🔍 10% Visceral Fat loss⤵️ T2D cases by 28% over 10y
5- and 10-yr follow-up of two 18-mo lifestyle RCTs. The story isn’t the weight loss. It’s what stayed lost after the weight came back:
🔹 VAT -27% at 18 mo (MRI)
🔸 5–10 yr later: weight fully regained. VAT still ~15% below baseline (~55–60% of original loss preserved)
🔹 Each 10% VAT loss = 28% lower T2D risk in follow-up (HR 0.72). Association, not proof
🔸 Liver and pancreatic fat fully regained
Track waist, not just weight.
🔗 https://t.co/Hp8C0gHJxw
The attempts of the @RCPhysicians to cling on to the vestiges of what they once supported is quite ...amazing
The requirements to be... Certificate in Geriatric Medicine Knowledge-Based Assessment Lead includes being a PA for 7 years.
I predict this is a degree anyone can do and be equated to specialist training in near future too.
@GeriSoc - are you saying a Consultant of 3 years experience and a PA of 7 years experience are at par?
Cos that's....something
Link:
https://t.co/67tFEl2NXM
To be honest there are a lot of unknowns about this. In terms of diabetic retinopathy the postulated theory remain rapid drop in glucose exacerbation the retinopathy. Although they are GLP-1 receptors within the retina.
In terms of normal glucose in an obese population without T2D less is known and particularly in non diabetic retinopathy. Other than what you have seen
Age of diagnosis; #T1Diabetes#T2Diabetes & science
“Clinicians should be aware that patients progressing to #insulin within 3 years of diagnosis have a high likelihood of #type1diabetes, regardless of initial diagnosis”
Via @DiabetologiaJnl
Please use, RT as possible
Link:
https://t.co/Qg6yf0L98y
The opportunity this provides and potential is there… if science builds further and regulation/policy/funding allows… hopefully will go the way of tech all those years ago …. Would like to get to a point to say the next 5 years is about cementing and implementing immunotherapy in T1D… not there yet though…
¿Cuándo elegir semaglutida y cuándo tirzepatida?
