The first question was:
Why is teclistamab so active after ASCT?
The second question is:
Why do some patients remain MRD negative while others relapse?
Perhaps the answer is not deeper response.
Perhaps the answer is restoration of durable immune surveillance.
🧬 In Biology We Trust
#MultipleMyeloma
MajesTEC-4 was the most fascinating study reported at EHA 2026 for me.
Not because 100% MRD negativity (10⁻⁵) was achieved.
What truly caught my attention was the magnitude and speed of CR/sCR conversion.
After ASCT, CR/sCR rates were approximately 25-40%.
Within 6-12 months of Tec-based maintenance, CR/sCR approached 100%.
That is breathtaking.
MASTER, CASSIOPEIA, and PERSEUS established an extraordinarily high bar. MajesTEC-4 is now challenging those landmark studies despite being an early run-in cohort of ~90 patients.
The deeper question is not whether teclistamab is active.
We already know it is.
The question is why it appears so active in the post-ASCT setting.
Where do the effector T cells come from?
Are they predominantly reinfused with the autograft?
Do the classic Mayo observations linking early lymphocyte recovery to superior outcomes offer a clue?
Perhaps ASCT is doing more than cytoreduction.
Perhaps maintenance is doing more than maintaining.
Step by step.
Trial by trial.
Not only are responses becoming deeper.
More patients are achieving them, and they are achieving them faster.
#EHA26 #MultipleMyeloma #ASCT #MRD #Myeloma
Based on a recent slew of RCTs & updates at #ASCO26 and #EHA26 in relapsed #MultipleMyeloma, here is my framework for approaching 1st relapse (assuming access to all of these regimens in patients with ≥1 prior LoT). Its an exciting time in myeloma, with a rapidly changing treatment landscape!
WHY DOES SCALP COOLING WORK FOR TAXANES — BUT NOT FOR T-DXd?
The answer may be simple: it's a problem of exposure time.
✅ Taxanes → brief exposure → scalp cooling overlaps drug delivery → hair preservation is often possible.
⚠️ Anthracyclines → greater follicular toxicity → protection becomes less effective.
❌ T-DXd → DXd payload exposure may persist for ~5–6 days, while scalp cooling lasts only hours.
An umbrella can stop a storm.
It cannot stop a week of rain.
A biologic explanation for why scalp cooling appears most effective with taxanes, less effective with anthracyclines, and has not shown proven benefit with T-DXd.
#BreastCancer #ScalpCooling #TDXd #TrastuzumabDeruxtecan #Taxanes #Oncology #MedTwitter #OncTwitter #MVOnco
What did ASCO 2026 change?
Some standards of care have now moved by years.
That almost never happens.
BRAF colorectal, pancreatic KRAS, and DDLPS sarcoma
are three of oncology's hardest diseases
SOC moved by > 1yr:
▫️BRAF mCRC: 15.1 → 30.3 months OS
▪️Pancreatic KRAS: 6.7 → 13.2 months OS 🏆
▪️DDLPS sarcoma: 1.5 → 9.7 months PFS ⭐️
(sarcoma went from "nothing" to a win).
Myeloma, GIST, HR+/HER2- breast, uveal melanoma, bladder, prostate, and RET+ lung cancer moved too.
This is what decades of funded science look like when it compounds.
- - - - -
Source: Jori (@jori_health)
𝘗𝘭𝘰𝘵 𝘱𝘦𝘦𝘳-𝘳𝘦𝘷𝘪𝘦𝘸𝘦𝘥 𝘣𝘺 𝘦𝘪𝘨𝘩𝘵 𝘰𝘯𝘤𝘰𝘭𝘰𝘨𝘺 𝘦𝘹𝘱𝘦𝘳𝘵𝘴. 𝘛𝘩𝘢𝘯𝘬 𝘺𝘰𝘶 <3
- - - - -
HER2-low TNBC may be entering the ADC + IO era.
BEGONIA arm 6 tested 1L durvalumab + T-DXd in HR-negative, HER2-low metastatic breast cancer.
👩⚕️ n=58
🧬 Mostly PD-L1 negative
🎯 ORR: 62.1%
⏳ mPFS: 12.6 months
🧭 mOS: 30.3 months
But the signal comes with a warning:
ILD/pneumonitis: 20.7%
Grade 5 ILD: 1.7%
My take:
Promising efficacy, especially in a difficult biology, but this is still phase 1b/2, single-arm, small n, and missed its protocol-defined ORR target.
