I replaced my financial advisor with Claude - and no, that's not clickbait.
Claude now operates as my personal CFO - and it's the best thing I've done for my finances in years.
It's trained like a McKinsey-level analyst, using all my financial data.
Steal the full setup:
A backtable illustration of a couple techniques you can use if the #Rotaburr gets stuck,
1-The skipping rope technique.
We have known it for a couple years, and it was recently published
https://t.co/fqTn6NXkaT
2-The final resort of cutting the rota driveshaft and advance a guideliner through it to get more leverage to pull.
Of course the first thing you do is to pull hard and maybe try to balloon around it, but those can help with tougher situations.
#CardioX community, please share your additional tips and comments
Here is my algorithm:
1) Vasodilator therapy (if hemodynamic allow and pull)
2) Pull Rotawire. This works very effectively, 90% of times. It is frequently overlooked. The 0.014 tip works as a great way to bring back the stuck burr. Make sure wire is free with brake off for maximal efficiency. Pulling the driveshaft is less effective, as it is made of 3 coiled wires which gives some elasticity to the driveshaft.
3) If burr is free beyond lesion, can use short dynaglide runs and then pull. Prinicple is that dynamic friction is lower. Don’t overdo this and also with skipping rope technique, there is risk of driveshaft breakage and burr loss due to torsional forces with a fix s immobile burr!
4) Cut driveshaft and remove teflon sheath
5) Deliver GE over driveshaft to the burr and pull.
6) Intimal/subintimal wire and ballooning to dislodge burr and pull.
7) Re-deliver GE over driveshaft and pull.
8) Obtain second access and adding a ping-pong guide. Remember a ping-pong guide is not required in most cases. Once Teflon sheath is removed, a 6F guide can accommodate: Driveshaft + coronary wire, Driveshaft + Caravel microcatheter, Driveshaft + Corsair/Turnpike LP microcatheters, Driveshaft + 2.5-4mm balloons
9) Combine subintimal ballooning and GE over driveshaft and pull. Only these maneuvers requires ping-pong guides.
10) Call surgeons.
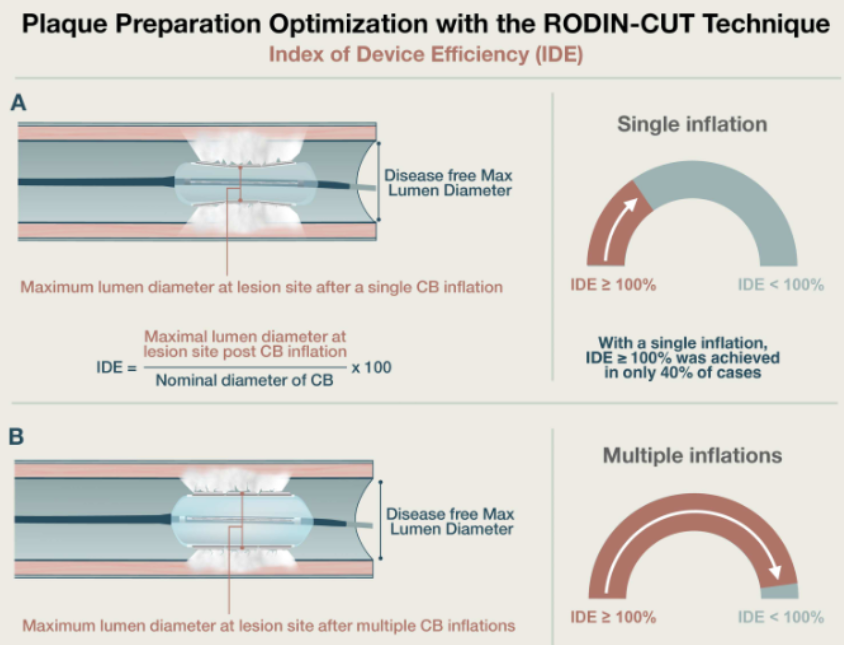
Welcome to the Index of Device Efficiency (IDE), a novel IVUS-derived metric quantifying the mechanical efficiency of cutting balloon angioplasty https://t.co/GDJ01Hmjaw @ccijournal
Presented at #ACC26:
Among patients with infrainguinal artery disease who were undergoing angioplasty, the risk of major adverse limb events at 1 year was lower with sirolimus-coated balloons than with uncoated balloons, and mortality was similar. Full phase 3 SirPAD trial results: https://t.co/q0me2qDhtj
Editorial: Sirolimus-Eluting Technology for the Treatment of Peripheral Artery Disease https://t.co/OIyR2PAKgo
@ACCinTouch
#ACC26 What an incredibly challenging RCT. ORBITA CTO. Simple question with amazing blinding and patient reported angina frequency based on app (much better than recall). CTO PCI DOES improve angina much more than meds in JCTO 3 or less.