La EASO acaba de actualizar su algoritmo con evidencia hasta noviembre 2025 📊 @EASOobesity
Spoiler: depende del objetivo clínico. No es solo pérdida de peso.
🔗 @NatureMedicine
https://t.co/RKkccNGYTq
#ECO2026
Interesting data from #ECO2026@EASOobesity
Building on the need for more data in women’s health esp around menopause but more interesting is the migraine data
Expanding the other potential beneficial effects of weight loss and why there are also trials in IIH with incretins
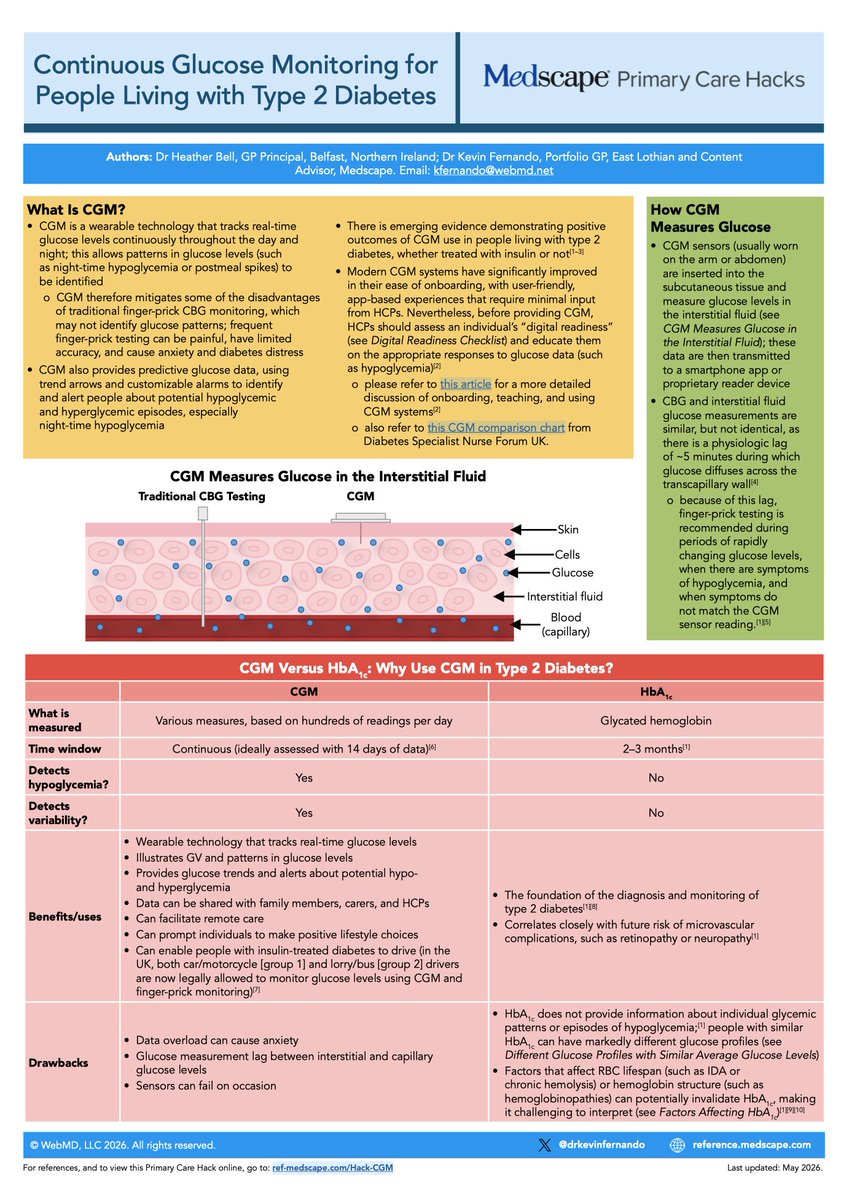
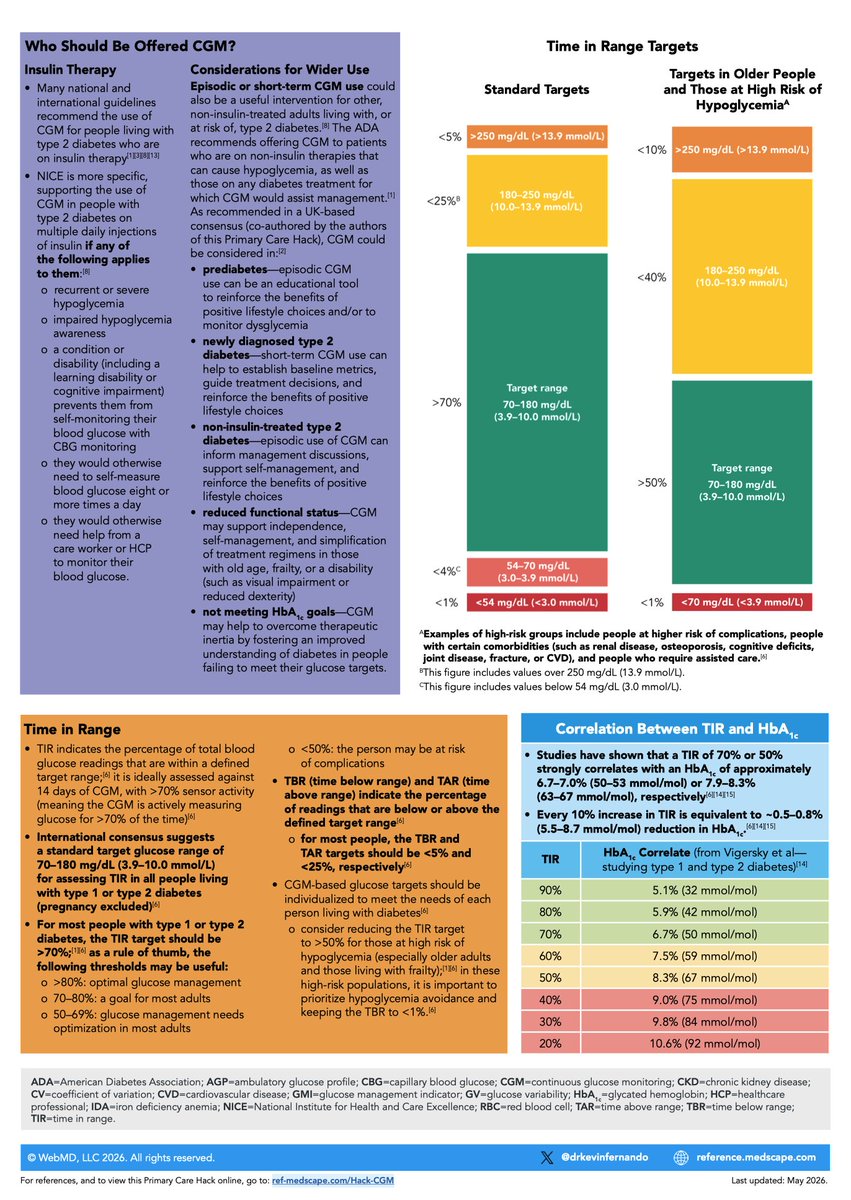
🔥My latest Medscape Primary Care #Hack is live!
💡Continuous Glucose Monitoring #CGM for people living with #T2D
Co-authored with @drheatherbell
Includes 8 simple steps to interpreting the Ambulatory Glucose Profile report #AGP
PDF download link in comments 👇
Don’t miss the signs of #T1Diabetes
The 4 Ts
And no, they don’t have to be altogether as a presentation
Keep this in your mind as a possible diagnosis
Even one life saved?
Is worth all the “cost”
Better safe than sorry
#T1Diabetes 💙
So folks: this means that if you have obesity…. You are 38% less likely to die if you have bariatric surgery - there are no studies for GLP-1ra that show these dramatic results.
🚨NICE TA1152: #semaglutide 2.4 mg recommended as an option for ⤵️💔risk in adults with established CVD and BMI ≥27 kg/m² 🚨
🔹 Eligible: previous MI, ischaemic/haemorrhagic stroke, or symptomatic PAD, with BMI ≥27. No restriction on time since index event. T2D not excluded.
🔸 SELECT (n=17,604): First MACE: HR 0.80 (0.72-0.90) Non-fatal MI: HR 0.72 (0.61-0.85) Coronary revasc: HR 0.77 (0.68-0.87) All-cause death: HR 0.81 (0.71-0.93) Benefit appeared early, before substantial weight loss.
🔹 Preferred ICERs £6,878 to £14,594 per QALY, well below the £20,000 threshold.
🔸 What a TA means for access: statutory funding mandate. ICBs in England must make it available within 90 days when considered the right treatment (Wales: 60 days from final draft). But that doesn't mean immediate primary care prescribing.
🔗 https://t.co/WRVJ0F8gOB
#PrimaryCare #Cardiology #GLP1 #NICE