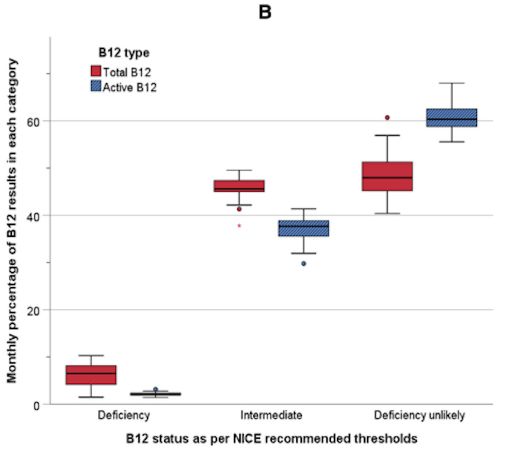
Better test ≠ better system.
This study shows that active B12:
🔍 Classifies more patients as deficiency unlikely
🔍 Reduces the grey “indeterminate” zone
Here’s the catch:
💸 It comes at a significantly higher cost ~26× more expensive !
💡 Take-home:
Better diagnostics don’t exist in isolation.
They live in real systems, with cost, access, and scale.
A great read if you’re thinking about lab medicine: https://t.co/bpMMsHMlvl.
#Pathology #LabMedicine #JCP
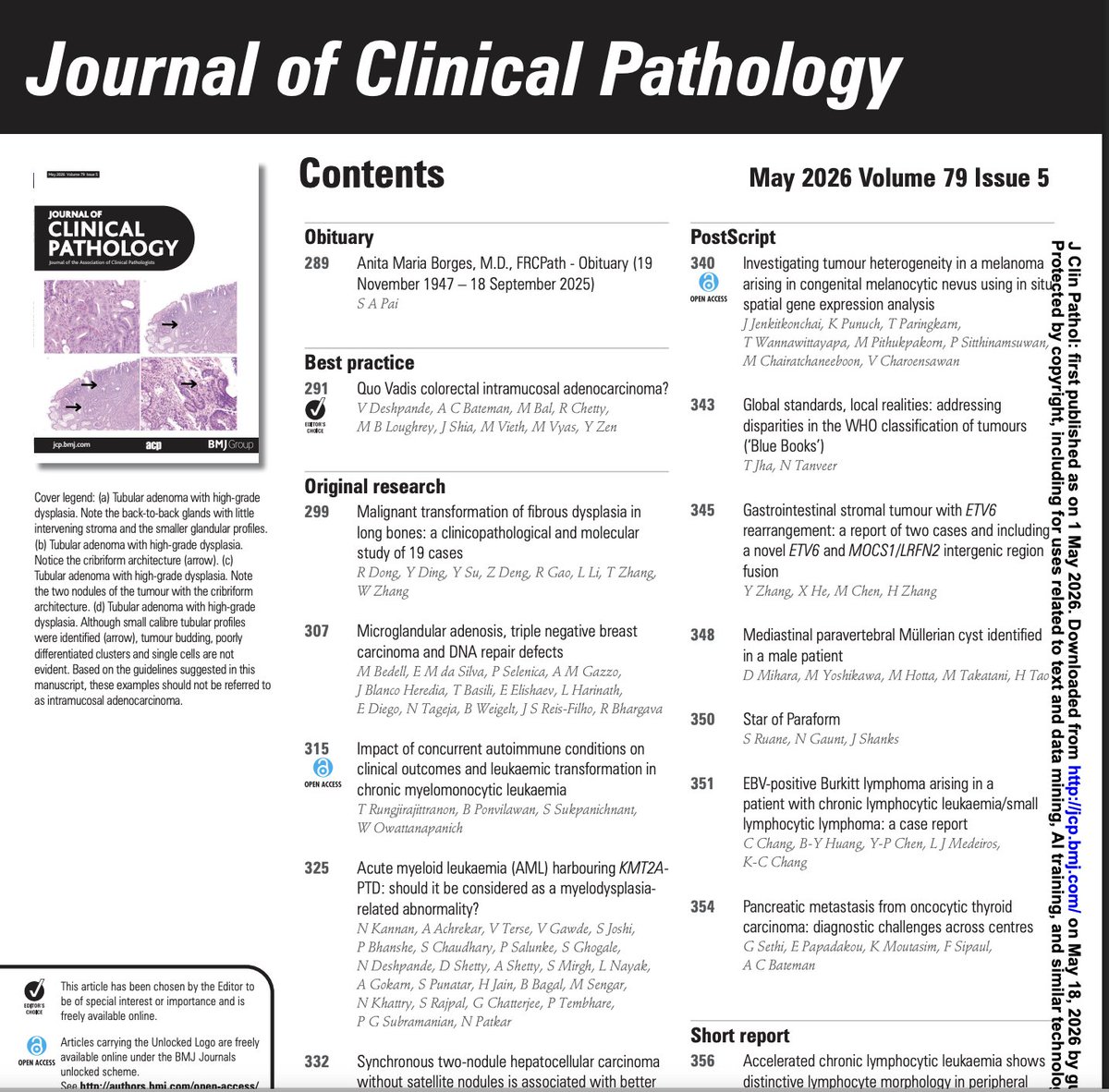
What’s inside the latest issue of JCP?