ADC + IO is exciting.
But toxicity monitoring will decide how far this strategy can go.
🔖 Save this for breast oncology updates.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #BreastCancer #TNBC @OncoAlert@myesmo@esmo_open
Unfortunate to see no benefit with 1L giredestrant/palbo (vs AI/palbo) in persevERA — despite a signal for patients with more indolent disease features. The benefit of oral SERDs in metastatic disease remains mostly anchored to ESR1 mutations.
BCMA targeting continues to evolve. ⚔️🧬
We recently reviewed the MajesTEC universe.
TODAY let’s focus on the DREAMM program and the long, unusual journey of Blenrep (belantamab mafodotin).
From:
🧪 DREAMM-1 proof of concept
➡️ DREAMM-2 accelerated approval
➡️ DREAMM-3 withdrawal setback
➡️ DREAMM-7 comeback story
➡️ DREAMM-8/9 expansion into earlier disease
Important reminder:
A powerful target does not disappear because one strategy struggles.
BCMA has now validated itself across:
⚡ CAR-T
⚡ Bispecifics
⚡ ADCs
The platform changes.
The biology survives.
And perhaps the most important teaching pearl:
Not all relapsed myeloma is biologically equivalent.
DREAMM-7 and DREAMM-8 likely studied very different immune battlefields despite both being “relapsed MM.”
🧠 Triple refractory ≠ biologically homogeneous disease.
Dr Fun + G
#MultipleMyeloma #Hemetwitter
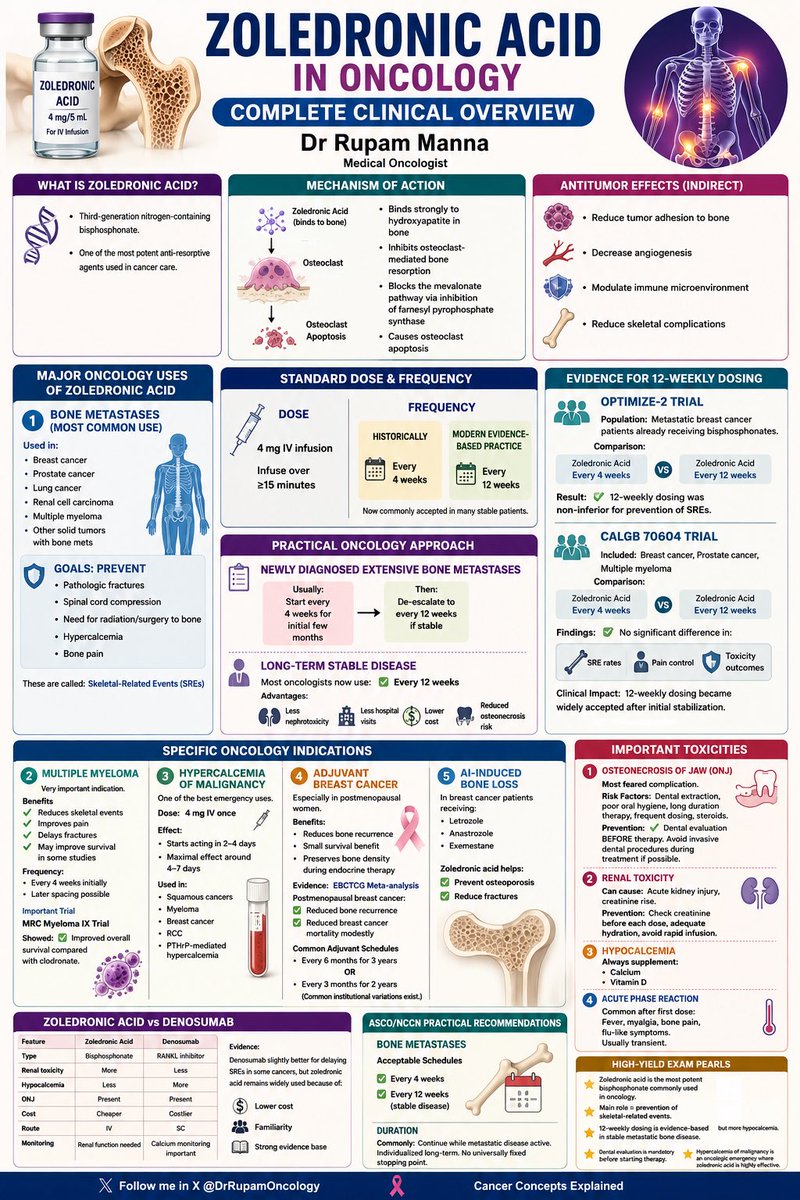
🦴 ZOLEDRONIC ACID in Oncology: Your COMPLETE 2026 Clinical Mastery Guide!
