Some thoughts on who should be admitted to Stroke Units and how fast! in respose to Europe Stroke Action Plan @ESOstroke@draravindganesh@nishita_singh3 https://t.co/ndW8x1HE38
🚨 🌍 WHO has adopted its first-ever stroke resolution, recognising stroke as a full continuum of care, from prevention to rehabilitation.
👉 The resolution sets out 16 operative actions for Member States
Read about the resolution here!👇
https://t.co/82b7KbjlcT
Fantástica iniciativa la I jornada de investigación del @HospitalUVRocio inspirador contar con tan buenos compañeros! Y el ATILA ha sido premiado, imposible agradecer a todos los que han hecho posible este estudio. A por más!
The HOPE Trial
Does personalized BP control after EVR (<160 for TICI 2B and <140 for TICI-2C/3) improve outcome compared to standard of care (SBP <180)?
Yes -- a 13% absolute increase in favorable outcome (mRS 0-2) and a 9% absolute decrease in hemorrhagic transformation.
Is this a new standard of care? Let us know what you think!
Personalized Blood Pressure Targeting After Endovascular Therapy for Acute Ischemic Stroke https://t.co/4GpqbfJ4hQ
La Inteligencia Artificial no va a sustituir a los médicos.
Y el problema no es tecnológico.
Es mucho más incómodo que eso.
Porque diagnosticar no es solo acertar.
Es sostener la duda.
Es detectar lo que no encaja.
Es cambiar de hipótesis cuando la evolución del paciente rompe el guion inicial.
Un reciente estudio publicado en JAMA Network Open analizó 21 modelos de IA de última generación para evaluar algo mucho más complejo que responder preguntas médicas cerradas: su capacidad de razonamiento clínico real.
Y los resultados dejan una reflexión importante.
Cuando los datos ya están ordenados y estructurados, los modelos funcionan sorprendentemente bien.
Pero cuando aparece la incertidumbre clínica (el verdadero territorio de la medicina), el sistema se rompe.
La mayoría de modelos fracasan al construir diagnósticos diferenciales complejos, tienden al cierre prematuro y muestran enormes dificultades para sostener hipótesis alternativas en el tiempo.
La medicina no consiste en encontrar la respuesta más probable en una lista de síntomas.
Consiste en interpretar matices humanos, contexto, evolución y biografía.
Y eso exige algo que todavía no puede automatizarse: criterio clínico.
La IA será una herramienta extraordinaria para reducir burocracia, sintetizar información o apoyar procesos de baja complejidad.
Pero convertirla en un sustituto autónomo del razonamiento médico no solo es prematuro.
También puede ser peligroso.
Porque el verdadero acto médico no es acertar. Es navegar la incertidumbre sin dejar solo al paciente.
🧠💫Somos el hospital que más pacientes con ictus aporta al ensayo internacional ‘We-Trust’. Este estudio, en el que están solo tres hospitales en España y 16 en todo el mundo, pretende reducir en 30 minutos el tiempo de asistencia.
#SomosHUVR
https://t.co/Kt4yhynJ9J
📊Meta-analysis of RCTs
🧠💊In patients without clear anticoagulation indication, coagulation‑pathway therapies did not reduce covert brain infarcts (CBI) vs antiplatelets
👉 Composite endpoints dominated by CBI may not reflect clinical stroke benefit
https://t.co/ka7POUjwtC
Focused Update: Immune Response in #Stroke 🧬 Brain–immune interactions are dynamic and central to stroke. Immune cells contribute to both injury and repair, with emerging brain–peripheral circuits redefining the neurovascular–immune interface. https://t.co/QqHlHvuHSE
🧠7T PC-MRA revealed two distinct perforator hemodynamic phenotypes in single subcortical infarction (SSI):
👉Proximal inflow limitation in SSI+parent artery disease (PAD)
👉Diffuse distal hypoperfusion in SSI−PAD
Read more here⬇️
https://t.co/cestk3n1Rj
🧠Ayer se celebró el preestreno de 6:15 y Agujas, dos cortos sobre migraña que ponen imágenes y palabras a una realidad que muchas veces no se entiende.
Visibilizar la migraña es una obligación. Reducir el sufrimiento y la culpa de quien la padece, una necesidad.