From evolving diagnostic dilemmas to rare case insights, the May 2026 issue brings together key reads across pathology.
Open Access Highlight: Autoimmune conditions & CMML outcomes.
If you read one paper today, make it this one!
#Pathology #HemePath #OncPath #OpenAccess #JCP #MedTwitter
Check out this paper on ELOC-mutant renal cell carcinoma highlighting the practical diagnostic features and differential considerations by the authors - Meifang Lin, Chuncheng Chen, Shujing Guo, Yue Wu, Fenglian Lin, Xin Ding.
Link to the article https://t.co/5fXCqKeXmF
Read this editorial titled "Extranodal extension in head and neck cancer: why HN-CLEAR matters and what still needs proof" by the authors - Dr Vikram Deshpande, Dr Munita Bal for an indepth understanding and clarity.
Link to the editorial https://t.co/5jP8eqCyg7
International Consensus Guidelines for Diagnostic Criteria & Checklist for Future Studies for Minimally Invasive Carcinoma ex Pleomorphic Adenoma: HN CLEAR Initiative
Beadle et al
https://t.co/MZdbPDvB7C
#HeadNeckPathol#HNPJ#HeadandNeckPath#Pathology#ENTPath#PathologyTweet
🔊 Our April issue is out now folks! Here are the highlights:
✒️ Editors choice: Histological reporting of locally excised pT1 colorectal cancer in the English Bowel Cancer Screening Programme
⭐ Synaptophysin expression in SMARCA4-deficient undifferentiated carcinoma of the esohagus - A potential pitfall
⭐ ELOC-mutant RCCs - Diagnostic features & Tips for diagnosis
⭐ Pan-TRK IHC in peripheral nerve sheath tumours - Does it truly indicate NTRK rearrangements ?
⭐ Review article: Patient safety in AI-powered diagnostic pathology
✒️ And don't forget to check two excellent editorials by @Vik_deshpandeMD and @mun_mm on
- HN-CLEAR consensus for ENE in H&N cancers: https://t.co/eMRcRWTxWb
- Advancing the diagnosis of IgG4-related ophthalmic disease: a critical appraisal of current criteria: https://t.co/MeGWkI35I2
Check out this paper - "High upgrade rate to invasive carcinoma makes subclassification of papillary carcinoma of the breast in core needle biopsy unnecessary" by Di Ai, Abdulwahab M Ewaz, Kevin Van Smaalen, and Xiaoxian Li.
Here is the link
https://t.co/kuJJVuVMH7
WHO-HAEM5 didn’t just rename entities: it reshaped B-cell neoplasm classification. Key updates across small and aggressive B-cell lymphomas highlighted here. More details here: https://t.co/U1cbb42k7r
Over the weekend, I had the privilege of attending the inaugural meeting of the GI Pathology Society of India—an outstanding event that, I suspect, will soon become a major force in education, research, and outreach in gastrointestinal pathology. What stayed with me most, however, was how often the conversation returned to the WHO Blue Books and their limited relevance in low- and middle-income countries. Colleagues repeatedly came up to me to say they shared the same concern: in their current form, these classifications do not reflect the realities of practice in countries like India. That matters. When pathologists working at enormous scale feel unseen by the very system that claims to set global standards, the problem is no longer merely technical; it is structural. By underrepresenting Indian and other LMIC pathologists, the WHO weakens the legitimacy and usefulness of its own classifications. The irony is unmistakable: a system designed as a global standard remains disproportionately shaped by perspectives from settings far removed from where most patients actually live and receive care.
