@norfolk_tim @msiuba@load_dependent 2/2
1) pushing patients to their limit of fluid responsiveness is putting them in a non physiological state.
2) I find that often, as opposed to me!, patient in the ICU are not fluid tolerant. So I don't go far on the FR path..
@ThinkingCC
@norfolk_tim Agree with @msiuba and @load_dependent .
1/2
You and I right now are fluid responder. Yet we don't need fluid. If I receive 2 l of LR, it won't hurt me much. I am fluid tolerant as well.
We are releasing the interim (final data coming and publication submission pending) data from our amazing mpRCT collaboration w/ @ATTACC_COVID @remap_cap to aid in clinician decision making on anticoagulants for #COVID19: https://t.co/Tg78vM5xfD @nih_nhlbi @macky_neal
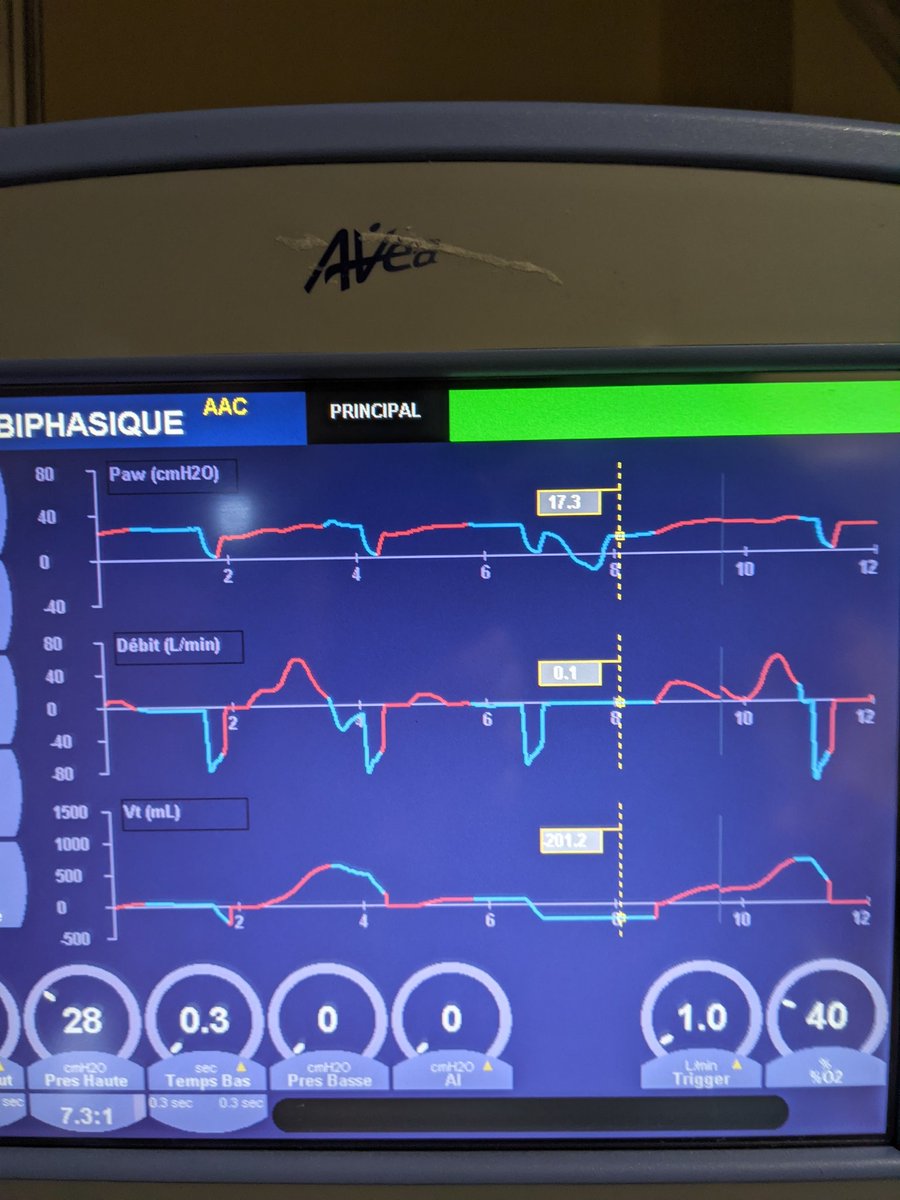
@erico_vale@Francofoam1@khaycock2@PulmCrit My understanding is that it's best if the patient is spontaneously breathing on top of T high. It improves PCO2 (Among other things).
Hence avoiding if possible NMB and use the least amount of sedatives.
I have seen comfortable and awake patient under this mode. Cheers
@load_dependent@NephroP Great point about septum.
I find that PW Doppler analysis on portal vein is easier (less subjective?! at least for non cardiologist...).
Also, by septum movement alone, isn't more difficult to have a diuresis stop point?
















![TheRounds's tweet photo. Join Dr. Mallemat [@CriticalCareNow] for the next week at The Rounds Virtual Conference #FOAMed #resuscitation https://t.co/8F6dNoUBS8 https://t.co/CerJeri74O](https://pbs.twimg.com/media/DA7_YUoVoAARO0v.jpg)





























