📊TENSION trial results are reproducible in routine care
🇩🇪🧠German Stroke Registry data shows similar 90‑day results to the RCT, supporting wider adoption of thrombectomy for large‑infarct stroke
https://t.co/OYqxkT0mrK @WinkelmeierMD@Fie0815@FabianFlottmann@MDoctoronboard
El truco es ocultar el tiempo. Nos exigen 2.598h/año (4 meses extra). ¿Qué pasaría si TODO el hospital trabajara nuestra jornada?
He corrido la simulación.
La brecha colapsa.
🔊 Sigmoid plate dehiscence in pulsatile tinnitus: fixed defect or a dynamic process?
This study shows sigmoid plate bone regrowth in most patients after endovascular stenting, supporting a hemodynamic, potentially reversible process.
🔗 Read more: https://t.co/KtoWF7m9L4
1/Controversy in radiology can get tense!
The Mt Fuji sign for tension pnemocephalus is under scrutiny. When should you call it?
A thread about imaging this important neurosurgery complication
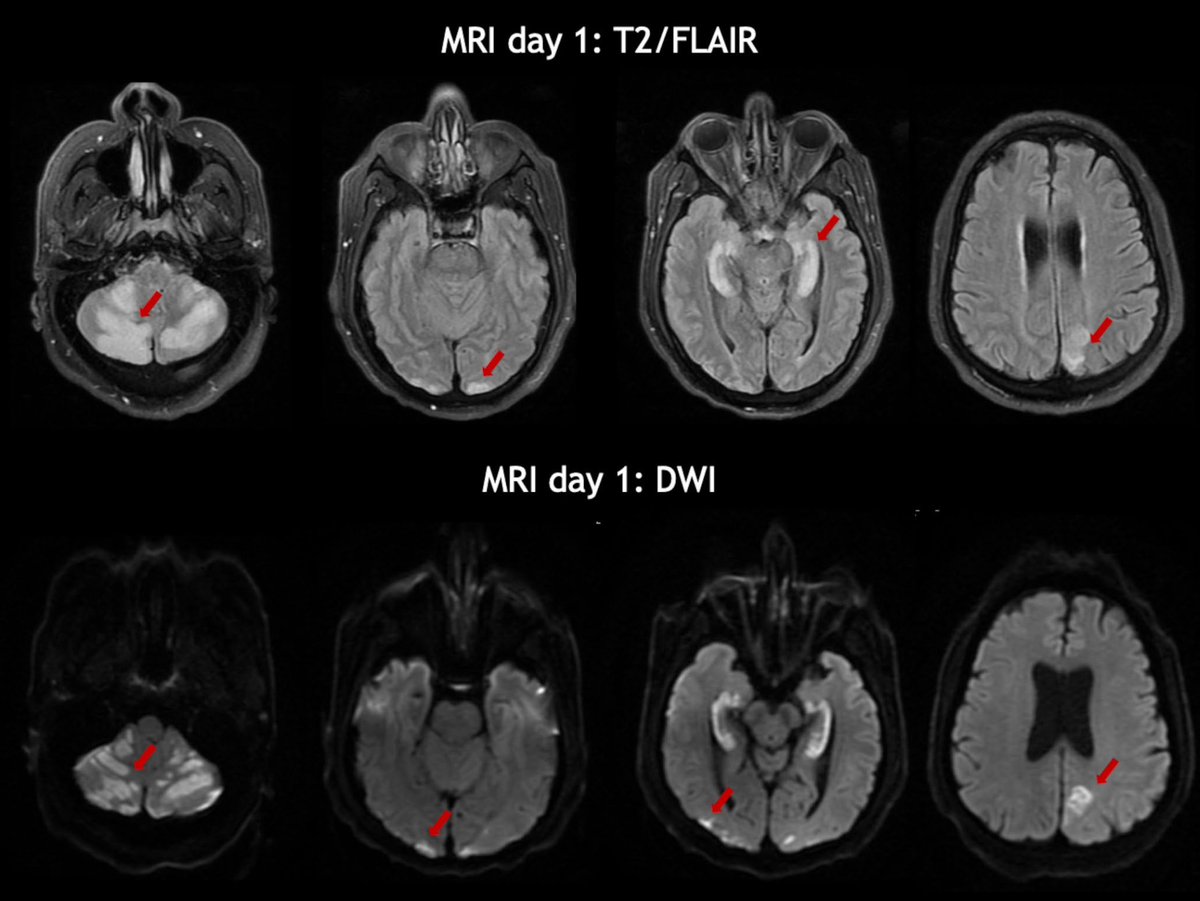
MRI findings of genetic diseases often misdiagnosed as MS. A-D LHON B CADASIL. D CANVAS. E Krabbe disease F Cobalamin C disease. G polymerase gamma gene disease. H Alexander J/K CADASIL L Spastic paraplegia 5 with diffuse leukoencephalopathy https://t.co/h0aW7Cd4hJ
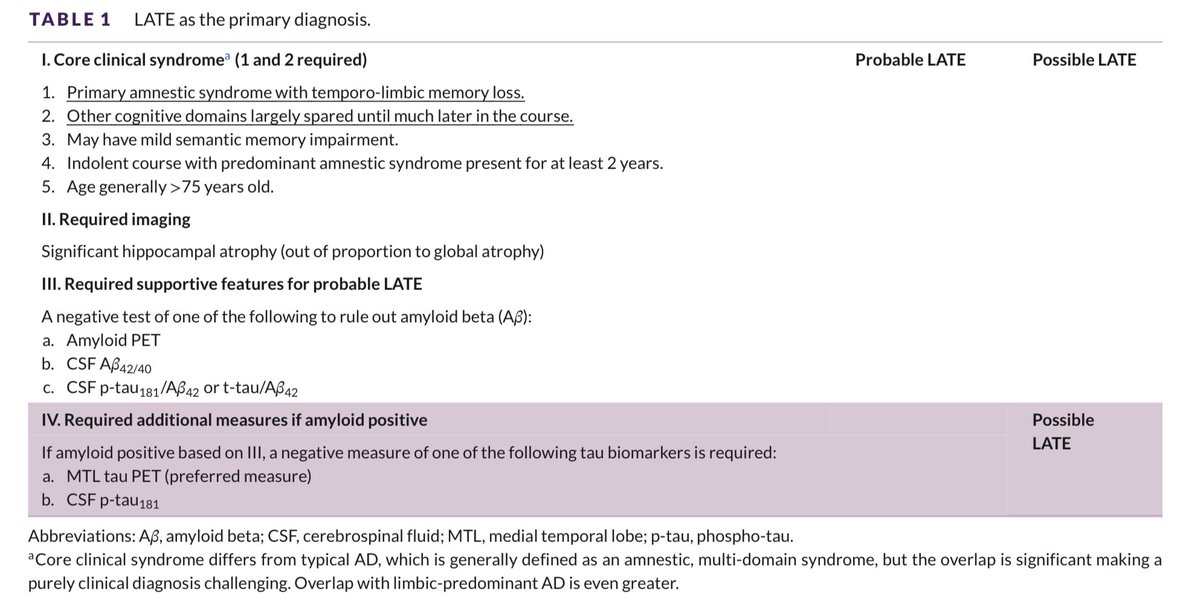
🧠 Pacientes >75a con amnesia leve, atrofia hipocampal llamativa pero sin clara progresión cognitiva.
☝️No siempre es Alzheimer.
👉 Podría tratarse de #LATE, una encefalopatía por TDP-43 que simula EA pero sigue otro curso
https://t.co/2ohgL1ZpfL
Can’t remember what to look for on scans for memory loss?
New Alzheimer’s treatments are changing the way we look at these scans!
