CardioNugget™ 💡
Why can't you calculate RVSP from a torrential TR jet?
In torrential TR, the tricuspid valve behaves more like a wide-open conduit than a restrictive orifice.
➡️ Massive regurgitant flow causes rapid RV-RA pressure equalization early in systole.
➡️ The CW Doppler envelope becomes early-peaking and triangular with a low peak velocity.
Therefore:
❌ 4V² no longer reliably reflects the true RV-RA pressure gradient
❌ RAP is underestimated because IVC-based estimates do not capture the giant systolic c-v waves seen in severe TR
The result is a falsely low calculated RVSP/PASP.
Parabolic TR jet = pressure lesion → Bernoulli works
Triangular TR jet = flow lesion → Bernoulli fails
https://t.co/dYRan7MEHA
#EchoBoards #CardioNugget #CardioTwitter #ASEcho #CardiologyFellowship
Is there a ‘better’ TTR stabilizer? How should we even measure stabilization? Complex issues - check out the manuscript by Judge et al & my accompanying editorial in this month’s @JACCJournals JACC:CardioOncology! https://t.co/k9ajoBbh1J https://t.co/TNRWFWZGWn
🫀 #CardioNugget™
Expiratory diastolic flow reversal in the hepatic veins = think constrictive pericarditis.
🔑 During expiration, LV filling increases while RV filling decreases due to enhanced ventricular interdependence. This causes a rise in RA pressure and prominent hepatic vein diastolic flow reversal.
#EchoBoards #CardioNuggets #ASEcho #PericardialDisease #FOAMEd
🏃♂️⚡ Can exercise stress testing (EST) improve the diagnosis and risk stratification of #BrugadaSyndrome?
A fascinating new state-of-the-art review highlights that exercise testing is much more than a tool for assessing exercise capacity. In Brugada syndrome, the *recovery phase* may be the key moment to uncover concealed disease and identify patients at higher arrhythmic risk.
🔍 Key takeaways:
✅ Type 1 Brugada ECG pattern is rarely unmasked during peak exercise (~1%) but becomes evident in up to 25% of patients during early recovery.
✅ The transition from sympathetic activation to parasympathetic rebound appears to play a crucial role in ECG changes and arrhythmogenesis.
✅ Premature ventricular contractions (PVCs) occurring during early recovery may represent an important marker of future ventricular fibrillation risk.