📊Exploratory analyses of TRACE‑III
💉Tenecteplase (4.5–24h) may benefit late-window stroke patients without thrombectomy
👉❗️Effect depends on infarct growth rate
Read more here👇
https://t.co/KcktWOcqwk
This year’s @ESOstroke Conference saw late-breaking presentations from multiple clinical trials indicating the benefits of tirofiban as an adjunctive therapy in acute ischaemic stroke patients
#ESOC2026@ELeNaZapS@JAMA_current
https://t.co/pFubJxxL3y
🧠🩸Hemorrhagic Transformation (HT) remains an important complication after emergent intracranial stenting
💊☝️High‑intensity antiplatelet therapy appears safe in select HT subtypes and was associated with⬇️lower occlusion and mortality
Read more here👇
https://t.co/qNajHtPkQ1
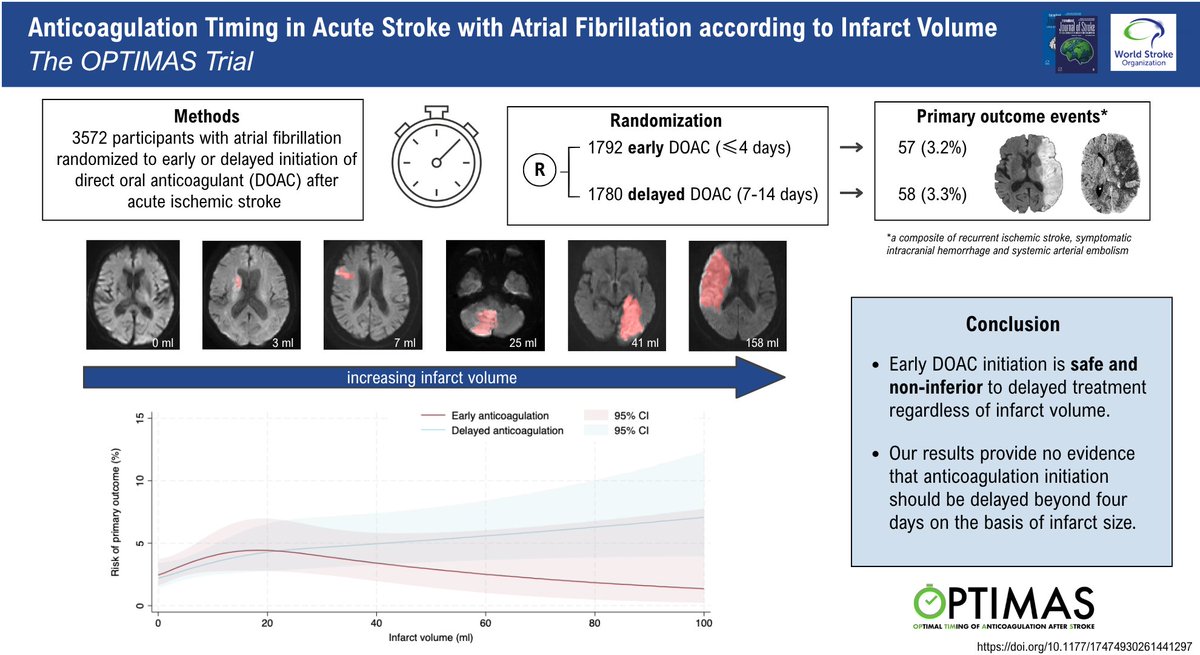
💊Early DOAC initiation is safe and non-inferior to delayed treatment regardless of infarct volume
❌⏱️No evidence that anticoagulation initiation should be delayed beyond 4 days on the basis of infarct size
Read the paper here!👇
