Valproic acid is great for refractory agitated delirium.
🏆 Especially useful in patients with explosive/aggressive behavior in the context of a personality disorder (often exacerbated by delirium).
Candidates for VPA:
✅ Not pregnant
✅ No severe liver dz or history of hyperammonemia
✅ No major drug-drug interactions with VPA
✅ Didn't respond to antipsychotics +/- alpha-2 agonists (dexmedetomidine). This isn't a hard requirement, but generally VPA isn't usually a front-line agent.
Advantages of VPA:
👍 Cardiovascular stability
👍 Low risk of airway compromise (only mildly sedating)
👍 Antiseizure activity (e.g., can be used for sz prophylaxis in an agitated patient)
👍 Can be given IV or PO (1:1 conversion with immediate-release formulations)
👍 EM/ICU folks should be knowledgable and comfortable within it already
Disadvantages of VPA:
👎 Dosing requires a little more thought than most agents. For patients on this for more than a few days you want to check a VPA trough and adjust it using the Fraser equation (to account for albumin).
👎 Can cause a lot of side-effects (but most of these are due to *chronic* VPA, rather than just a few days of therapy)
Dosing
🎯 My preference is to use the same dosing regimen as for status epilepticus (40 mg/kg load max 3 grams, then 15 mg/kg/day in divided doses). You can up-titrate as needed while following VPA troughs if ineffective (max dose of 45 mg/kg/day).
🎯 Many studies have reported starting lower and up-titrating, but this delays its efficacy for 2-3 days.
🎯 Using more frequent doses (e.g., q6hr rather than q8hr) may avoid toxic peak levels while maintaining adequate trough levels.
This isn't an option I use a ton, but it's a terrific tool to have in your toolbox for agitated delirium that isn't responding to usual front-line treatments.
⚠️ VPA should be weaned off prior to hospital discharge (unless the patient is seen by psychiatry and they are intentionally recommending VPA as chronic outpatient therapy for bipolar disorder etc - which would be uncommon).
(more discussion on VPA pharmacology in the IBCC chapter on status epilepticus)
Recent article on this in NeuroCritical care here:
Literally the most fulfilling intervention as a pharmacist is providing a warm blanket to a cold patient, like idec it’s not med related it’s SO wholesome.