✅ Exercise-induced malignant arrhythmias are rare, suggesting that EST is generally safe when performed with appropriate monitoring.
✅ Careful ECG monitoring during the first minutes of recovery may provide valuable diagnostic and prognostic information.
💡 The review supports the concept that both *peak exercise* and *early recovery* offer complementary insights into the electrophysiological substrate of Brugada syndrome and may help refine individualized risk assessment.
An important reminder that sometimes the most informative part of a stress test is not the exercise itself—but what happens immediately afterwards.
#BrugadaSyndrome #Electrophysiology #Cardiology #InheritedCardiacConditions #SuddenCardiacDeath #Arrhythmias #SportsCardiology #ExerciseTesting #ECG #RiskStratification #PrecisionMedicine #JACCAsia
The following tracing was obtained during threshold testing for LBBAP lead (unipolar). #Epeeps
Change in QRS shown below- Whats happening? Poll below 👇👇
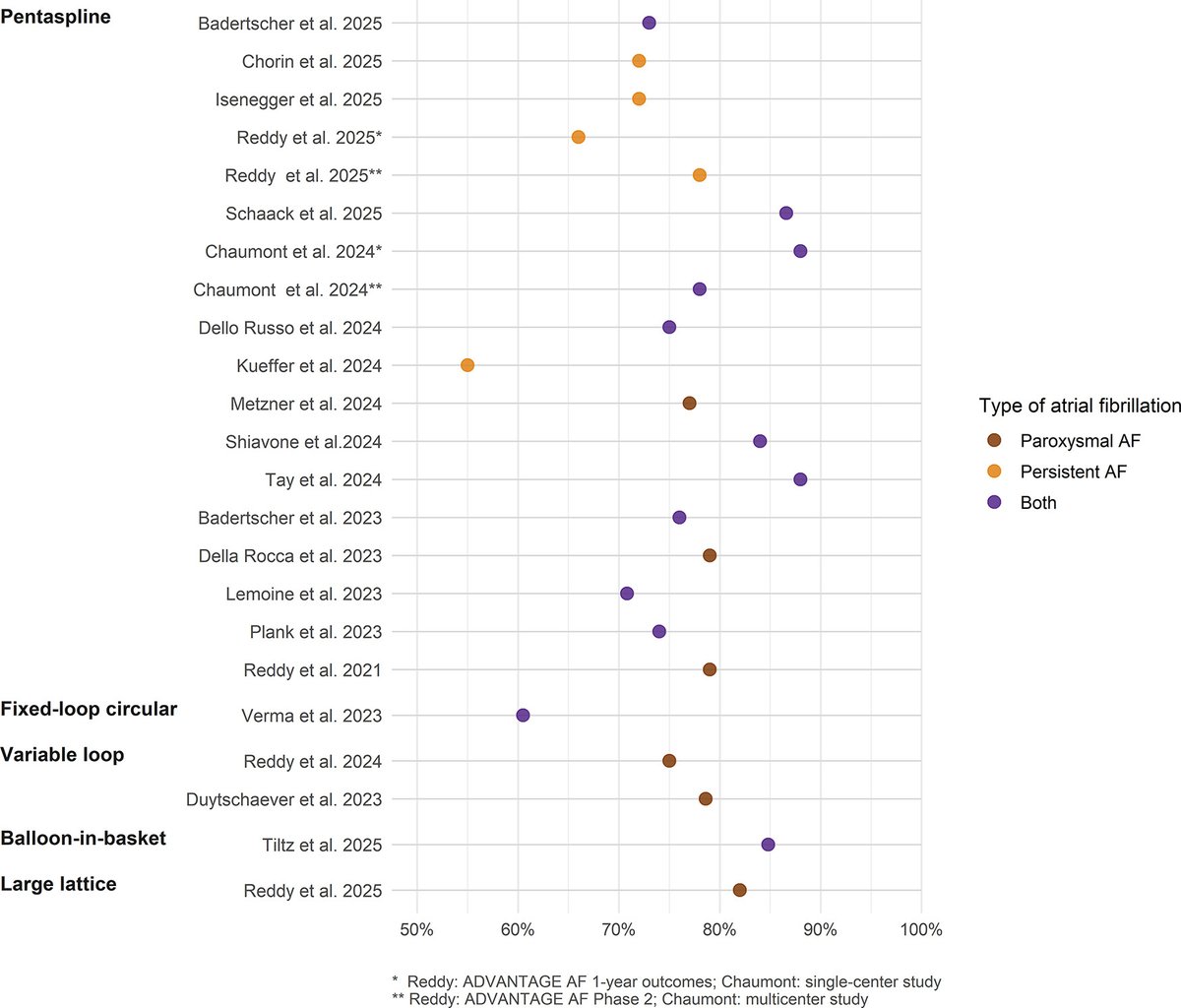
🎯 Efficacy findings: Acute success is no longer the differentiator
➡️Across all currently available single-shot PFA platforms—acute PVI approached 100%.
➡️First-pass isolation was generally mid-90s to 100%, with only a few outlier studies reporting lower rates.
➡️Long-term arrhythmia approximately 55–88% at 12 months (6 months for the balloon-in-basket system). ✴️However, direct comparisons between catheters are difficult because studies differed substantially in AF type (paroxysmal vs persistent), monitoring intensity, adjunctive lesion sets, and f/U protocols.
🧑🎓The most important observation is that evidence supporting dose escalation remains surprisingly limited
⭐️Only two studies specifically evaluated whether delivering additional applications improved outcomes. ⭐️Neither a simplified dosing protocol nor the addition of extra “olive” applications resulted in a significant improvement in freedom from arrhythmia.
Vena de Marshall. 🫀⚡️
🔶️La vena de Marshall es un remanente de la vena cardinal izquierda embrionaria que discurre entre la orejuela izquierda y las venas pulmonares izquierdas.
🔶️Lo importante es lo que contiene:
⚡ Fascículo de Marshall (tejido muscular arritmogénico).
⚡ Plexos autonómicos simpáticos y parasimpáticos.
⚡ Conexiones epicárdicas protegidas por grasa.
