There might finally be a way forward for Long COVID treatment, and I will talk about it 🚨
A few months ago, I shared an image: Pain + Context = Suffering and behaviour. 🚨
It got a lot of backlash.
I expected it.
Today Alan Levinovitz’s Long COVID article was published, titled: “There might finally be a way forward for Long COVID treatment; if only you were allowed to talk about it.”
Again, a predictable backlash.
So what I want to do is link Levinovitz’s article with my clincial work, Mark Solms’ recent paper on “function” in functional neurological disorders, and other literature on predictive processing, active inference, and interoceptive dysfunction. All biology.
In addition, I will explain the neuroscience of how the brain reacts to allostasis, shaping a new 'person'.
It's a long post, so I'll break it down into chapters.
Chapter 1: The Image, the Backlash, and the Question
The image and the article can create an almost reflexive judgment about what I am going to say, before I can make an argument.
But before reacting with anger, dismissal, contempt, or the urge to block, pause for a second because that reaction is part of the very mechanism I want to explore.
Ask: What exactly am I reacting to? (You haven't read what I'm about to say; have you made a prediction of what I mean before knowing what I mean? )
Because what I am about to describe is precisely that process.
-How a lower-level bodily signal (arousal, anger, reflex reactions, etc.) becomes a prediction.
-How a prediction becomes a feeling.
-How a feeling becomes a conscious thought.
-How a conscious thought becomes an action.
-And how repeated action becomes a loop.
That loop is NOT “mindset”, willpower, “just think differently”.
It is the brain doing what brains do: predicting, protecting, acting.
So before going further, let me be clear.
This does NOT mean MECFS, Long COVID, FND, or chronic pain are not real.
It does NOT mean symptoms are “all in the head”.
It does NOT mean people should push through.
None of that.
What I am saying is that there is/ may be a way forward, and that way forward requires understanding how the brain organises around pain, fatigue, threat, uncertainty, bodily collapse, and the loss of a previous life.
Chapter 2: From Signal to Action
In medicine, one of the most neglected questions is still this:
How does the brain turn a body signal into an action?
A signal comes in.
Pain. Fatigue. Dizziness. Weakness. Breathlessness. A strange internal sensation.
But the brain does not simply receive the signal.
It asks: (note - The Brain asks; Not you consciously)
-What is this?
-Have I felt this before?
-What happened last time?
-Is this safe?
-What should I do next?
The basic pathway:
Perception → prediction → meaning → threat/safety → attention → action.
Input → prediction → prediction error → updating → conscious thought → action
Chapter 3: The Staircase
Most of this is not conscious. You see stairs.
You do not consciously calculate vestibular input, muscle contraction, joint angle, cardiovascular demand, expected effort and recovery curve.
Your brain predicts:
“I know stairs.” “My legs can do this.” “This cost is manageable.” “I will recover.”
So you climb.
Chapter 4: The Same Staircase After Illness
Now take the same staircase after illness.
--After Long COVID or FND or pain.
-After ME/CFS.
-After repeated PEM.
-After dizziness.
-After pain flares.
-After months, your body no longer behaves like the body you knew.
Now the staircase is not just a staircase.
It is a prediction. (the meaning; easily misinterpreted as thought)
What will this cost?
Will I crash?
Will I recover?
Will this take hours, days, or weeks?
That is the nervous system trying to protect the organism based on prior experience.
Chapter 5: The Solms article
It's likely people look at the word psychoanalysis and immediately filter the article through old memories. which is exactly what Solms argues.
"Memories are about the past, but they are for the future."
Solms revisits the old idea of a “lesion of an idea”, but places it within a modern neurobiological frame.
The point is not that symptoms are imaginary.
The point is that not all pathology is structural in the simple textbook sense.
Some pathology is functional, which is not 'made up' but rather how the brain / CNS organises perception, affect, memory, attention, prediction and action.
Doctors are trained to look for textbook lesions.
-A nerve lesion should follow a nerve.
-A spinal lesion should follow a tract.
-A cortical lesion should follow a map.
But the brain does not only work from our diagrams.
The brain has its OWN IDEA of the body.
And sometimes, after illness, pain, trauma, collapse, autonomic dys, humiliation, medical fear or repeated bodily alarm, the brain develops its own idea of what the body can or cannot safely do.
Not fake.
Not imagined.
A functional model. (brain's model of functions)
Chapter 6: FND, ME/CFS and Long COVID
A patient with FND may consciously want to move their leg.
