Inspired by the recent Celiac disease post at @CPSolvers by @rabihmgeha and @DxRxEdu , here is my first attempt at #MedTwitter
Any comments and suggestions appreciated!
Thanks.
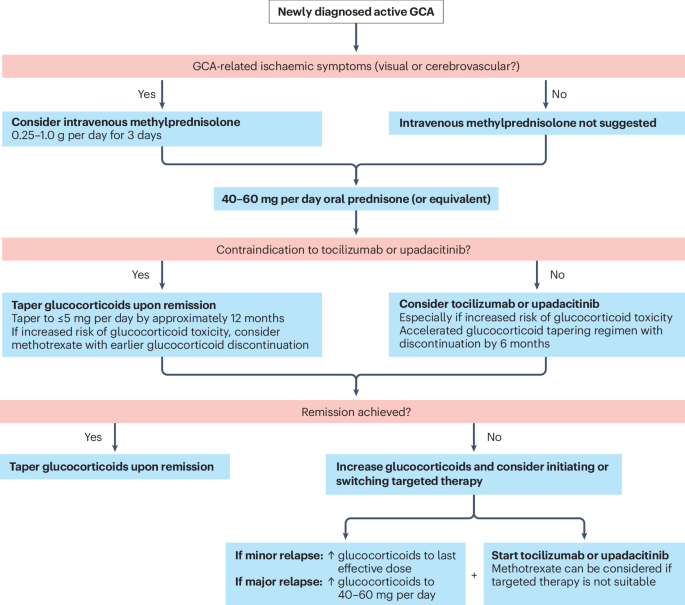
What's a D-dimer?
Fibrinogen = 3 domains = central E + 2 D
Thrombin cleaves fibrino-peptides (A,B) in E
= Fibrin monomers
With fibrin-peptides A + B gone monomers can polymerize
Fibrin monomers polymerize = Fibrin polymers
FXIIIa crosslinks D in polymers = (D-D)E-(DD)E... = cross linked fibrin->clot stabilized and leaves behind some (d-D) = D-dimer!
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
🫀Heart failure in 2026: we are no longer treating symptoms. We are redesigning the disease.
The latest evidence update reminds us of something profound:
Heart failure is no longer a single entity.
It is a spectrum, and now, finally, we are treating it as one.
Several paradigm shifts stand out.
1. SGLT2 inhibitors are no longer “add-on” therapy.
They are foundational across the entire EF spectrum.
From HFrEF to HFpEF, the data are now consistent.
Not just symptom improvement, but hard outcomes.
This may be the most important unifying therapy in modern HF.
2. HFpEF is no longer a therapeutic desert.
For the first time, we have real disease-modifying options:
Finerenone → outcome reduction across EF ranges
GLP-1 / dual incretin therapies → targeting the obesity phenotype
Structural and metabolic mechanisms are finally being addressed
We are moving from “HFpEF frustration” → HFpEF phenotyping.
3. Acute heart failure is no longer about stabilization.
It is about early transformation.
The new paradigm:
Start GDMT in-hospital
Optimize rapidly
Treat beyond congestion
Decongestion is still important, but it is no longer the goal.
Disease modification starts on day 1.
4. Decongestion is becoming precision medicine
Urine sodium-guided therapy
Early escalation of loop diuretics
Sequential nephron blockade
Not just “give furosemide”, but measure, adjust, and target response.
5. Devices are no longer rescue therapy, they are integrated care
TEER expanding from mitral → tricuspid
Pulmonary artery pressure monitoring reducing hospitalizations
Remote hemodynamics shaping outpatient management
The boundary between ICU, ward, and home is dissolving.
6. The biggest problem is no longer evidence.
It is implementation.
We already have:
Quadruple therapy
Proven outcome benefits
Yet many patients never reach target doses.
The gap is no longer science.
It is execution.
🤓Final message
Heart failure care has entered a new era:
Mechanism-based therapy
Early aggressive optimization
Phenotype-driven treatment
And perhaps most importantly:
We are no longer chasing symptoms.
We are altering the trajectory of the disease.
📃Reference
Liori S, et al. Heart failure evidence update 2026. Heart Failure Reviews. 2026. https://t.co/T4MVjK0vGd
💉The 2026 Anaphylaxis Guidelines highlight something uncomfortable for all of us in acute care:
we do not fail because we lack knowledge, but because we fail to act on what we already know.
Across 12 international guidelines, there is almost perfect agreement on one point:
intramuscular epinephrine is the first and most important intervention⚠️. Yet in real practice, it remains significantly underused, often replaced or delayed by antihistamines or corticosteroids, therapies with no evidence for acute life saving benefit
This gap between evidence and behavior is the central clinical problem.
From a bedside perspective, three insights are particularly relevant:
First, diagnosis remains the main bottleneck, not treatment.
The guidelines clearly show that variability in diagnostic criteria, especially in patients without skin manifestations or in infants, leads to hesitation. Clinically, this reinforces a key principle:
-> anaphylaxis is a clinical diagnosis driven by physiology, not by complete textbook criteria. Waiting for skin signs or full multisystem involvement delays epinephrine and worsens outcomes.
Second, the document reframes management from a pharmacologic problem to a systems and education problem.
Underrecognition by clinicians, lack of training in schools and community settings, and poor patient education all contribute to undertreatment. In reality, the success of anaphylaxis management depends less on ICU level interventions and more on early recognition and immediate action in prehospital environments.