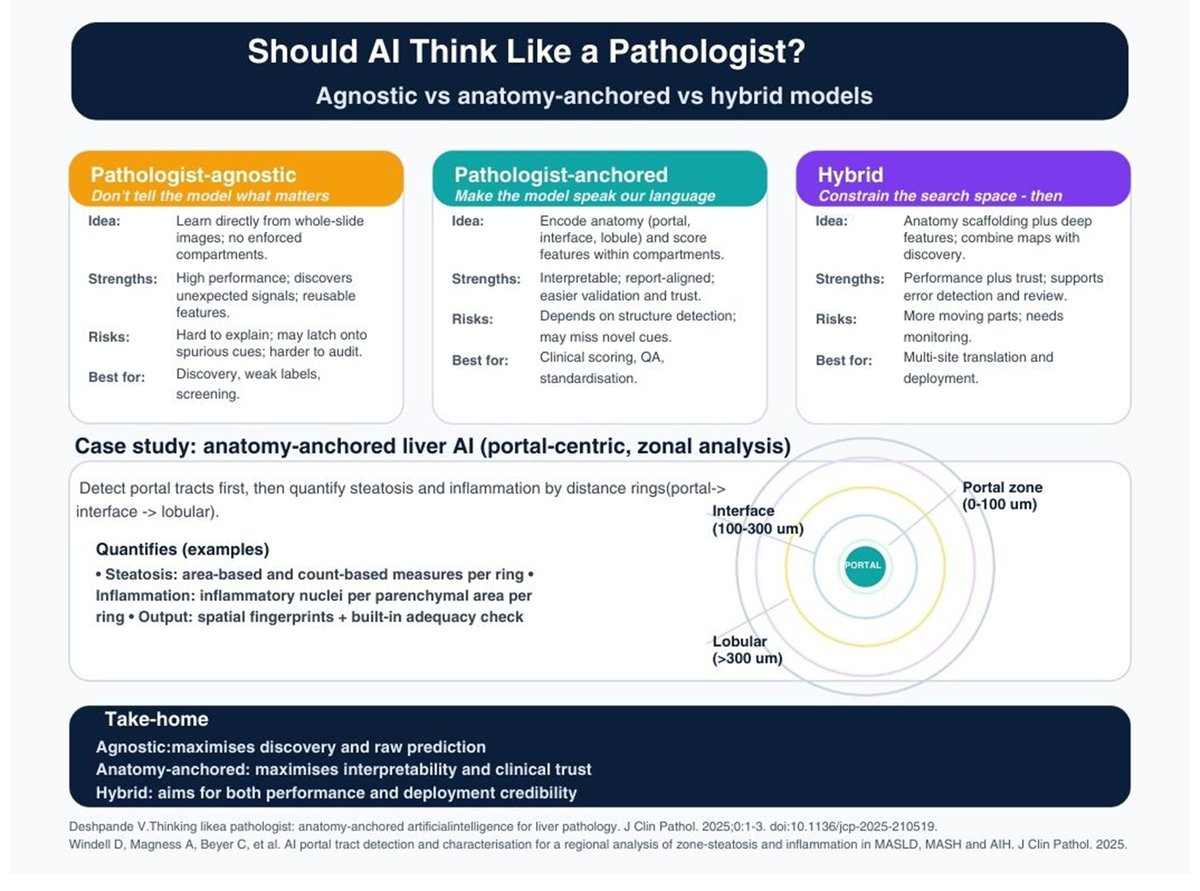
🌟Claudin 18.2🌟 Murtazaalieva G, Baldwin A, Fassan M, Deshpande V. Claudin 18.2 in cancer research and treatment: a pathologist's perspective. J Clin Pathol. 2025 Dec 17:jcp-2025-210328. doi: 10.1136/jcp-2025-210328. Epub ahead of print. PMID: 41407541.
when not to use the term)New paper alert! Our work on colonic intramucosal adenocarcinoma (when not to use the term) is now online in @JClinPath ahead of print. Quick video walkthrough of the key points.
#PathTwitter#GIPath#IMCA#Pathology
Fascinating discussion with Monika Vyas, Harshwardhan Thaker & Vidarshi Muthukumarana on IBEX AI pathology
Same slide, 5 runs = same heatmap. Zero variability. But focus size matters for the overall likelihood score.
#AIPathology#DigitalPathology#IBEX
IBEX AI in action with Monika Vyas, Harshwardhan Thaker & Vidarshi Muthukumarana Heat map overlay on H&E -- red = high cancer likelihood, blue = low. Toggle off and there's the adenocarcinoma. #AIPathology#DigitalPathology#IBEX
Deshpande V, Bal M. Extranodal extension in head and neck cancer: why HN-CLEAR matters and what still needs proof. J Clin Pathol. 2026 Feb 9:jcp-2026-210621. doi: 10.1136/jcp-2026-210621. Epub ahead of print. PMID: 41663234.
https://t.co/xSwYZavy9e
Two JCP reads on a familiar trap: iMCD-IPL can look like IgG4-related lymphadenopathy; in a sizeable fraction, the lymph node even meets common “IgG4-RD” numeric thresholds, and serum IgG4 isn’t reliably separating; what helps is stepping back: serum IgG4/IgG ratio (≈19% cut-off), total IgG (very high in iMCD-IPL), and the systemic inflammatory signature (CRP ↑, albumin/haemoglobin ↓), alongside careful morphologic pattern recognition; the take-home is practical: don’t let IgG4 counts drive the diagnosis in isolation—be explicit about iMCD-IPL in the differential and align the pathology call with the clinical/lab context.https://t.co/ZvalpQ8da8 https://t.co/PfguFLmG95