But the motor system may be operating under a stronger prediction:
“This leg is not available for safe action.”
A patient with ME/CFS may consciously want to walk.
But the system may have learnt:
A patient with Long COVID may desperately want their old life back.
But the body has been 'teaching' the brain:
“Exertion has consequences.”
Chapter 8: Precision: When Prediction Becomes Policy
This is where prediction is so easily misunderstood.
People hear “prediction” and think:
belief, mindset, choice, attitude, willpower, try harder
NO!
The brain has a hierarchy of predictions.
Some become conscious thoughts.
Many never do.
They sit in interoception, autonomic regulation, motor control, salience, memory, arousal, habit and action selection.
A lower-level prediction can rise into conscious experience as:
“I feel unsafe.” “I can’t do this.” “This will make me worse.”
Then it becomes behaviour:
-stopping -lying down -avoiding
-withdrawing
-resting.
Sometimes that action is protective.
Sometimes it is necessary.
But sometimes, over time, the protective response can become a 'trap'.
In predictive processing, the keyword is precision.
Precision means confidence. (it's below thought)
A flexible prediction sounds like:
“Maybe this hurts, but I can test it.”
A high-precision prediction sounds like:
“If I move, I will crash.” “If I stand, I will collapse.” “If I use this leg, it will fail.”
Once a prediction becomes high precision, the brain stops treating it as a question.
It becomes a policy. A habit. An automated protective solution.
That is why “just push through” isn't helpful. Changing your thoughts isn't helpful .
The problem is NOT a lack of effort.
The problem is that the nervous system has assigned too much confidence to a protective prediction.
Chapter 8: The Cost of Effort
This is also why the newer cost-of-effort paper in chronic fatigue is important.
In that study, people with chronic fatigue watched videos of others exercising and estimated how effortful it looked.
They were not exercising themselves.
Yet they predicted higher exertion across effort levels than controls.
More importantly, in the chronic fatigue group, the prediction bias was shaped less by the person in the video and more by the observer’s own fatigue and disability.
Because the system is not only responding to the task. It is responding to what the task is predicted to cost.
Again, not consciously or wilfully.
Not “all in the mind”.
But through a brain-body system that has 'learnt' from experience.
Chapter 9: Why People React
And yes, I understand why people react.
Patients with Long COVID, ME/CFS, FND and chronic pain have been dismissed for years.
They have been told,
“It is anxiety.” “Your tests are normal.” “Just exercise.” “It is stress.” “It is in your head.”
So when words like prediction, meaning, attention, function or brain are used, many understandably hear invalidation.
..and the new neurobiology is filtered through the lens of memories.
But Prediction IS biology.
The mistake is thinking that biology only counts if it appears as a visible lesion, an abnormal blood test, or a scan finding.
Biology also includes:
-interoception
-autonomic state
-salience
-memory
-attention
-arousal
-precision
-motor output
-habit
-action selection
Chapter 10: What I See Clinically
As a clinician who spends months, yes, months, with this same complexity on the ward in a multidisciplinary private setting, with chronic pain, MECFS/ Long covid, FND, this is not abstract to me.
Alan Levinovitz’s article makes an important observation: Kennedy, who had worked in a Long Covid speciality group, felt she had “too little time with patients to form the kind of relationship necessary for this approach.”
Time is a core part of the treatment.
We incorporate the neuroendocrine, ANS, inflammatory, circadian, etc., layers, as well as the biological aspects of interoceptive processing, predictive processing, and active inference.
It is rarely one or the other.
Some patients recover rapidly with a specific biological intervention - medication, sleep, autonomic, inflammatory, endocrine, pain or circadian treatment and return to high-level function.
Others improve symptomatically but stall, because the body is better, but the nervous system has not updated its model: movement still means danger.
Then there is a third group, where years of pain, withdrawal, dismissal and failed treatments shape everything. Doctors, medications, reassurance, physiotherapy, side effects, even recovery, are filtered through the same predictive lens:
"this will harm me, this will fail, if I improve, I will crash, no one believes me, I'm not being heard; I'm trying, and no one sees the effort."
This is why I admit for months. I don't just do second opinions because an opinion without a plan behind it doesn't mean much.
The patterns play out in real time, with me, new clinicians, medications, boundaries, ruptures and repairs. (objects never before encountered)
Therapeutic alliance is crucial.
For some patients, trust takes months because the brain has spent years learning that resistance was protection.
You see the brain organise around real biology.
