EM specialist, after all... reader, undiagnosticated ADHD, not-so-young-but-still-here free climber, coffee and protein bars (italian by birth, not my fault)
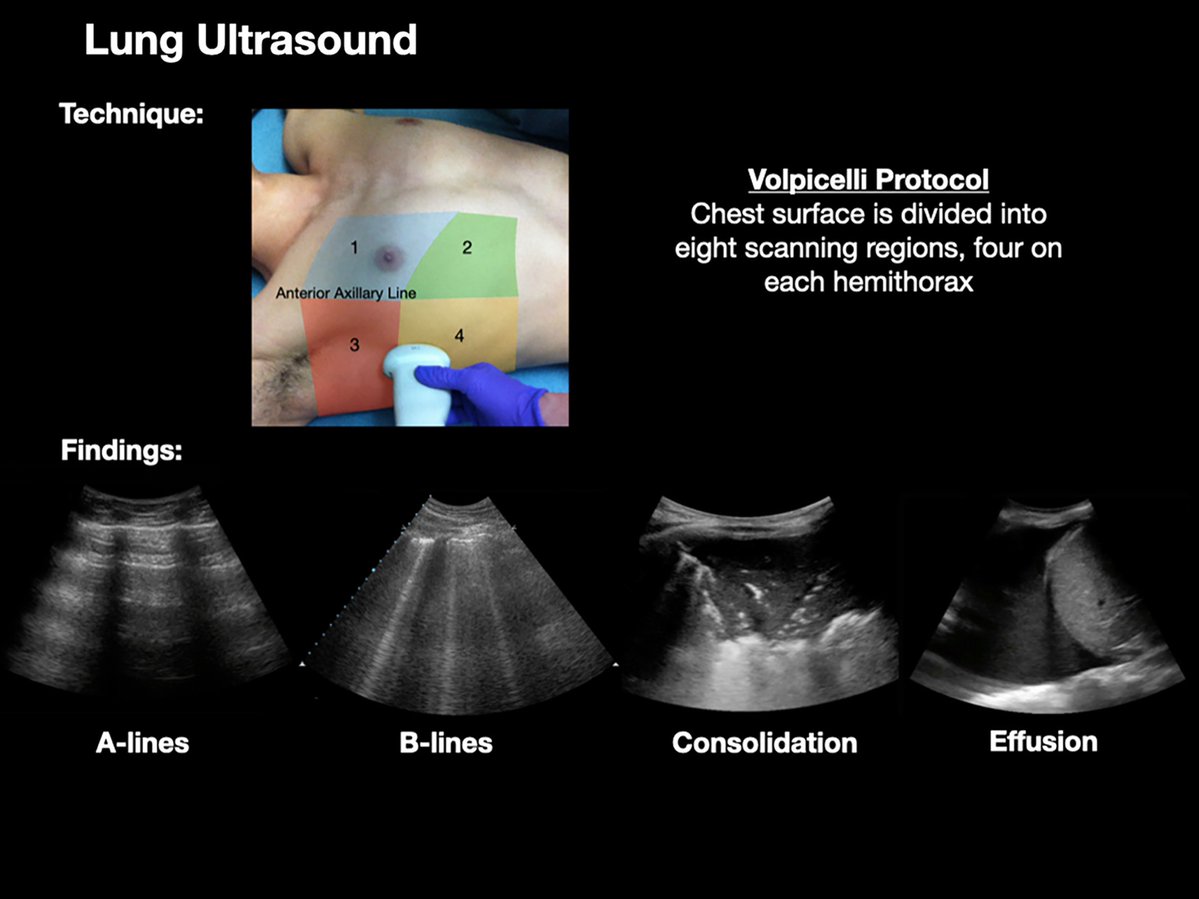
#POCUS review
🖊️"POCUS can be seen as an evolution of the stethoscope, perhaps bringing clinicians back to the bedside and providing time to build a therapeutic relationship while harnessing the advantages of technology"
🔗 https://t.co/TQfumvKW69
#MedEd#IMPOCUS#Nephrology
Acute variceal bleed + unstable vital signs = give blood products & get an emergency endoscopy
However, if the patient is stable & Hgb is >7, don’t transfuse
Quick reference on upper GIB in the ED: https://t.co/DQZerwURry
If you’re presented with a patient who is bradycardic and hypotensive after a calcium channel blocker overdose, you are going to be expected to initiate high dose insulin therapy as this is the standard of care in CCB OD
A secondary spontaneous PTX is considered stable if:
😮💨 RR <24
❤️HR > 60 and <120 beats per minute
💪 Normotensive
🌬️ SpO2 >90% on room air
🗨️ Able to speak in full sentences
Clinical features that define a BRUE include any of the following:
- cyanosis or pallor
- absent, decreased, or irregular breathing
- change in tone
- AMS
These occur for <1min & pt must be asymptomatic at the time of presentation
Free quick reference: https://t.co/OcTJWPaBrK
Bottom line:
Giving supplemental O2 to someone w/ severe COPD really *can* cause oxygen induced hypercapnea.
It occurs for three reasons:
1. Loss of hypoxic vasoconstriction --> worse V/Q matching (major reason)
2. Haldane effect
3. Decreased respiratory drive
15/15
This - the loss of hypoxic vasoconstriction to poorly ventilated lung areas - turns out to be the primary reason for oxygen induced hypercapnea.
https://t.co/f9XgY9gnn2
14/
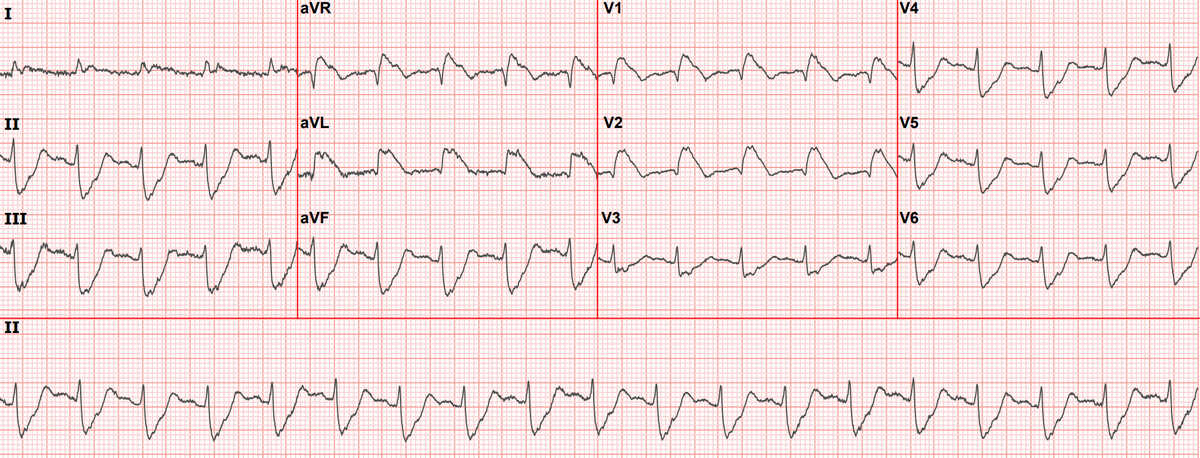
90 year old with acute chest and epigastric pain, and diffuse ST depression with reciprocal STE in aVR: activate the cath lab? @ECGcases
https://t.co/81CFXialMO