Most people don’t know why retatrutide’s results are so different from semaglutide or tirzepatide.
It comes down to receptors.
Semaglutide targets one.
Tirzepatide targets two.
Retatrutide targets three - adding glucagon to the mix, which accelerates fat burning in ways the others can’t.
Each receptor added has moved the needle significantly. The Phase 3 results reflect that.
RFK has been saying this was coming for weeks. Now it’s official.
The FDA is removing 12 peptides from the restricted list. BPC-157, MOTS-c, Semax, Epitalon, Thymosin beta-4 among them. Independent scientific review begins in July.
People have been sourcing these through grey markets for years because legitimate access was cut off. That’s what created real risk for real people.
This should never have happened in the first place.
Today, we took long-overdue action to restore science, accountability, and the rule of law.
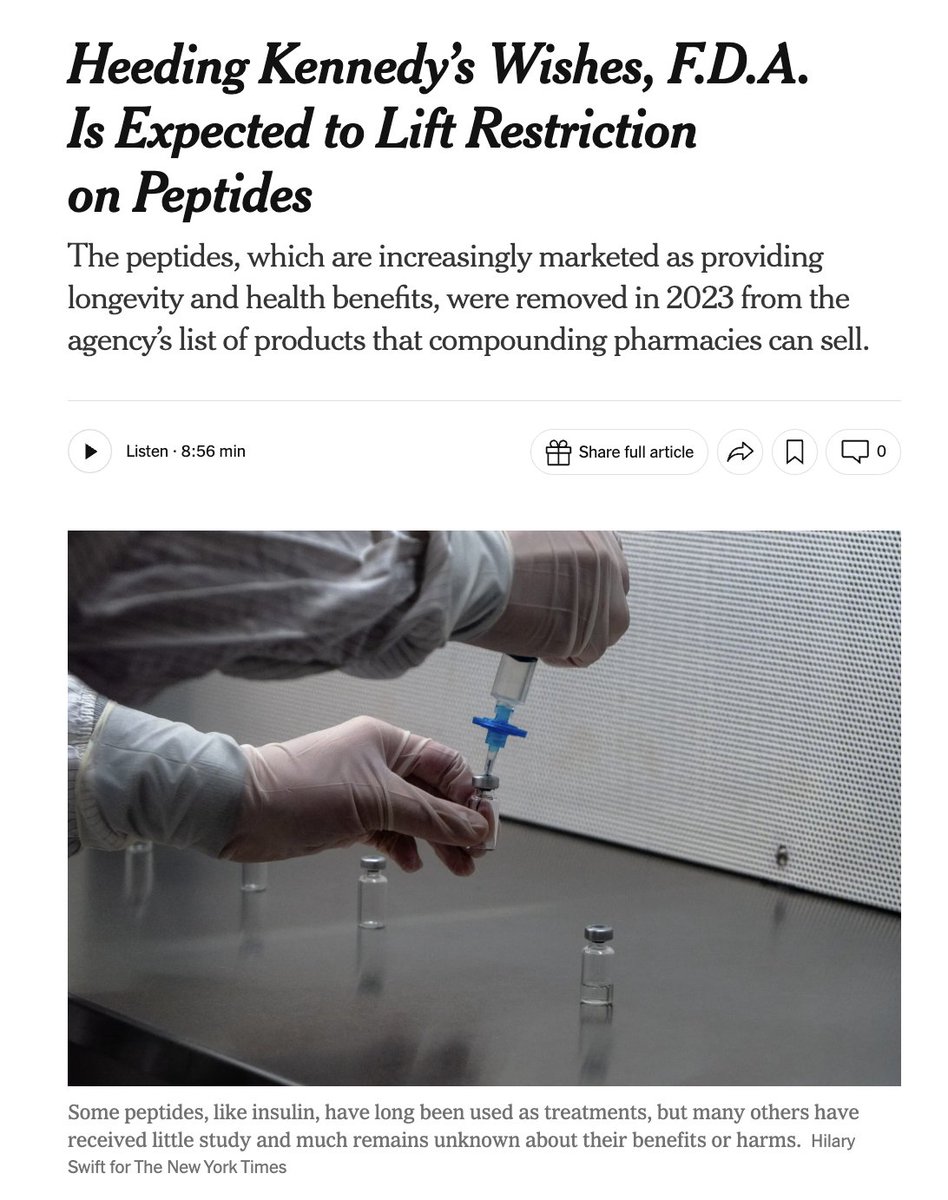
In September 2023, the Biden FDA pushed a number of peptides into Category 2 — “Bulk Drug Substances that Raise Significant Safety Risks” — driving a dangerous black market that puts Americans at risk.
Now, after nominators withdrew 12 peptides, the FDA will remove them from Category 2 and will bring them to PCAC at its next two meetings, beginning in July—where independent experts will rigorously evaluate each substance on its scientific merits using full clinical, pharmacological, and safety evidence.
• BPC-157
• Thymosin beta-4 fragment (LKKTETQ)
• Epitalon
• GHK-Cu (injectable)
• MOTS-c
• DSIP (Emideltide)
• Dihexa Acetate
• Ibutamoren Mesylate
• Melanotan II
• KPV
• Semax (heptapeptide)
• Cathelicidin LL-37
This action begins to restore regulated access and will immediately begin shifting demand away from the black market.