Read on for w/the latest @theAJNR SCANtastic on imaging for Alzheimer’s:
https://t.co/1mPC273Xrm
Current hypothesis in AD is that amyloid beta (AB) protein results in inflammation & neuronal death. Treatments in AD are focused on anti-AB antibodies to remove this protein
But AB protein is in vessel walls & removing it increases vascular permeability, leading to edema & hemorrhage
On imaging, this causes ARIA (Amyloid Related Imaging Abnormalities), which may be ARIA-E (edema) or ARIA-H (hemorrhage)
Not everyone gets ARIA. So what means a high risk of ARIA?
Before you dive into treatment, you want to know if they will sink or SWIM—so look for SWIM:
S = superficial siderosis (present/absent)
W= white matter hyperintensities (graded mild, moderate, or severe on the Fazekas scale)
I = infarcts (total number)
M = microhemorrhages (total number)
1-4 microhemorrhages = high risk & need repeat imaging
>4 are excluded
Remember the rhyme:
1 to 4 = need to image some more
If there’s 5, treatment won’t jive
ARIA is usually treated by pausing treatment if it’s moderate to severe. So remember this by the rhyme:
--If they start to feel, then it’s a big deal
--If ARIA findings > 5, then medication deprive
--Or if siderosis > 2, then medication break for you!
Hopefully, now you ARIA will stay in your memory!!
Debate about the clinical application of RANO 2.0. To what extent is it appropriate?
RANO 2.0 application guide for clinical trials:
https://t.co/BWzZ44LXBO
Letter:
https://t.co/l9o8c3mxjk
Reply to the letter:
https://t.co/fhr4ZGoZ51
Opinion article:
https://t.co/0Z6tTKoMZO
📣Do more CTA than MR carotid imaging? Need a way to classify carotid plaque using Plaque-RADS on CTA? Read our work evaluating patients w/ ESUS🧠using CTA-based Carotid Plaque-RADS!
@StrokeAHA_ASA@AHAScience@lucasabaITA@PennRadiology@PennNeurology
📖https://t.co/VJCEHwEspm
New publication: CHANTER is an under-recognized syndrome of multifocal cerebral edema after opioid ingestion. It's important to recognize: diffusion restriction and edema are reversible and outcomes are promising!
