OpenVAERS takes the PUBLICLY available data from VAERS and make it more user friendly. We are a PRIVATE entity, not affiliated with HHS, the CDC or the FDA.
I've written thousands of articles over the past 20 years, but this is the most important one I have contributed to the age-old debate between "viruses don't exist" and "viruses are lethal." I encourage you to share it with health practitioners, who probably have no idea that common environmental exposures, such as microplastics and metals, can mimic EXACTLY the symptomology of contagious infectivity, commonly misdiagnosed as viral in origin. And for those who think this is "magical thinking," they can consult the 60+ references at the end of the article. This is a REAL problem, and it contributes significantly to what the WHO and CDC promote as the cause of the majority of epidemics and pandemics. I don't think you'll be disappointed. I encourage comments and criticisms.
📎https://t.co/CzIgya9tW8
React19 and ICAN have formally put HHS, FDA, and NIH on notice.
For five years, the vaccine injured have been ignored, dismissed, denied care, and left without answers. Safety signals were overlooked. Families were abandoned. Accountability never came.
That ends now.
Our submission to federal health agencies details years of suppressed safety concerns, a broken compensation system, and the real human cost carried by thousands of Americans.
To the injured: do not give up.
We are not stopping anytime soon.
Read more here: https://t.co/gorqNyGaIT
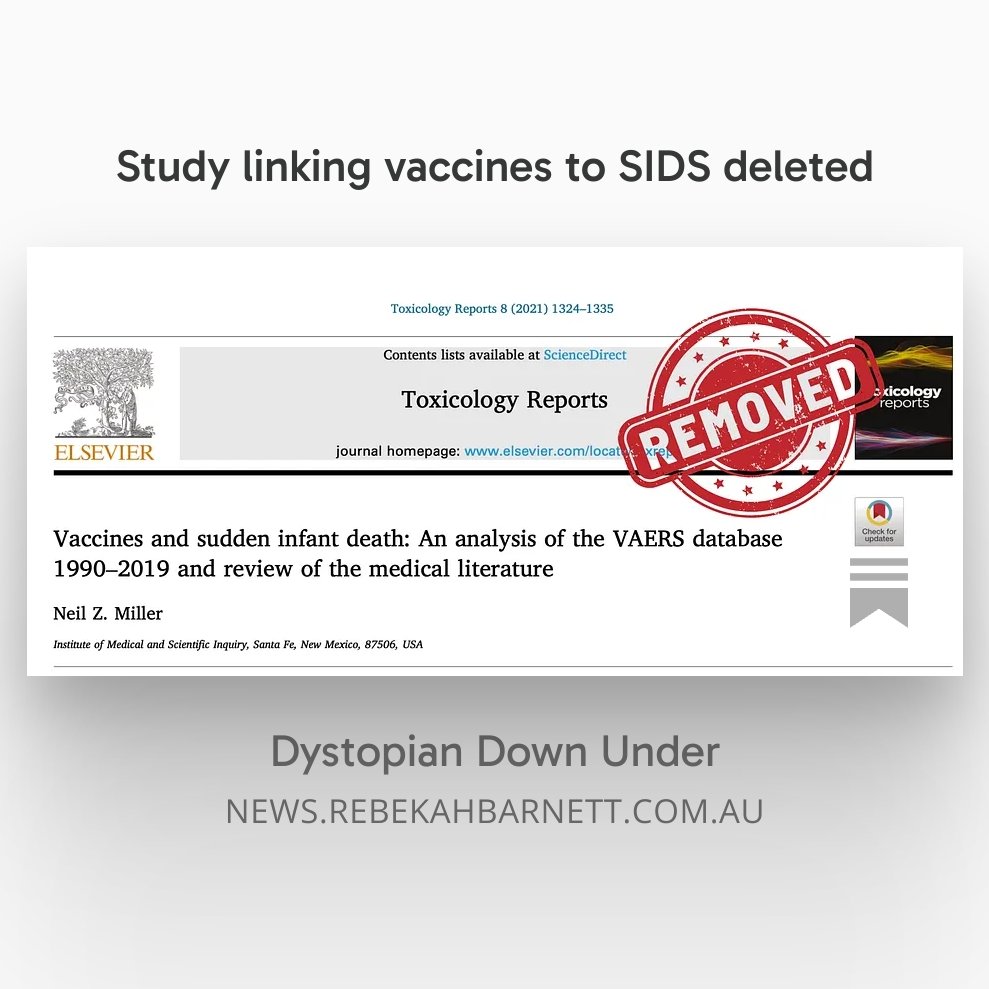
Study linking vaccines to SIDS deleted 🚨
A major science publisher says the peer-reviewed article is too dangerous for doctors and parents to read...
