A decel zone unmasked with S2 (circled). Conversion of PMVT with RF at sites 1,2 to MMVT and non Inducibility with RF at site 3.
#ablateVT#abbottcardio@slate11p
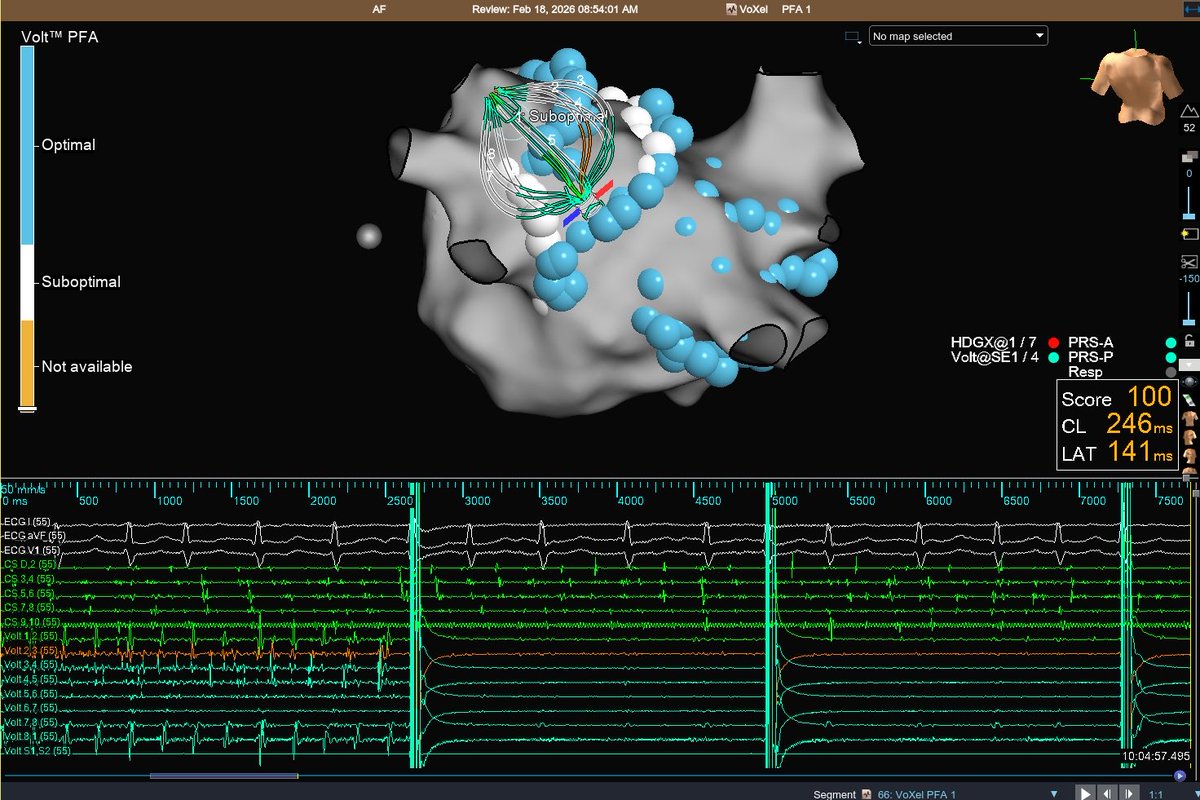
Focal (automatic) atrial tachycardia from the crista terminalis beautifully mapped on Voxel mode with Grid X. 42 msec pre-P and uni QS with no phrenic capture. Would you RF or PFA? #EPeeps
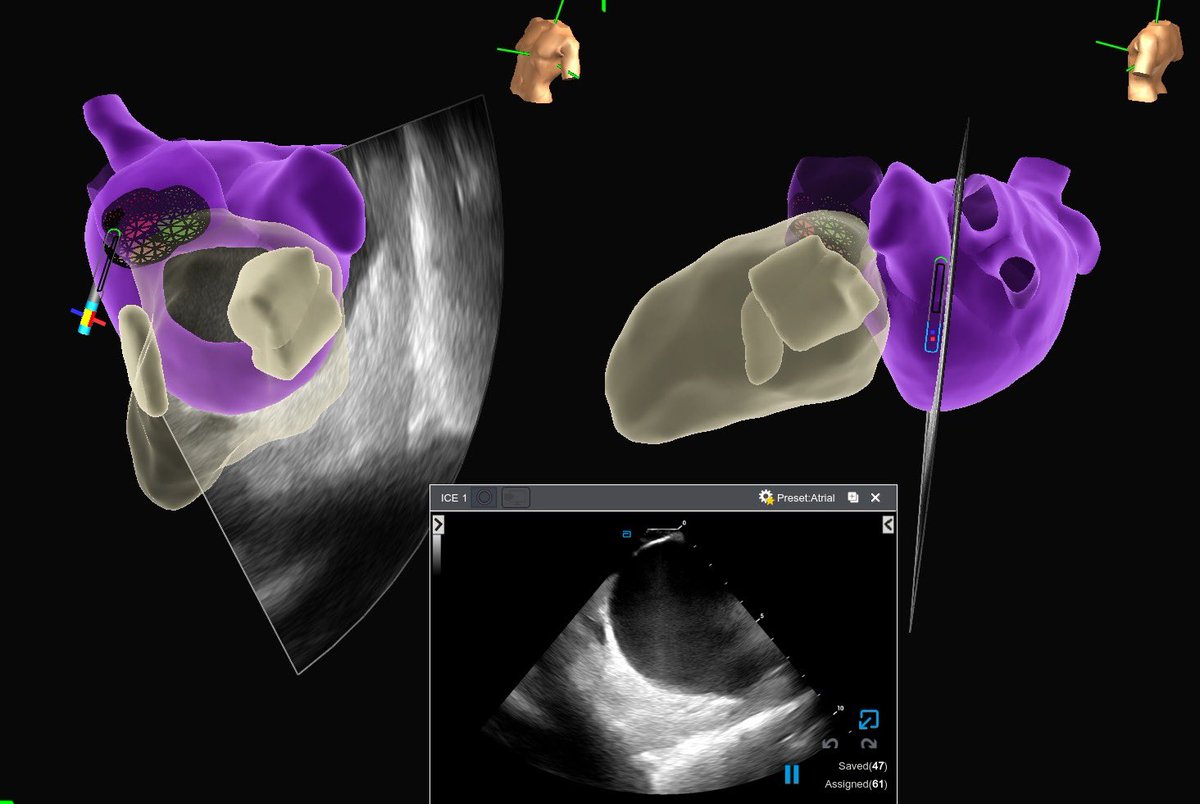
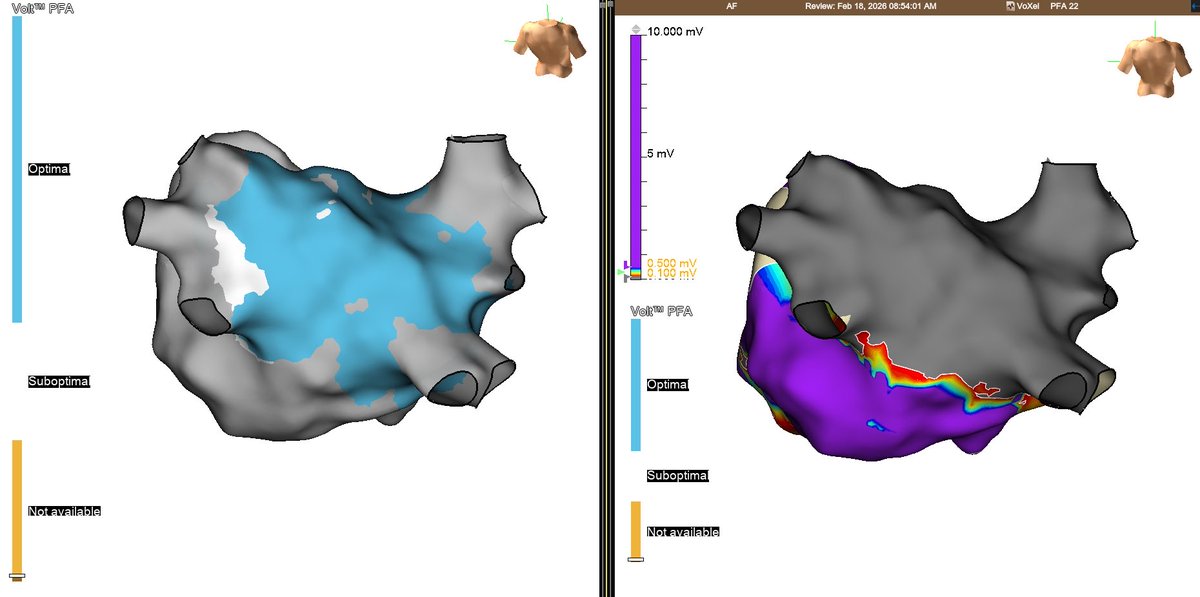
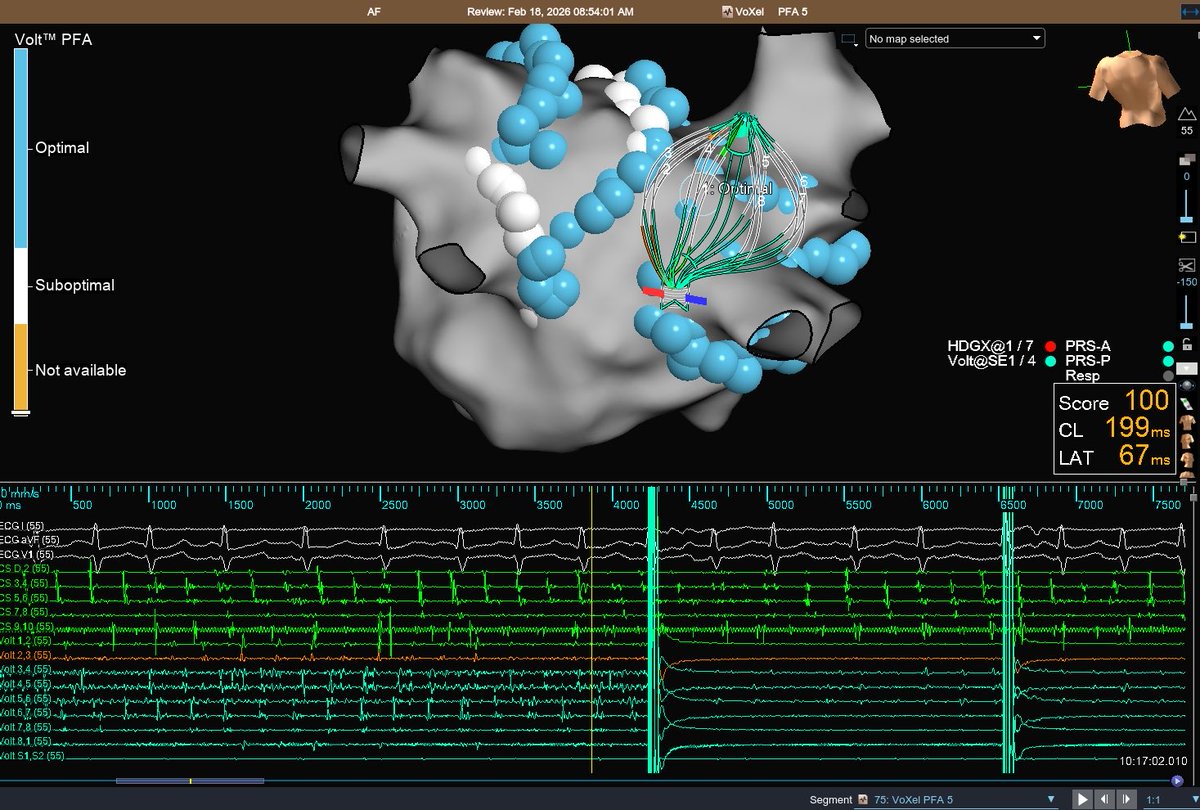
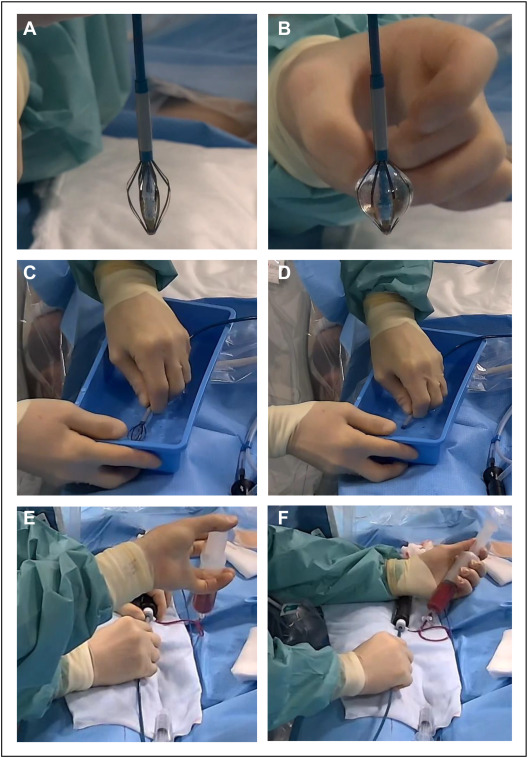