You see pain become linked to threat.
You see fatigue become linked to cost.
You see dizziness become linked to loss of control.
Avoidance reduces prediction error in the short term, while shrinking the person’s world in the long term.
And you also see change.
Not by saying 'think positively'.
But because the nervous system gradually updates, through a combination of safety, pacing, autonomic regulation, medication, physiotherapy, psychotherapy.
etc
Sometimes, even through supplements or interventions that may not work by the mechanism claimed, but because they provide a new object around which agency can restart.
"Stranger still are patients’ stories of astonishing recoveries from severe long Covid, achieved entirely outside mainstream medicine." (Levinovitz)
The common factor is often something (often multiple things) that allows the system to reduce prediction error and test a new action.
Maybe something has changed. Maybe I can try. Maybe this body can act again.
Chapter 11: The Clinical Question
The clincial question needs an additional question.
Not Where is the lesion? Or what are the mechanisms, BUT also
What has the nervous system reorganised around?
Because sometimes the lesion is not where the textbook tells you to look.
Sometimes it is visible in the function:
what the brain predicts, attends to, avoids, automates, and what action it no longer permits.
If you want to keep the prediction that biology only means visible numbers and visible lesions, that is okay.
But at least allow others to learn the broader biology.
Because the invisible CAN be made visible when you learn what to look for.
@AlanLevinovitz
Good question. Answer - The Brain X Environment Mismatch 🚨
This is where an evolutionary perspective helps. 👇
Cognition, emotion, activity and arousal interact with the environment.
-Cognition evolved to facilitate movement
-E-motion ( the word gives it way) - To MOVE out - also to facilitate movement
The balance of activity , cognition and emotion (ACE) has shifted in the modern environment
Example: the Ariaal tribe.
Eisenberg et al. found that men with the DRD4 novelty-seeking allele living nomadically were better nourished.
( also a allele linked to ADHD )
The same allele in a settled context was associated with poorer nourishment.
So I’d reframe the question as
“What environments made certain brains adaptive and what environments now make them struggle?”
Modern life is a sustained test of:
• sitting still • delayed reward • sleep disruption • low movement • high novelty • digital salience ‘traps’ • constant cognitive switching
A trait is not ‘good’ or ‘bad’ in isolation.
It depends on the environment asking something of it.
The load has shifted.
Historically, survival was distributed across the body, activity, emotion, community and immediate action.
Modern life places a heavier burden on cognition and self-regulation.
Different environment.
Different consequences.
Same brain.
That is the mismatch.
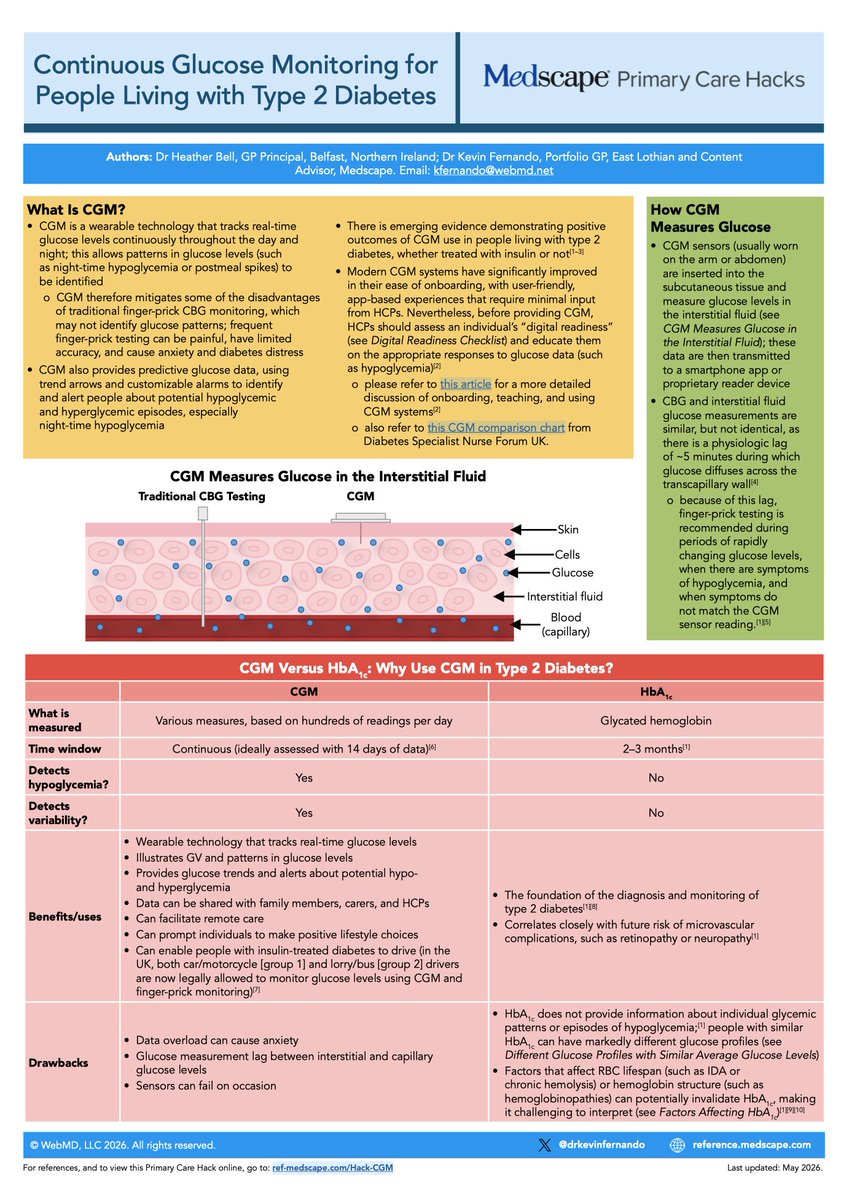
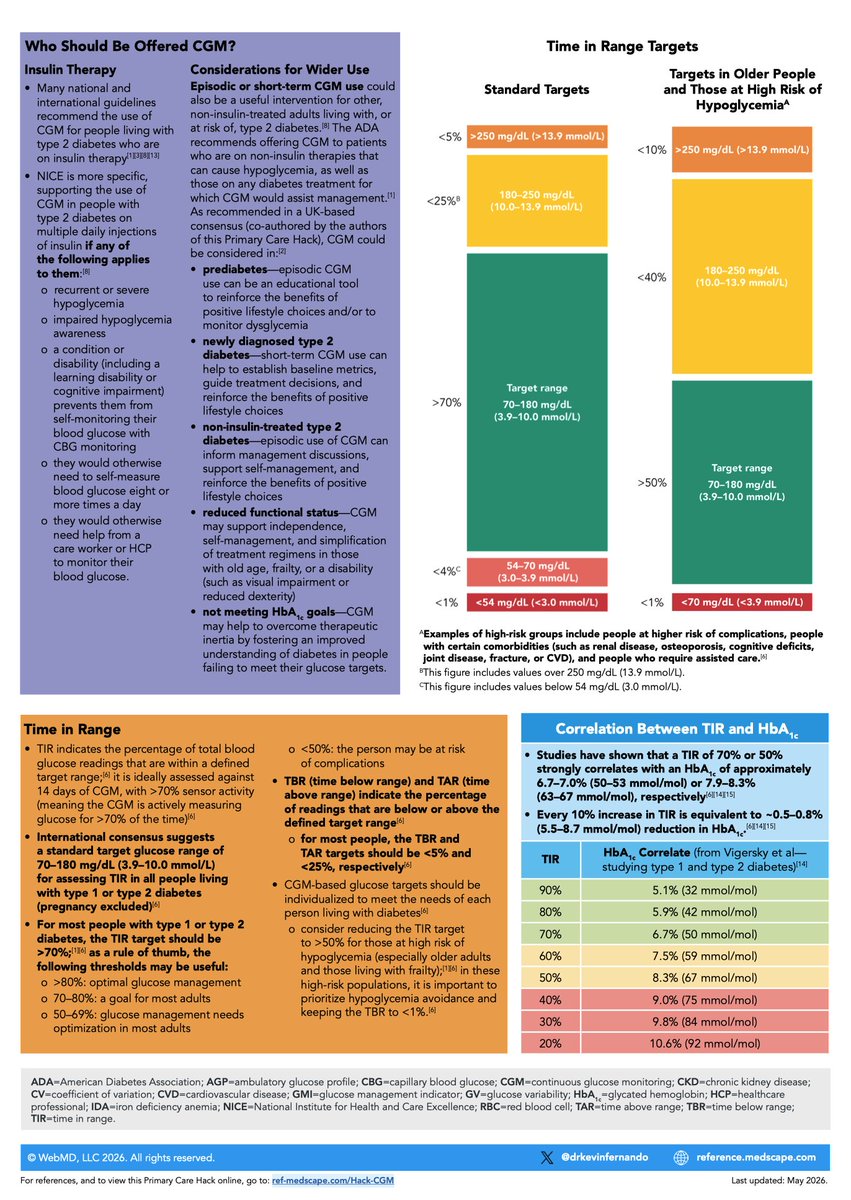
🔥My latest Medscape Primary Care #Hack is live!