Patients be making me BLUSH w their warm blanket praises 🤭
Had the privilege of presenting my PGY2 research project on VPA for agitation/delirium in neurosurg ICU patients at NCS last week.
Great week of learning and exploring sunny San Diego 😎
🚨NEW POD ALERT🚨
2024 @neurocritical Annual Meeting
Thursday Mini-Recap #NCS2024
Highlighting 16 research posters presented at the conference!
All 16 poster images included in thread below
🟢 https://t.co/4k3MVF3BHg
Standing room only at #NCS2024 session on @brain_trauma penetrating #TBI guidelines.
Long awaited with useful algorithms including tool for assessing futility. Most importantly, advocates for aggressive surgical treatment and acknowledges challenges with prognostication.
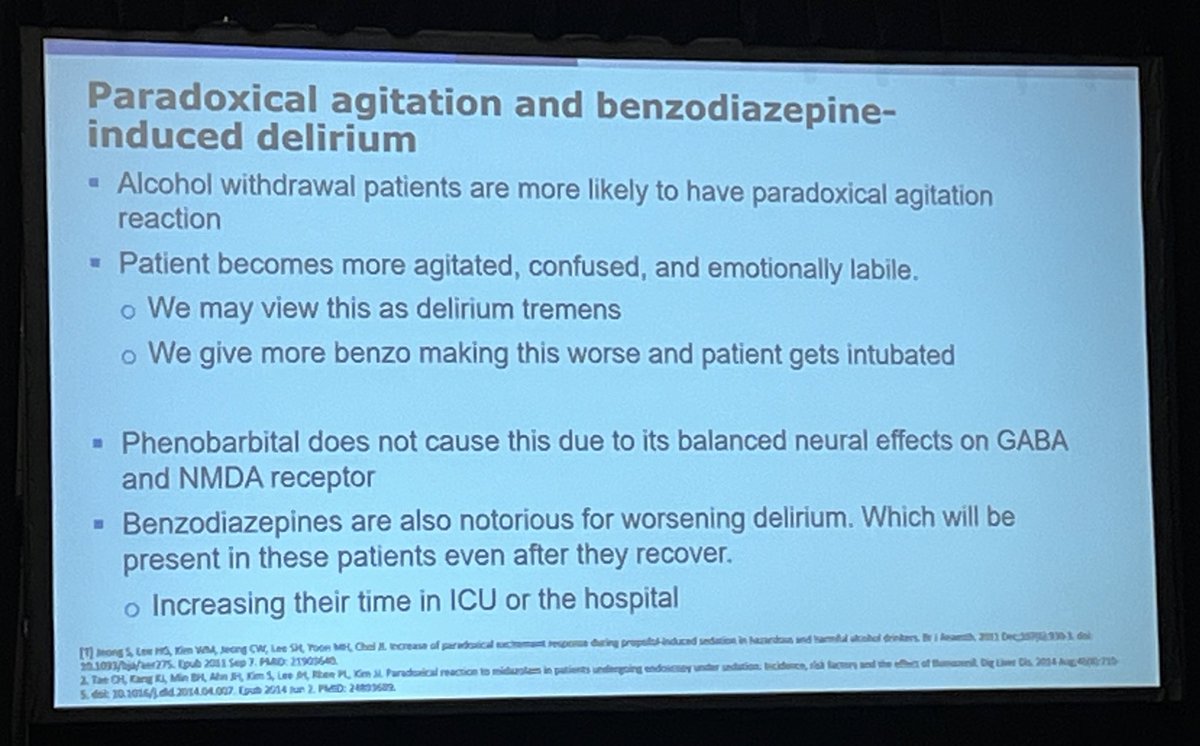
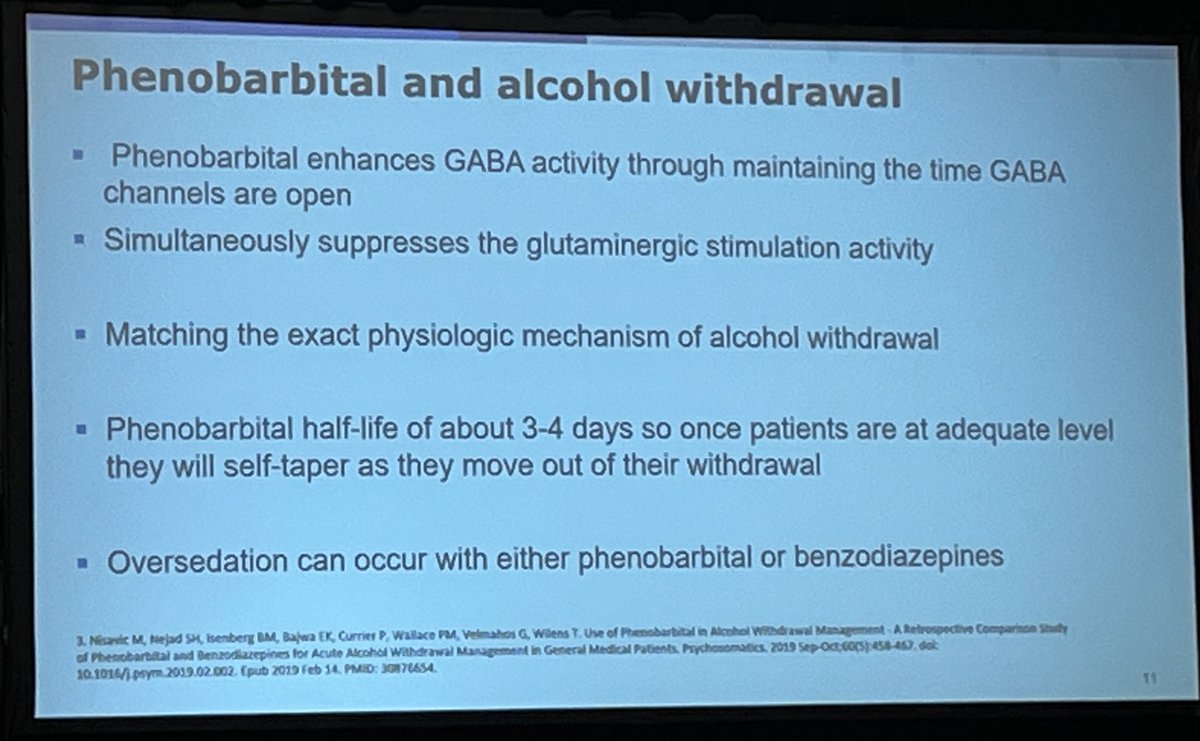
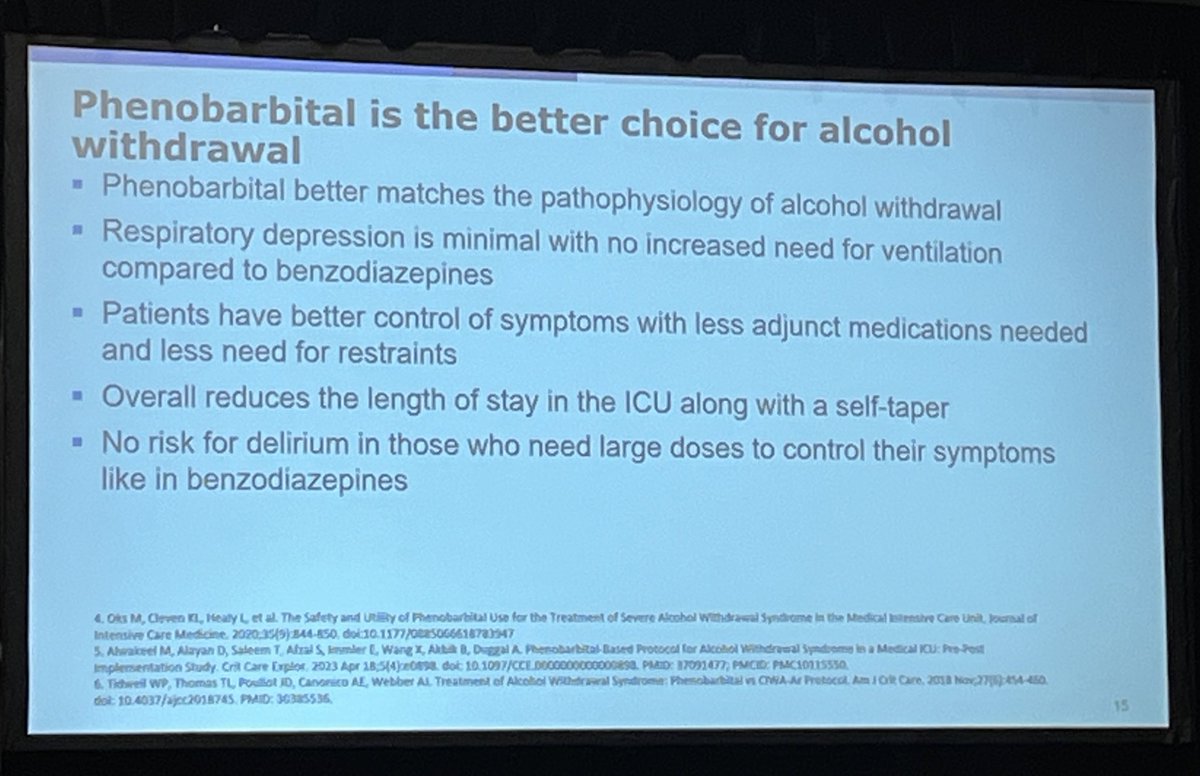
Pro-argument:
- better pharmacokinetics (longer acting, self taper) & anti-NMDA effects make PHB superior to BZDs
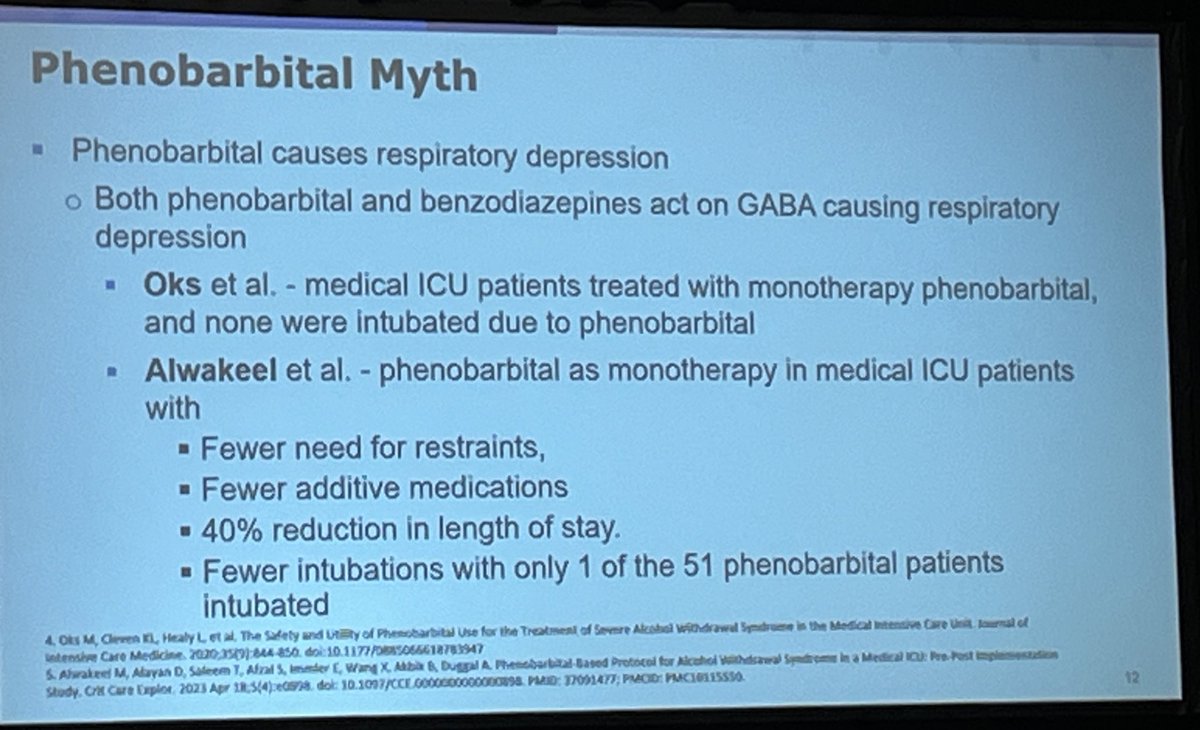
- less respiratory depression with PHB
- (limited) studies suggest PHB results in fewer additive meds & restraints, as well a 40% reduction in LOS
#CHEST2024