One of the most potent anti-resorptive agents in cancer care — now with evidence-based 12-weekly dosing that’s transforming practice!
🔥 Why this matters:
• Non-inferior to every-4-weeks for SRE prevention (OPTIMIZE-2 + CALGB 70604 trials)
• De-escalate after initial 3–4 months in stable bone mets → 75% fewer infusions, lower ONJ/renal risk & huge cost savings
• Still the go-to in resource-limited settings (superior cost-effectiveness vs Denosumab per 2026 meta-analyses)
• Proven in bone mets (breast/prostate/lung/RCC/MM), hypercalcemia of malignancy, adjuvant postmenopausal breast cancer & AI-induced bone loss
Plus full toxicity pearls, ZA vs Denosumab head-to-head, NCCN/ASCO-aligned practical approach & high-yield exam tips!
Designed for busy oncologists & trainees by @DrRupamOncology
📌 Save this infographic — you’ll use it weekly!
Tag a colleague who needs this 👇
Follow for more visual oncology gems!
#Oncology #MedEd #BoneMetastases #ZoledronicAcid #CancerCare #SREPrevention #FOAMed
💉 Game-changer for HER2+ Breast Cancer patients!
PHESGO = First fixed-dose subcutaneous combo of Pertuzumab + Trastuzumab + Hyaluronidase.
→ From 2–5 hours of IV infusion to just ~5–8 minutes injection!
✅ Non-inferior efficacy & safety (FeDeriCa trial)
✅ >80% patients prefer it over IV (PHranceSCa trial)
✅ Less hospital time, less fatigue, more convenience
A true landmark in patient-friendly oncology — especially valuable in the COVID era and beyond.
Full infographic breakdown by Medical Oncologist Dr. Rupam Manna 👇
#PHESGO #HER2BreastCancer #BreastCancer #Oncology #CancerCare #PatientCenteredCare
Follow @DrRupamOncology for more clear, evidence-based oncology education!
PFS is not always OS.
One of the biggest misconceptions in oncology is assuming that delaying progression automatically means patients live longer.
Many strategies consistently improve:
• PFS
• depth of response
• MRD negativity
…but OS often barely moves.
Examples:
• Upfront vs delayed AutoSCT
• Lenalidomide maintenance
• HD melphalan intensification
• Many maintenance strategies in lymphoma
Why?
Because:
• crossover therapies matter
• salvage therapies work
• toxicity matters
• resistant clones survive
• biology evolves
A longer remission is meaningful.
But it is not always a longer life.
The critical question is no longer:
“Did the curve separate?”
The question is:
“What happened to OS?”
#MultipleMyeloma #lymphoma #CART #Hemtwitter
Dr. Fun + G
🚨 STAMPEDE Trial Summary – One of the largest & most practice-changing platform trials in prostate cancer history!
Multi-arm, multi-stage (MAMS), adaptive design that transformed mHSPC management forever.
From ADT alone → upfront intensification with:
✅ Docetaxel
✅ Abiraterone
✅ Prostate RT (low-volume mets)
✅ Enzalutamide
✅ Triplet therapy
All major arms, landmark OS/FFS results, clinical pearls & exam-ready quick summary in ONE high-yield infographic by @DrRupamOncology 👏
Essential for oncologists, urologists, DM/DrNB candidates & daily practice. Save, share & tag a colleague!
How has STAMPEDE changed your frontline approach in metastatic hormone-sensitive prostate cancer?
#STAMPEDE #ProstateCancer #mHSPC #UroOncology #Oncology #MedEd #CancerResearch #CancerConceptsExplained
SERENA-6 Surveillance Data: ESR1 mutations emerge in 42% of patients on AI + CDK4/6i.
One test is not enough — serial ctDNA monitoring is essential.
Early detection → timely switch to camizestrant before progression.
Bidard et al. • SERENA-6
#BreastCancer#ESR1#ctDNA #PrecisionOncology #MVOnco #SERENA6