Dr. Deepak Bhatt and Dr. C. Michael Gibson discuss the MOMENTUM study: Among U.S. patients with resistant HTN, 27.3% were found to have endogenous hypercortisolism, a significantly higher prevalence than previously recognized. #ACC26 Watch video here: https://t.co/v9ojWxUmYR
#MATCH
Interesting data in Cardiology:
General Cardiology: 292 programs filled (100%), 1,377 positions filled (100%)
Interventional Cardiology: 104 programs filled (68%), 236 position filled (76.9%)
I am surprised by the amount of programs unfilled in IC. Is it lack of interest or learning curve (first years) with the Match?
#CardioX #Cardiology
Thanks to JACC Case Reports for publishing our paper on Real-Time IVUS Guided (RTIG) Ostial Stenting: A Step-by-Step Guide.
5 years of work from benchtop models, microCTs to a now standard part of our practice. Hope someone finds it helpful!
https://t.co/1C1krUklzp
SELUTION DeNovo met its primary endpoint of noninferiority at 1 year, with “only” 20% of DES required as bailout in the drug-coated balloon arm. Imaging use was limited in both groups, while specialty balloons were more frequently employed in the DCB+DES arm (though not dramatically so)—a consequence of randomization occurring before predilatation. There was applause in the room, but the full publication is still pending, so caution is warranted. This is particularly true since analyses were reported as intention-to-treat, which in a noninferiority trial does not tell the whole story (it would be important to see the as-treated and per-protocol analyses), and because some statistical interactions were not immediately clear and somewhat counterintuitive. In any case, an absolute difference of 0.9% between the two arms appears acceptable at 1 year, especially if noninferiority is maintained at 5 years and a benefit emerges consistent with the expected advantages of leave-nothing-behind strategies. #TCT2025
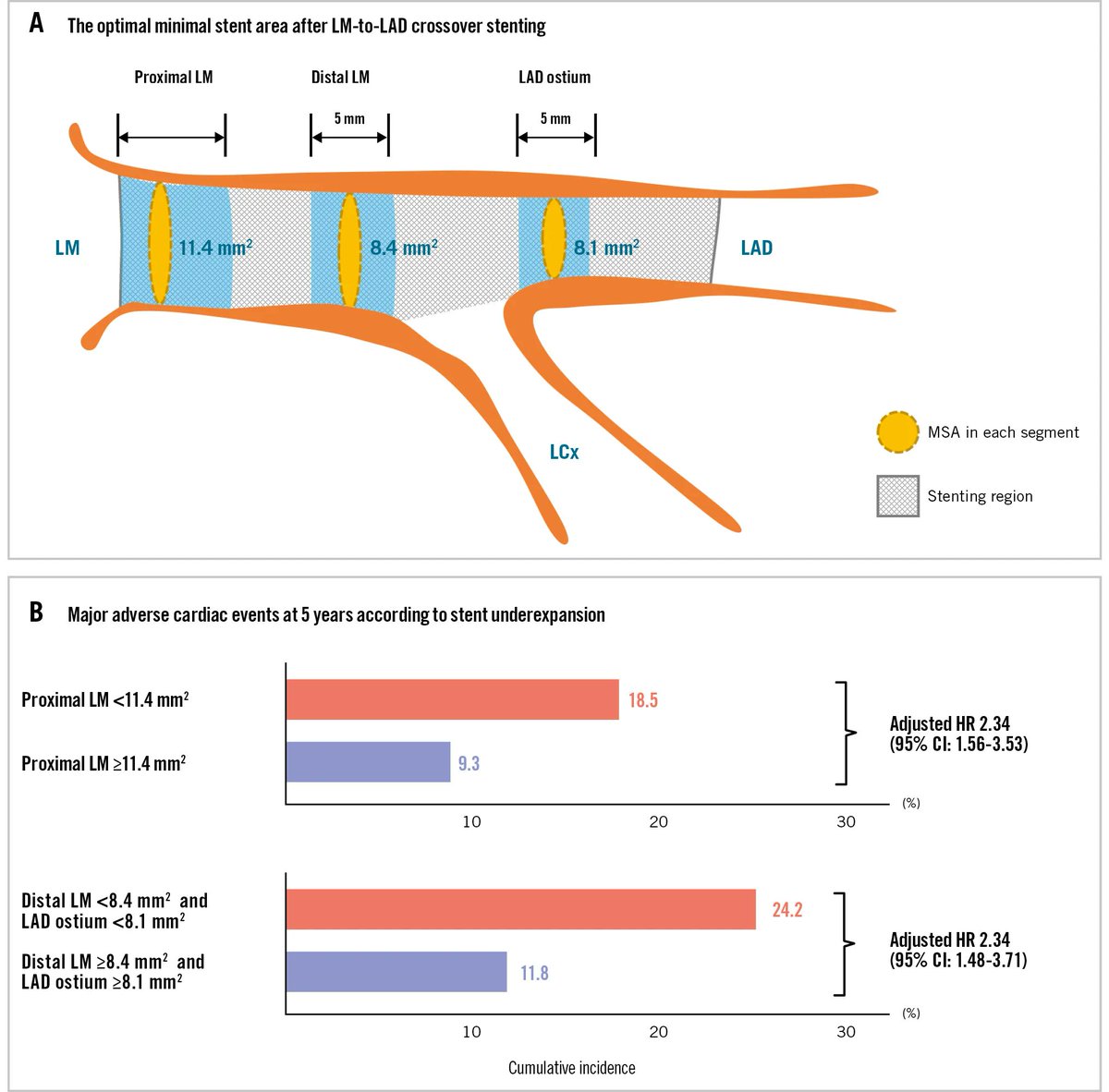
A new research study redefined optimal IVUS minimal stent area (MSA) thresholds for single-stent crossover in unprotected left main disease: proximal left main ≥11.4 mm², distal left main ≥8.4 mm², and left anterior descending ostium ≥8.1 mm². https://t.co/RQz3qdDlJr