We will follow the science, enforce the law, and deliver the clarity patients, providers, and pharmacies deserve.
GLP-1’s don’t simply cause you to eat less.
They reduce inflammation, reduce cancer, improve arthritis pain, reduce alcohol consumption, protect the heart independent of weight loss, stimulate beta cells in the pancreas, keep you from developing type 2, and generally reduce all cause mortality. 😮💨
So no, you can’t just “eat less” and get the same benefits.
Eli Lilly's orforglipron just got approved as the first GLP-1 pill for weight loss.
A lot of people who passed on injections are about to reconsider.
The barrier to entry just got a lot lower.
Peptide Sciences, arguably one of the largest research peptide vendors, just announced they’re shutting down.
That’s a pretty big deal considering how long they’ve been around.
It also likely won’t be the last.
As compounding pharmacies gain clearer pathways to prescribe peptides, the old “research peptide” vendor model becomes harder to sustain.
A few things worth knowing:
- This doesn’t mean peptides are going away
- Some gray-market vendors will likely disappear
- New ones will also show up quickly
When a big vendor disappears, the market doesn’t disappear.
It fragments.
If this plays out, we’re entering a more regulated phase of the peptide market…but that doesn’t necessarily make it simpler.
Gray markets don’t disappear overnight.
They evolve.
Access and enforcement often expand at the same time.
That increases fragmentation.
More vendors.
More supply channels.
More variability.
More room for protocol error.
Regulation may improve oversight.
It doesn’t remove execution complexity.
Access gets attention.
Structure determines outcomes.
Expect a massive surge in compounding pharmacies, explicit warning labels on gray market peptides (currently is “not for human use”… ) and steep penalties for any venue besides Lilly selling Retatrutide. And per prediction, NIH budget to be increased 1%. More on that soon…
RFK Jr. was just on Joe Rogan’s podcast and said ~14 peptides currently restricted under the FDA’s Category 2 list could soon be eligible for legal compounding again.
If implemented, that would materially EXPAND peptide access in the U.S.
Category 2 status currently restricts compounding due to safety concerns.
Moving substances to Category 1 would allow regulated U.S. pharmacies to compound them under oversight, potentially reducing reliance on unregulated sourcing.
Access expansion changes behavior quickly.
If more peptides become legally compoundable, we’ll likely see:
- More first-time users
- More stacking
- Faster experimentation
- More telehealth activity
But increased availability doesn’t automatically improve outcomes.
More compounds in circulation often means:
- Overlapping protocols
- Escalation mistakes
- Inconsistent cycles
- Less clarity on what’s actually working
Regulatory shifts may improve supply chain oversight.
They don’t replace execution discipline.
Whether 14 peptides move or not, one variable remains constant:
Outcomes depend on structured use.
Clear protocols.
Intentional dosing.
Consistent tracking.
If peptide access expands, structured protocol management becomes even more important.
That’s exactly why PepTracker exists.
🚨 BREAKING NEWS: RFK Jr. says ~14 of 19 banned peptides can be legally compounded again by US pharmacies within a few weeks. This will ensure Americans are getting "a good product… from ethical suppliers" vs. black market drug dealers that provide "substandard product" with serious safety risks.
The 19 compounds on FDA’s Category 2 compounding safety list include:
• BPC-157
• Cathelicidin LL-37
• Emideltide (DSIP)
• Epitalon
• GHK-Cu (injectable)
• GHRP-2 (injectable/nasal)
• GHRP-6
• Ipamorelin acetate
• Kisspeptin-10
• KPV
• Melanotan II
• PEG-MGF (pegylated Mechano Growth Factor)
• MOTS-C
• Semax
• Thymosin beta-4 fragment (LKKTETQ)
• AOD-9604
• CJC-1295
• Selank acetate (TP-7)
• Thymosin-alpha 1 (Ta1)
The five least likely to be legalized in a policy shift would be those with the most troubling safety signals or the weakest human data — for example: Melanotan II, Cathelicidin LL-37, GHRP-2, Ipamorelin acetate, and CJC-1295 — because of documented serious adverse events or other red flags in FDA’s risk assessment.
As more GLP-1 options enter the market, oral or injectable, the variable that won’t change is execution.
If you’re running a protocol, track it.
We built PepTracker for exactly that.
https://t.co/tIAwJOpDrX
Lilly’s oral GLP-1 (orforglipron) outperformed oral semaglutide in A1C and weight loss in a head-to-head T2D trial published in The Lancet.
This is meaningful comparative data.
But let’s add some context… 👇
In a head-to-head type 2 diabetes trial, our investigational GLP-1 pill delivered superior blood sugar control and weight loss compared to another GLP-1. Detailed results were published today in The Lancet. Read more: https://t.co/531zlZOUJ8
The molecule matters.
But behavior matters more.
Whether it’s:
- Injectable semaglutide
- Tirzepatide
- Retatrutide
- Orforglipron
The winners will still be the ones who track, escalate intentionally, and stay consistent.
That’s the part most headlines miss.