💡Continuous Glucose Monitoring #CGM for people living with #T2D
Co-authored with @drheatherbell
Includes 8 simple steps to interpreting the Ambulatory Glucose Profile report #AGP
PDF download link in comments 👇
@DudeAdhd@LuxMeaMundiAM Try not to worry too much, it sounds like you have everything that's needed and just need to go through the process. The form is long but you have enough information to fill it out.
Anxiety disorders are highly prevalent. Despite having well established first-line treatments, only 25% of affected people globally receive them.
Improved access, therapist training, and ongoing innovation are necessary pillars for effective clinical care
https://t.co/u6jWAyH4W7
Who responds best to stimulants in adults with ADHD? 🚨
Predictors of positive response 👇
1/ Worse task monitoring and working memory predicted better stimulant response
2/ Greater overall executive impairment on BRIEF predicted better outcomes
3/ Better quality of life predicted higher odds of response
Predictors of poor response : 👇
1 / Higher thought problems
2/ withdrawn traits
3/ internalising symptoms
4/ intrusive thoughts
Clinical implication:👇
Patients with more obvious fronto-striatal executive dysfunction may have more room to improve with stimulants, whereas internalising symptoms, social withdrawal, or ASD like traits may signal a weaker response or a more complex picture.
🩺 SGLT2i + high HbA1c = higher DKA risk?
New meta-analysis (22 studies, 1.3M patients):
🔹 HbA1c ≥67 mmol/mol (8.3%): DKA risk RR 1.63
🔸 HbA1c <67 mmol/mol: No significant increase (RR 1.10)
🔹 Significant effect modification (p=0.018)
Practical approach when HbA1c is very high:
🔸 Rescue therapy first (SU or insulin) to bring glucose down
🔹 Add SGLT2i for CV/renal protection once stabilised 🔸 Deprescribe rescue agent
Don't avoid SGLT2i. But consider "stabilise then protect" when starting from HbA1c >75 mmol/mol (9.0%).
Sick-day rules essential either way.
🔗 https://t.co/FT78pe9vNC
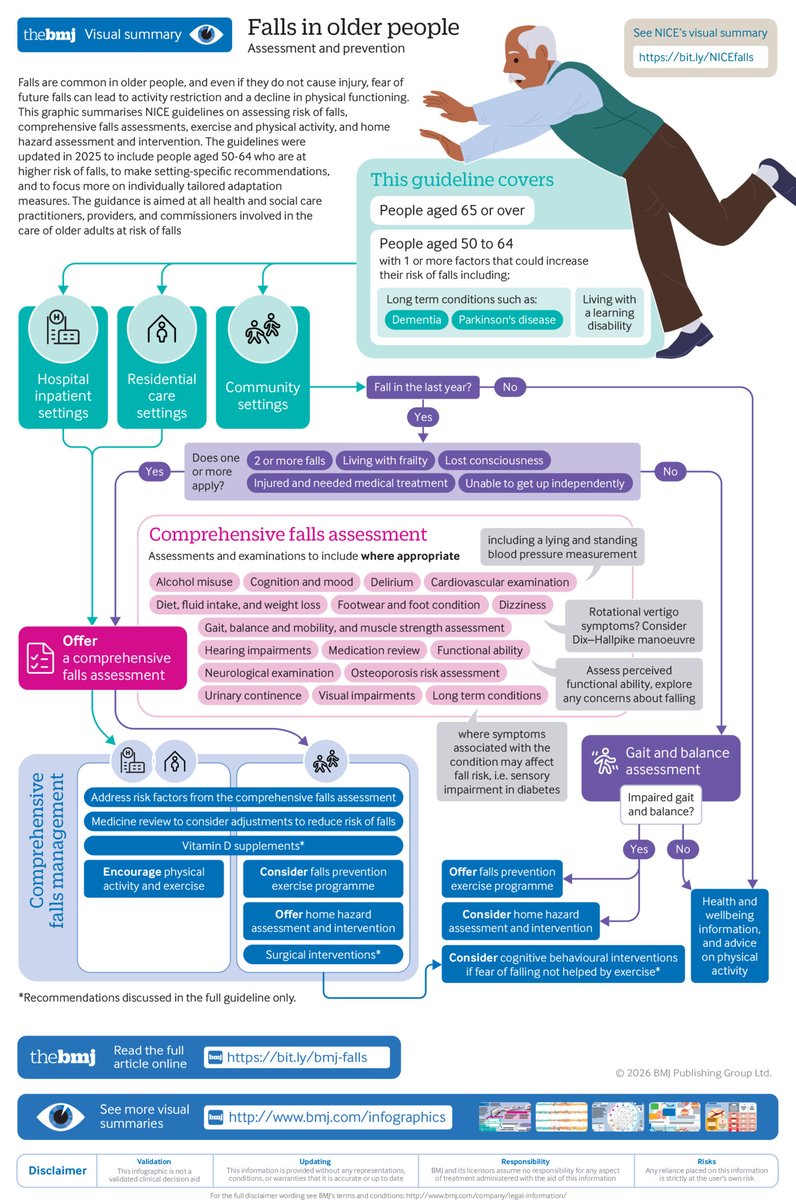
Falls are common in older people, and fall related injuries are a substantial cause of morbidity and mortality.