Free copy: https://t.co/g5GBaUm49s
@DanHarrisonMD@BWHNeuroICU
Have MULTIPLE questions about MULTIPLE sclerosis?
Having trouble seeing neuromyelitis optica?
In a fog about MOG?
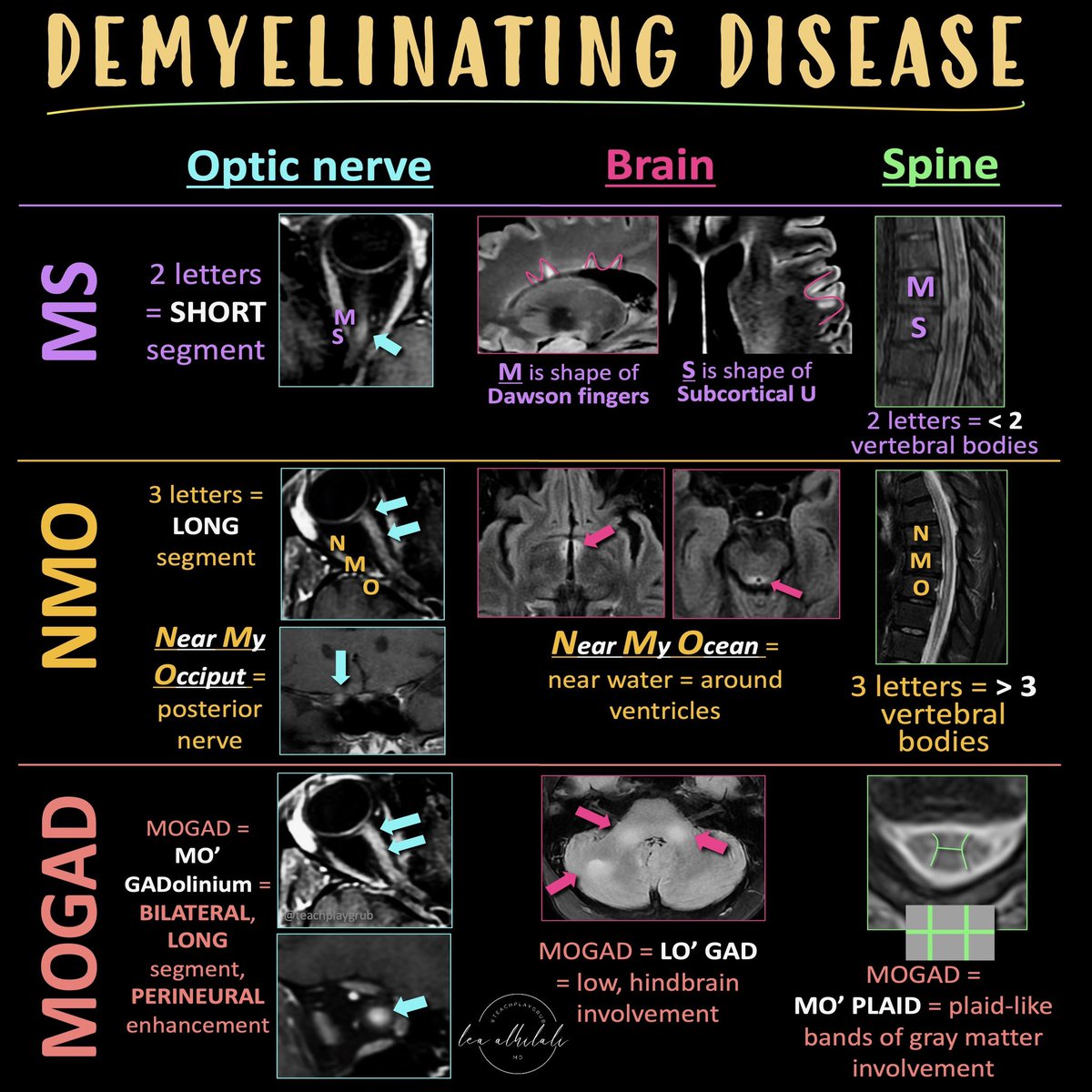
Here’s the cheat sheet you NEED to distinguish the demyelinating diseases!
Demyelinating diseases predominantly involve the optic nerves, brain, & spine.
The three main chronic demyelinating diseases are Multiple sclerosis (most common), neuromyelitis optica (NMO), & myelin oligodendrocyte glycoprotein (MOG) antibody associated disease or MOGAD
Each has its own features in the optic nerve, brain, & spine. Here’s how to remember them!
MS
Optic nerve:
MS only has 2 letters, so MS involvement of the optic nerve tends to be short segment
Brain:
Letter M makes the shape of the perivascular distribution of lesions along the ventricles (Dawson’s fingers)
Letter S makes the shape of the subcortical U fiber involvement
Spine:
MS is only 2 letters, so lesions are usually less than 2 vertebral bodies in length
NMO
Optic nerve:
NMO is a longer abbreviation, three letters, so longer involvement
NMO can stand for Near My Occiput. Occiput is posterior, so more posterior nerve involvement
Brain:
NMO can stand for Near My Ocean. What is your brain’s ocean? The ventricles. NMO lesions are all periventricular
Spine:
NMO is 3 letters, so lesions usually more than 3 vertebral bodies in length
MOGAD
Optic Nerve:
Remember MO’ GAD-olinium. So things that cause more regions of enhancement. MOGAD lesions are commonly bilateral & long segment & enhancement can extend perineural
Brain:
Remember LO’ GAD. MOGAD typically involves the lower areas of the brain
Spine:
Remember MO’ PLAID. MOGAD can give a plaid-like H shape in the cord from predominantly gray matter involvement
Hopefully, this cheat sheet will help you remember how to distinguish the demyelinating diseases! It ain’t lyin’ about diseases of myelin!