Do you want to learn more about INOCA/ANOCA?😃
INOCA International have been working quietly behind the scenes with the NHS and are delighted to launch 10 specially recorded videos on INOCA and ANOCA for Health Care Professionals!
Have you seen them yet? QR code in video 😃👍
🚀 Ready to master drug-coated balloons? Our first webinar in the #Coronary DCB series is tomorrow! Join us for an expert-led, interactive training on treating in-stent #Restenosis to learn practical skills you can use in the #CathLab.🔑
Register now➡️ https://t.co/dEoqLlYzv1
❤️ Heart attack is the leading cause of #cardiogenicshock —help patients recognize symptoms early with https://t.co/KY1Zlyzpqo resources and join us in Tampa for 2025 #SCAISHOCK to advance best practices in cardiogenic shock care.
Register today➡️ https://t.co/fuFqUFkIyM
#CardioEd #CardioX
.@CMSGov has released the proposed 2026 Medicare Physician Fee Schedule. #ACCAdvocacy has outlined key provisions including a new Ambulatory Specialty Model, a 2.5% efficiency adjustment, changes to PCI and LAAO codes, and more.
Get the details ➡️ https://t.co/2iwn6D4hta
Excited to share two advances that bring us closer to real-world impact in healthcare AI:
SDBench introduces a new benchmark that transforms 304 NEJM cases into interactive diagnostic simulations. AI must ask questions, order tests, and weigh costs, mirroring the complexity of real clinical decision-making.
MAI-DxO is a model-agnostic orchestrator that simulates a panel of virtual physicians. It achieves 85.5% diagnostic accuracy—four times that of experienced doctors—while cutting diagnostic costs.
Together, these advances offer a blueprint for how AI can help deliver precision and efficiency in healthcare, and we're looking forward to working with healthcare partners and the entire ecosystem on these advances making a difference.
https://t.co/XHpb1gWYxN
Efficacy of Direct Injection in Occlusive Lesion (DIOL) Fashion for Infrapopliteal and Inframalleolar Chronic Total Occlusions - Haraguchi - Catheterization and Cardiovascular Interventions - Wiley Online Library https://t.co/RnaJvzPMmM
#CTO#HDR#DIOL@dr_peripheral
This is one of HDR techniques for EVT #CTO.
@MauroCarlino3@realarainmd