Pulmonary vein isolation using a novel balloon-in-basket pulsed field ablation system: The Lübeck how-to protocol, by @PerWenzel and colleagues
@UKSH_KI_HL@dzhk_germany#EPeeps
https://t.co/Vv3JsYNrru
So Leinster used their privilege to pull some URC strings to have their SA tours moved to the beginning of the season so they could focus on finally winning the Champions Cup… Only to rock up and get licked on their 4th final in 5 years.🤣🤣
#LEIvUBB
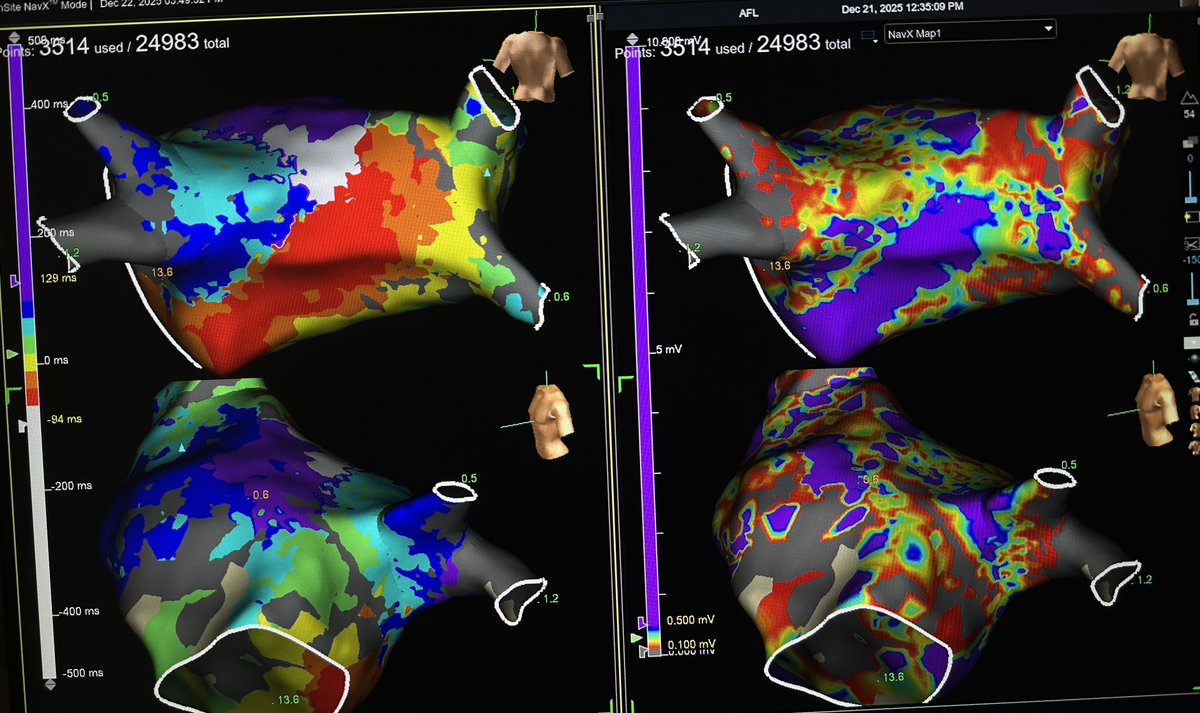
Fun mitral flutter that was hanging by a thread. Middiastolics with a frequency of 460 Hz at the site of termination! Great case with @rachelkaplanmd !
