@rocu_bene Except it’s not one or the other. Perfectly reasonable to gain control w provider 1 putting in an IO and provider 2 putting in a CVL. Maintains forward momentum
CRYOSTAT2 results #ccr23:
- Early *empiric* administration of high-dose cryoprecipitate to trauma patients activating the major haemorrhage protocol did not improve 28-day mortality.
- possible evidence of harm if given very early or in penetrating trauma patients...
The @PATCHTrial, led by @RussellGruen, a study of pre-hospital TXA for severe trauma in adults at high risk of acute traumatic coagulopathy treated in advanced trauma systems, has been published today in @NEJM. #CCR23 Here’s a summary of what we did...
https://t.co/fl3m8liWB2
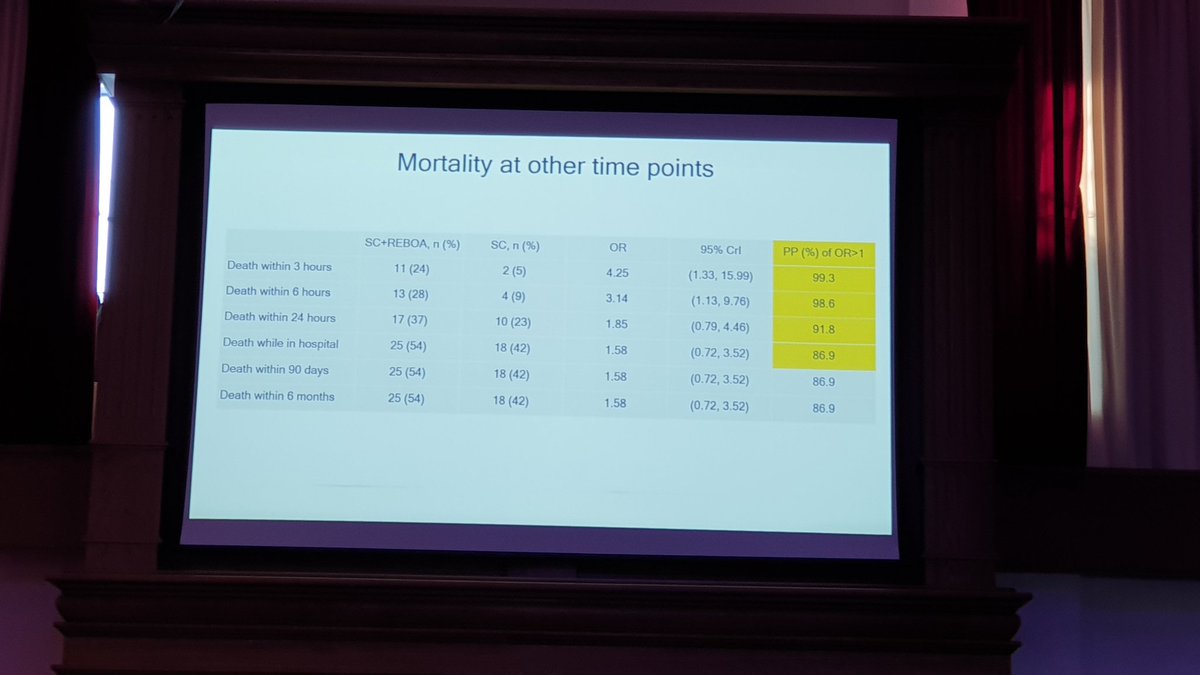
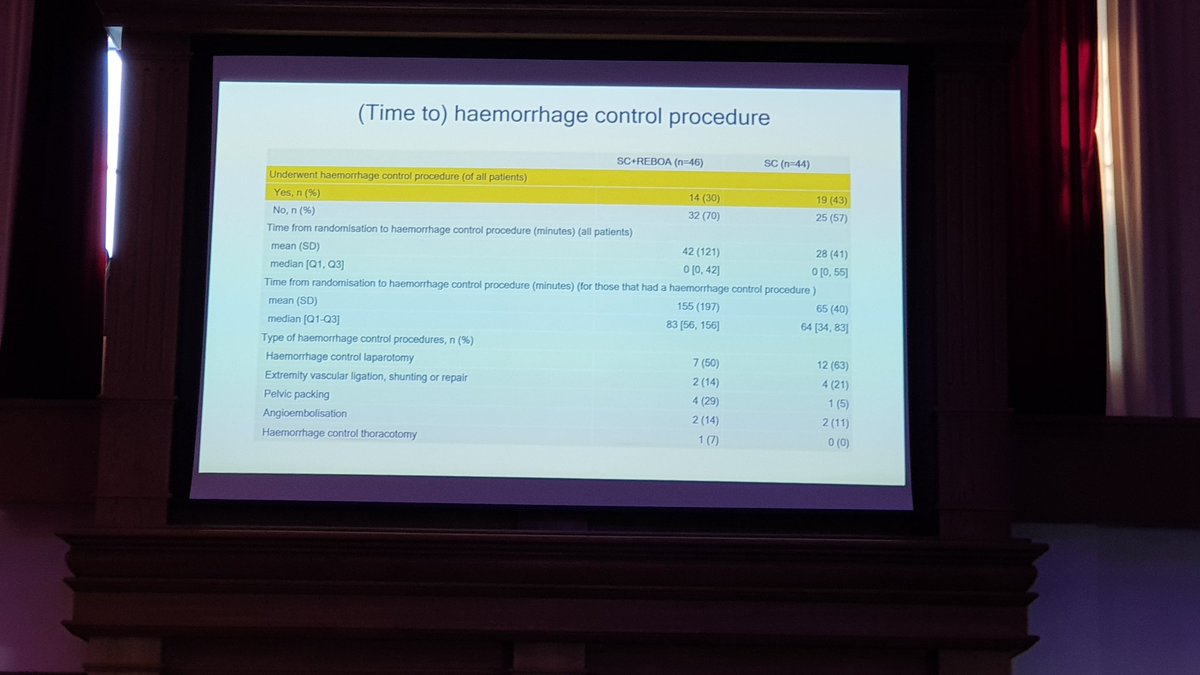
UK-REBOA results:
REBOA increased mortality at 90 days and at all interim time points.
REBOA increased deaths due to bleeding at 3 hours and 90 days.
REBOA substantially delayed time to definitive haemorrhage control.
💢🎈💢
#ccr23
@lotusgav Especially given that red cells rarely the product we need for elective procedures at risk of bleeding…. Thanks for the updates gav, loving it so far!
@GongGasGirl Maybe. But in an era of staffing issues etc, I bet we’re more efficient keeping radiographers in an environment they can control and are used to. We are pretty good at taking ICU patients anywhere (angio suites, MRI etc)
Peripheral noradrenaline vs metaraminol on ICU
Metaraminol more $$$, no benefit
Suspected noradrenaline extravasations required no additional management
Small single centre study but in keeping with the body of literature on this topic
https://t.co/hV5nAa5fSA
#Dogmalysis
@periopTTEcho@lotusgav Agreed. That’s my approach too. Pedagogically good to accentuate the heightened importance of analgesia in these ones though I reckon