https://t.co/lGPEE4sxdG
Gardasil 4 was licensed in 2006. Gardasil 9 was licensed in 2014. This is a perfect example where there was an ignored signal. Not because they didn't know, but because they decided that POTS was not serious enough to warrant action. There is no other way to explain it.
Further, this is one of those, no it was not reporting bias cases. No one expected POTS.
Tucker Carlson admitted he used to make fun of people who believe vaccines cause autism.
He now describes his behavior as “unthinking, stupid, and reactionary.”
Tucker says people are noticing what Robert De Niro noticed about vaccines before he suddenly abandoned the issue: “There’s something there that people aren’t addressing” with vaccines and autism.
De Niro declared this on “The Today Show” back in 2016. Let the clip roll, and you’ll see it.
Fast forward to today, and it’s hard to believe De Niro actually said what he did on mainstream television.
What’s even harder to believe is just how most of the vaccines used today got approved in the first place.
“Placebo” doesn’t mean what most people think it means when it comes to vaccines.
Once you understand what a vaccine “placebo” is, the way evidence gets buried starts making a lot more sense.🧵
Arendt’s Banality of Evil & Medical Compliance
Hannah Arendt didn’t find a monster in Adolf Eichmann.
She found a bureaucrat.
A man who organized train schedules.
Who filed the correct forms. Who advanced through institutional hierarchies by demonstrating competence and reliability. Who, when asked at trial whether he had committed evil, expressed genuine confusion.
He had only done his job.
Arendt’s term for what she observed has entered the language: the banality of evil. Not the dramatic, ideological, consciously malevolent evil of mythology. The quiet, procedural, unremarkable evil of ordinary people performing ordinary functions inside systems whose overall direction they never personally chose to examine.
The mechanism Arendt identified was breathtaking in its simplicity.
Thoughtlessness.
Not stupidity. Not moral weakness. Not cowardice, necessarily.
The suspension of the active, questioning, morally engaged thinking that asks: what am I participating in?
Now look at 2021.
The physician who processed the mandate paperwork without reading the trial data. The hospital administrator who drafted the policy excluding unvaccinated visitors and filed it alongside fifty other administrative documents that week.
The nurse who enforced the protocol and noted the patient’s distress and continued. The regulator who approved the expanded authorization without examining the subgroup analyses.
None of these people were required to be monsters. They were required only to stop thinking in a particular direction.
The system provided everything needed to make that easy. Clear protocols. Institutional consensus. Professional community. Legal cover. Moral language that made compliance feel like care.
Thinking, genuine, active, uncomfortable, morally engaged thinking had to be chosen deliberately against the grain of every structural incentive available.
Most people did not make that choice. Not because they were bad, even though a lot of them are out there. Because thinking that way is genuinely hard and the system was specifically organized to make it feel unnecessary.
Arendt’s conclusion was not despair. It was a call.
Critically Think. Not occasionally. Not when it’s professionally convenient. As a constant, active practice, especially inside institutions, especially under pressure, especially when the language of necessity and safety and consensus is loudest. It should be common sense in 2026.
Because the absence of thinking is not neutral. It has a direction.
And that direction has a history.