🔶️Por ello participa en los 3 pilares para generar FA:
🔸️Trigger: genera extrasístoles que inician FA.
🔸️Sustrato: favorece circuitos de reentrada y gaps epicárdicos.
🔸️Modulación autonómica: la estimulación de sus plexos puede inducir FA.
🔶️ La vena de Marshall no es un simple vestigio embrionario; es una estructura neuro-muscular capaz de iniciar, mantener y perpetuar la FA. Por eso se ha convertido en un objetivo terapéutico clave en la ablación moderna de la FA persistente (la infusión con etanol surge como nueva opción). 🫀⚡
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 💯👌🏻
https://t.co/wRtVPFbmZ6
https://t.co/qWJKrnsDI0
#CardioNugget™
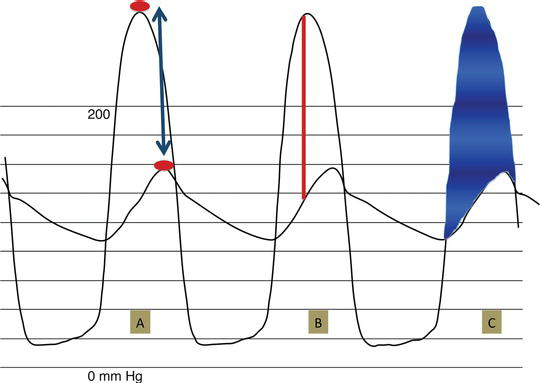
Cath gradients in AS are not all the same:
Peak-to-peak gradient
Peak LV systolic pressure − peak aortic systolic pressure
The peaks occur at different times → not a true instantaneous gradient
BUT clinically, the peak-to-peak gradient often approximates the mean transaortic gradient.
Peak instantaneous gradient
Closest equivalent to Doppler peak gradient
Mean gradient
The shaded area
Average of all instantaneous LV–Ao gradients during systole
Clinical pearl:
-Echo/cath mean gradients are most clinically useful
-Peak-to-peak gradient should not be used interchangeably with Doppler peak gradient
#CardioNuggets #MedEd #CardioMed #CardioMed #EchoFirst #AorticStenosis #MeanGradient
📊 📝📚 Excited to have attended and presented at #ASCO26. Grateful for the experience. Looking forward to future returns.
Read more on our abstract here: https://t.co/PBW1wylwUM
Cardiovascular considerations BEFORE cancer therapy🫀
The first of a 3 part #JACCCardioOnc Expert Panel series exploring CV care before, during, & after cancer therapy.
🫀Goals of CV evaluation Prior to cancer therapy:
📍Identify and treat subclinical CVD and cardiovascular risk factors 📍Optimize management of pre-existing CVD and cardiovascular risk factors 📍Perform targeted risk assessment to help inform cancer treatment decisions 📍Establish baseline cardiovascular function 📍Optimize primary prevention therapies 📍Plan cardiovascular surveillance during treatment
🫀Current tools include clinical assessment, biomarkers, 12-lead ECG, #EchoFirst, & risk scores
🫀Important evidence gaps includes cardiotoxicity mechanisms, impact of pre-treatment CV evaluations on clinical outcomes, validation&implementation of risk scores, & the role of AI.
Read more in @jaccjournals: https://t.co/cTCY0Acg99
#CardioOncology
Left Atrial Volumetric Enlargement in Heart Failure With Reduced Ejection Fraction: Obligatory Consequence or Independent Predictor of Outcome? | JACC: Heart Failure https://t.co/hH5D726cXa
🫀 #CardioNugget™
“Why is the cath gradient HIGHER than the echo gradient in AS?”
Think poor Doppler alignment first.
Doppler only measures velocity parallel to the ultrasound beam.
If the beam is not well aligned with aortic flow:
→ measured velocity is underestimated
→ gradient is underestimated even more
Delta P = 4v^2
Even a small drop in velocity causes a large drop in calculated gradient.
Example:
🔹 True velocity = 5 m/s → gradient = 100 mmHg
🔹 Measured velocity = 4 m/s → gradient = 64 mmHg
Clinical pearl:
➡️ When echo gradients are LOWER than cath, always reassess Doppler windows:
#EchoBoards #ASEcho #Cardiology