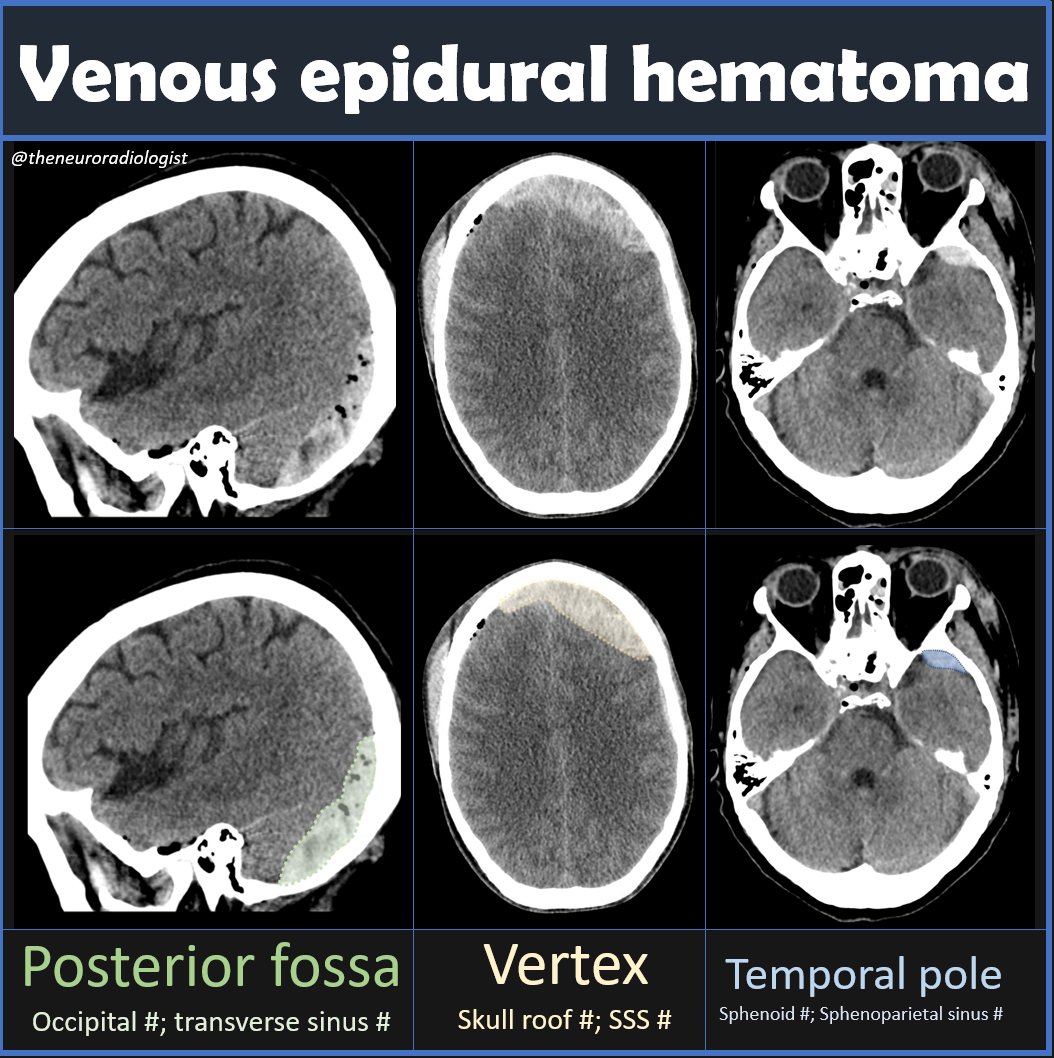
Venous epidural hematoms constitute about 25% of epidural hematomas, look like arterial EDHs (lensshaped), but can be found in three very typical locations: the posterior fossa, near the vertex and near the temporal pole #radiology#neuroradiology#RADed#FOAMrad#MEDed#FOAMed