“But I say to you who hear: Love your enemies, do good to those who hate you, bless those who curse you, and pray for those who spitefully use you.”
Every obedience experiment in history had the same overlooked finding.
Not everyone complied.
In Milgram’s lab, 35% refused to deliver the final shock. In Asch’s line experiments, 25% never conformed, not once, across any trial. In Zimbardo’s prison, at least one guard refused to dehumanize. One prisoner demanded a lawyer instead of a doctor and broke the psychological frame entirely.
We spent decades studying the ones who obeyed.
We barely asked what made the others different.
That question matters more now than it ever has.
The resisters in the COVID era were not difficult to find. Physicians who filed exemptions and lost their licenses. Nurses who walked away from careers rather than mandate patients into decisions they hadn’t genuinely chosen. Scientists who published contrary data knowing what it would cost them. Parents who stood alone at school board meetings. Ordinary people who simply said, quietly, without drama , no.
What made them different?
Research consistently identifies a cluster of factors. Not personality traits you either have or don’t. Situational and cognitive patterns that can be cultivated.
First: prior reflection on authority. The resisters had usually thought, before the crisis, about the limits of institutional trust. They weren’t cynics. They were people who had already asked the question “under what conditions would I refuse?” before anyone was asking them to comply.
Second: a concrete reference point outside the consensus. A value, a principle, an oath, a relationship that existed independently of the institutional structure demanding compliance. Something the system couldn’t reach.
Third: at least one other person. Milgram found that a single dissenting confederate reduced compliance dramatically. The resisters rarely stood entirely alone. They found each other. Sustained each other. Gave each other permission.
Fourth: the willingness to tolerate social pain. Not immunity to it. Tolerance of it. They felt the pressure. They felt the exclusion. They chose the discomfort of integrity over the comfort of belonging.
None of this is innate. All of it is learnable.
The most important thing Milgram, Asch, and Zimbardo taught us is not how fragile conscience is.
It’s that conscience can hold, if you’ve trained it, named its limits, and found even one other person willing to hold theirs beside you.
Build that now. Because the experiment is always running.
Until then stay humble.
⚠️ This will rattle you to your core.
The families of two Black infants who died in a 1960s gov't RSV vaccine trial have filed a federal lawsuit, alleging researchers enrolled the children in a medical experiment without parental consent. 🧵
https://t.co/tQS4X8e3H7
I have come to the conclusion that in almost all cases the researchers do not understand the databases they work with nor do they read individual reports. They stay entirely within the easily assessable fields. My guess is most dont even do the queries themselves but delegate to a computer science geek, receive a table of results they have been taught to crunch.
Very cool work @aravindmohanoor !
I think these entries fall into three classes.
1. Bypass��� I had a fall off a ladder as a child.. it left me a scar on my shoulder. Right next to that I now have a large tumor from the vaccine.
2. Direct—I became very dizzy and fell off the ladder two hours after my shot.
3. Comparison (like your sunburn example).
The value from AI is that we can have it analyze each report and generate statistics based on this type of scale and set it to go, whereas a human doing this would take years.
The hatred directed at the unvaccinated was never really about the unvaccinated.
Jung would have known that instantly.
Because he spent his career studying what happens when human beings cannot face what lives inside them. The answer is always the same. They find someone to put it in.
Jung called this projection. The unconscious transfer of an internal psychological content, a fear, a weakness, an unacknowledged doubt, onto an external figure who then carries it for the group.
It is one of the oldest and most reliable mechanisms in human psychology.
And in 2021, it ran at civilizational scale.
Think about what the pandemic had actually produced in the compliant majority. Genuine fear of death. Deep uncertainty about whether the interventions they had accepted were truly safe. Suppressed grief over lost time, lost connection, lost autonomy. Unexamined anxiety about whether they had thought critically enough before complying.
None of that could be faced directly. Facing it would mean confronting the possibility that the certainty was false, that the compliance had costs, that the authority was imperfect.
So it was projected.