Dominant Ectopic Atrial Pacemaker From the Right Atrial Appendage Base Mimicking Inappropriate Sinus Tachycardia @CleClinicHVTI
https://t.co/h6wd4tyPKm
Intramural anteroseptal substrate, incessant VT with exit close to His region, inducible after RCC 3 RF apps (50W, 90sec each), effective and safe PFA with Tactiflex Duo in RCC with low dose to avoid His damage and coronary spasm @PranavBhagirath@hospitalclinic@aportasanchez
Sinus #ILAM propagation in a patient with prior anterior infarct, apical aneurysm, and apical morphology VT (12-lead ECG mysteriously vanished so I never saw it). Patient loaded up on amio/mexiletine and unable to induce VT during ablation. What do you do next? #EPeeps
The “Blanking Period” after Pulsed Field Ablation for Persistent Atrial Fibrillation: An Implantable Monitoring Subanalysis of ADVANTAGE-AF - Dr. Vivek Reddy #AFSymposium2026
EP is beautiful! Atypical flutter in a pt.with hx. of mechanical MVR! Gradual lengthening and termination at this 👇corridor with nice diastolic buffet! #Epeeps
@Hapa_EP My experience of RPS WPW is that they are the most likely ones with acute success and then late recurrence (despite a 30min wait time). I always recommend Agilis with a contact force abl catheter for improved stability and contact verification. Nice case :)))