https://t.co/3P82y5VF72 @UCLStrokeRes
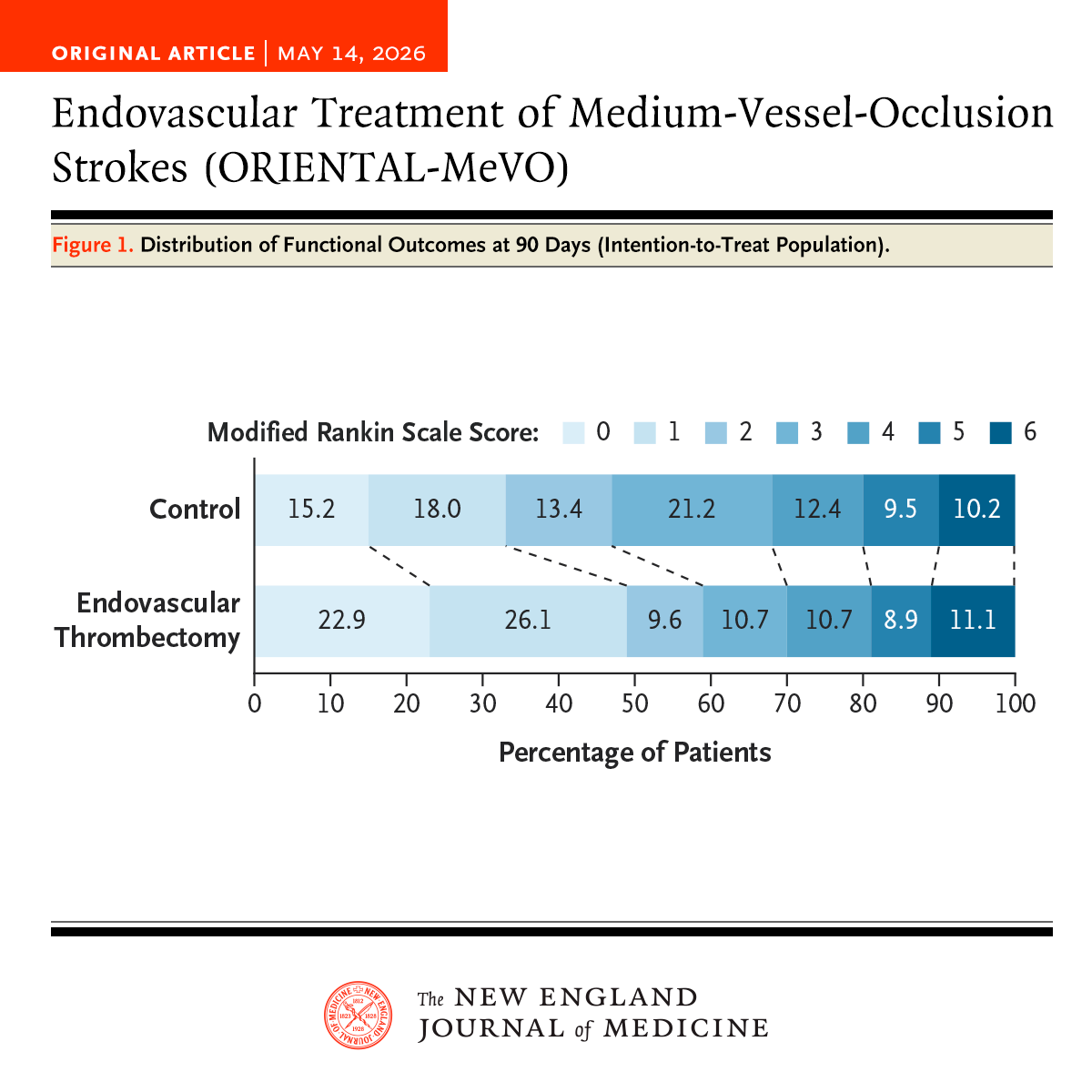
Among patients with stroke due to medium-vessel occlusion, thrombectomy led to functional independence at 90 days (in 58.6% of patients, vs. 46.6% with medical management) but also to a higher risk of intracranial hemorrhage. Full ORIENTAL-MeVO trial results: https://t.co/FvyLPQz4CV
Editorial: Endovascular Therapy for Medium-Vessel Occlusion Stroke — Narrowing the Target Population https://t.co/hnLi0DvzuF
#MondaytTip#Malignant MCA stroke is a neurosurgical emergency...
☝️but DHC is not just a technical decision
📉It reduces mortality, often with major disability
🔍Recognise early
👥discuss within 48h
🎯and centre patient values
From: https://t.co/sTXhjaedGC
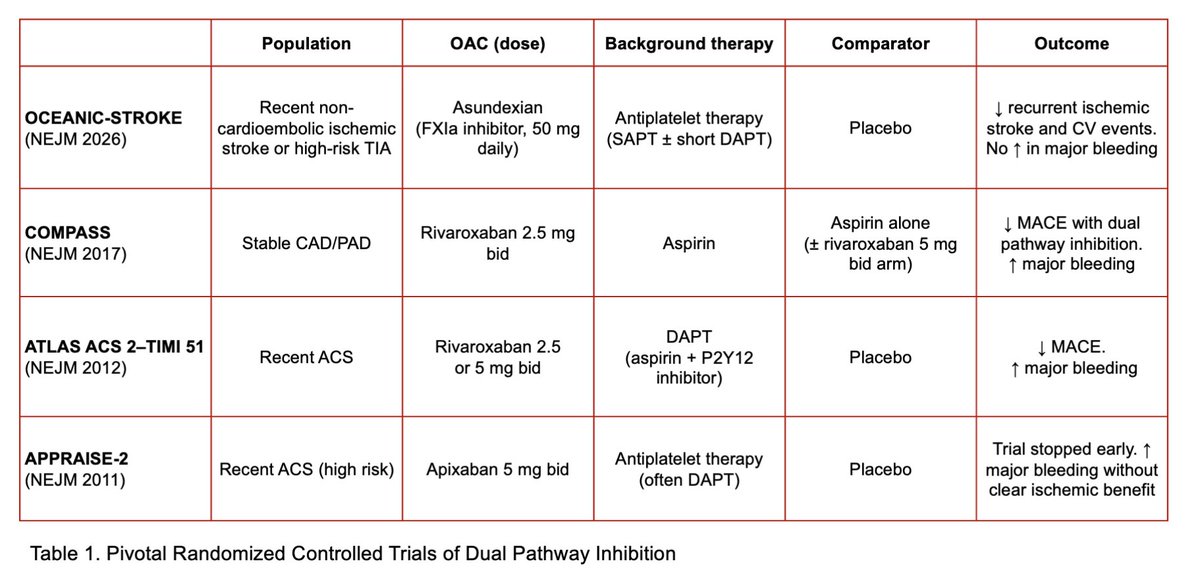
OCEANIC-STROKE & the Evolving Role of Dual Pathway Inhibition
Check out the 🆕 @ESCStrokeBlog!
https://t.co/layjttYh1n
📚@NEJM paper: https://t.co/9vvpEucJrm
Asundexian for Secondary Stroke Prevention
@JacopoImberti@tritz98