The unvaccinated became a container for everything the vaccinated could not hold.
They were selfish, carrying the projection of the resentment people felt but couldn’t express toward the institutions that had restricted their lives.
They were dangerous, carrying the projection of the fear that the vaccinated still felt despite their compliance.
They were irrational, carrying the projection of the doubt that had been suppressed rather than examined.
The intensity of the hostility was not proportional to the actual epidemiological risk the unvaccinated posed.
It was proportional to the size of the shadow being projected.
Jung’s diagnosis of this dynamic was precise: the more violently a person or group insists on the evil of the other, the more certain you can be that they are encountering their own rejected contents in the mirror.
The way out is not more argument. You cannot reason with a projection. You can only withdraw it.
Which means the most radical thing any of us can do, now, and in whatever comes next, is look honestly at what we are projecting and why.
The enemy you are most certain about is usually closest to home.
Arne Burkhardt opened the bodies.
What he found should have stopped everything. Vaccine-derived spike protein in heart tissue.
In blood vessel walls. In brain tissue. In multiple organs across multiple cases. Not in one anomalous death.
Consistently. Repeatedly.
With inflammatory patterns and lymphocytic infiltrates that follow directly from the known mechanism of mRNA vaccination, widespread, systemic spike protein production that the manufacturers and regulators always claimed would stay local and resolve quickly. It did not stay local. It did not resolve quickly.
Burkhardt found it persisting in the deceased, distributed throughout organ systems, accompanied by the exact tissue damage you would predict if you believed Sucharit Bhakdi’s warnings about endothelial cells producing spike protein and triggering immune attack from within.
The mechanism is not complicated once you accept what the biodistribution data already showed.
Lipid nanoparticles do not remain at the injection site. Pfizer’s own Japanese biodistribution study, obtained through freedom of information requests, showed accumulation in the liver, adrenal glands, ovaries, and beyond.
When those nanoparticles reach tissue, cells take up the mRNA, produce spike protein, and display it on their surface. The immune system recognizes it as foreign and attacks. In the heart, that means myocarditis. In vessel walls, that means vascular inflammation. In the brain, that means neurological damage.
Burkhardt’s autopsies are not speculation, they are the physical, histological confirmation of a mechanism that was biologically predictable and institutionally ignored.
In many of these cases, no other plausible cause of death was identified. These were not people with terminal diagnoses or obvious competing explanations. They were people who died in proximity to vaccination, whose deaths were documented, whose tissues were examined by a trained pathologist, and whose organs showed the fingerprints of spike protein-driven inflammation. That is not a coincidence. That is evidence. And health agencies have responded to that evidence by downplaying it, dismissing Burkhardt’s methodology, discouraging thorough post-mortem investigation, and refusing any systematic, government-funded autopsy program that might produce data they cannot control.
They knew the biodistribution data before a single dose was administered to the public. They had Pfizer’s own studies showing the lipid nanoparticles traveled. They authorized anyway. They mandated anyway. They silenced the clinicians and pathologists raising concerns anyway. And now, faced with autopsy findings that document spike protein in the organs of the dead, they respond not with investigation but with institutional silence and the quiet suppression of inconvenient science. That is not a public health apparatus functioning in good faith. That is an apparatus protecting itself.
The dead cannot demand answers. The injured, many of whom carry the same spike-driven inflammatory damage in living tissue, are told their symptoms are unrelated, psychosomatic, or coincidental. Burkhardt’s work, alongside the vascular findings documented by Bhakdi and colleagues, represents a body of post-market evidence that should have triggered immediate regulatory review, mandatory autopsy protocols, and full transparency on biodistribution. Instead it has been buried, not by counter-evidence, not by superior data, but by institutional authority and the refusal to look.
This is what burying evidence looks like. It does not always involve shredded documents or deleted files. Sometimes it looks like a regulatory agency that simply never funds the study, never mandates the autopsy, never convenes the independent panel and then points to the absence of data it refused to generate as proof that there is nothing to find.