How should doctors assess the risk of falls? A summary of NICE guidelines, including a #BMJInfographic
https://t.co/s3P7sATuvU
Let's gather the evidence the Government needs to take action!
We’re working with a neurodiverse team of researchers to develop a survey for anybody who’s asked for an autism or ADHD assessment - adults or children - in the last six years.
The survey will ask about reasons for requesting an assessment and experiences while waiting.
The more people who complete the survey, the more powerful the evidence wll be, and the stronger the case for Government to act.
Please share this with anybody likely to be interested, including organisations and professionals who provide assessments - because they can share with many more people.
Visit https://t.co/vp7p6JVhZp to register your interest and hear when the survey is ready.
#autismassessment #adhdassessment #autism #adhd
ADHD vs RSD? Same Circuit , Different Label🚨
This is where labels can start creating more confusion than clarity.
RSD is not a diagnosis. ❌
It is better understood as a phenomenon.✅
So rather than getting stuck on the label, ask:
What is actually happening in the brain? 👇
What people call RSD is fundamentally an intense emotional response to a specific interpersonal stimulus, usually perceived rejection, criticism, or disapproval.
A key aspect is it is relational.
The brain detects social threat.
The amygdala reacts strongly.
And when this happens repeatedly over time, that response can become sensitised.
So each new rejection, criticism, exclusion, or even subtle interpersonal shift can feel disproportionately intense.
In that sense, RSD is often the cognitive label given to a real affective process.
Now bring in ADHD.
ADHD is not just about attention.
It also involves fronto-striato-limbic circuits.
That means ADHD can affect:
-attention -salience assignment -impulse control -emotional regulation -frustration tolerance -response to interpersonal stress
This is why emotional dysregulation is such an important part of ADHD, especially when ADHD is understood through an arousal-regulation model.
So when someone with ADHD appears highly sensitive to rejection, criticism, or perceived failure, that does not automatically mean there is a separate entity that needs to be split off as something entirely different.
Often, it reflects the same broader neurodevelopmental system:
-heightened limbic reactivity -reduced top-down modulation -difficulty regulating the emotional significance of a stimulus once it is tagged as threatening
That is why ADHD and so-called RSD overlap so strongly.
The takeaway?
-RSD is a phenomenon. -ADHD is the broader neurodevelopmental condition.
And if you want to help the person, the task is not just to name the phenomenon.
It is to ask:
👉How do we reduce amygdala overactivation? 👉How do we strengthen top-down control? 👉How do we improve regulation using biological, psychological, and social strategies?
Because in the end, treatment is about understanding the mechanism in the person sitting in front of you.
New video on Sleep Supplements 🚨
I cover the 3-system understanding of sleep arousal, movement, and circadian timing and how supplements can be used more effectively when matched to the underlying sleep problem.
https://t.co/7EcpQ3SIbb
the proportion of NHS spending going to mental health will fall again next year, dropping to 8.4% of the total NHS budget...'
... the third year in a row that mental health’s share has slipped.
https://t.co/M7Lu3Ebmrd
@DudeAdhd The assessment we experienced for my adult child for low capability for work was good, it involved a lengthy form tho. Once on lcw there isn't a requirement for job centre meetings. Depends on the outcome as to what contact is required going forward.