Third, there is a clear shift toward proactive risk management rather than reactive treatment.
Modern guidelines emphasize emergency action plans, patient carried epinephrine, and structured education programs. This aligns with a broader trend in critical care: outcomes improve when interventions occur before physiological collapse, not after.
An important nuance for critical care physicians is the role of adjunctive therapies.
Antihistamines and corticosteroids are consistently positioned as SECONDARY, non life saving treatments. Their continued overuse reflects a cognitive bias toward treating visible symptoms rather than addressing the underlying hemodynamic and airway threat. Clinically, this is equivalent to treating hypotension in septic shock with paracetamol.
🤓Bottom line:
Anaphylaxis is one of the clearest examples in medicine where the evidence is simple, but implementation fails.
The priority is not new drugs or devices, but closing the gap between recognition and immediate epinephrine administration.
📃Reference
Wallace DV, Immunol Allergy Clin N Am ▪ (2026) https://t.co/VoarNwD7v7
🤓🔥The 2026 Surviving Sepsis Campaign update are out!! And does not overturn sepsis care, but it clearly shifts the field from rigid protocol thinking toward more individualized decision making, stronger implementation, and broader recovery planning.
From a bedside perspective, the most important change is not a new miracle therapy, but a more clinically mature framework. Compared with 2021, the 2026 recommendations place greater emphasis on structured sepsis response systems such as a code sepsis or sepsis huddle, continued rejection of qSOFA as a stand alone screening tool, and a more operational diagnostic pathway using cultures, lactate, and early clinical reassessment.
The antibiotic message is also more refined: immediate treatment within 1 hour remains central for septic shock and for probable or definite sepsis without shock, while possible sepsis without shock still allows a short diagnostic window before antibiotics, rather than automatic indiscriminate administration.
The hemodynamic section is where the philosophical shift becomes most visible. The 30 mL/kg initial crystalloid strategy remains, but 2026 makes the reassessment mindset more explicit, including how weight can be calculated in obesity and when early concurrent vasopressors may be justified in unstable shock. Balanced crystalloids remain preferred, but routine albumin is de emphasized, with the panel now suggesting crystalloids alone over crystalloids plus albumin, while acknowledging that albumin may still be reasonable after large crystalloid exposure or in cirrhosis. This is a meaningful departure from 2021, where albumin was suggested more directly after large crystalloid volumes. Just as important, 2021 had no recommendation on restrictive versus liberal fluid strategy after initial resuscitation, whereas 2026 now allows either approach after the first 30 mL/kg based on patient and system factors, and even introduces the concept of active fluid removal after the acute resuscitation phase. Clinically, that is a major step toward phase specific resuscitation rather than endless fluid accumulation.
Another relevant evolution is that 2026 is more explicit about what not to do. The guideline suggests AGAINST using antipyretics to improve outcomes, against IV vitamin C, against blood purification techniques, against vitamin D, and against probiotics for sepsis treatment. That matters because the update is telling us, more clearly than before, that sepsis care should focus less on physiological cosmetic correction and more on interventions with plausible patient centered value.
🤓Bottom line:
The 2026 SSC guideline is less protocol driven, more phenotype aware, and more longitudinal in its view of care.
📃References
Prescott HC et al. Surviving Sepsis Campaign. Intensive Care Med. 2026. DOI: 10.1007/s00134-026-08361-1.
Surviving Sepsis Campaign 2021. DOI: 10.1007/s00134-021-06506-y.
1/
Flavors of PEA - PRIS, PREM & What to Do with Them by Dr. Jason Nomura
#REVIVE2026
PREM - pulseless rhythm with echo motion
PRES - pulseless rhythm with echo standstill
Lots of new terminology in the medical literature
@CardioNerds@OscarJMitchell@Gurleen_Kaur96
Causes of hypopituitarism are a lot like bone marrow disorders;
Myelophthisis: infiltration
Aplastic: aplasia
Precursor deficiency (Fe/B12): Hypothalamic dysfunction
Bonus:
AIHA (Norm BM with peripheral destruction) ~ Laron dwarfism(Normal Pituitary with GH receptor abn)
@CPSolvers The OG Rabih and Reza!! Their love, passion and devotion to the art that is medicine bleeds through their every word as they dissect a complain as trivial as cough! A must listen for every Medstudent remotely fascinated with medicine. ALERT: you may fall in love <3
Like Spotify wrap-up, can we also have a top 10 study moments? Like a quick flip through those moments and days where new concepts blew your mind or you had an Aaha moment? #lifeofaResident
@Kamal_MAMC Medicine got doxxed with tox reviews this year. Most OG faculty retired, quality dipped. Also, crumbling infra. What sustained it this far was quality peers. Now, even that adv will go away.
Octreotide pearls
1. When a patient comes in with upper GI bleeding, you do NOT need a PPI with octreotide because “it may be an ulcer”. Both drugs raise the gastric pH to the same amount
2. Octreotide stops working after 3-6 days.
4/ Clinical Pearls
Ponatinib is the only TKI active against all known BCR-ABL mutations, including T315I.
For CML, reserve for multi-TKI resistance or T315I mutation; not for front-line use.
For Ph+ ALL, the PhALLCON trial supports front-line combination with chemo — now FDA-approved (accelerated).
De-escalate dosing (30→15 mg) after achieving MRD-negative remission or MMR to minimize vascular risk.