PRIME: Procedural Research and Innovation for Medical Educators. We aim to advance procedural research + education within Internal Medicine. R/T not endorsement
Hi #medtwitter! We’re #PRIME - a group of (mostly) Internal Medicine physicians dedicated to advancing procedural innovation, safety, and research.
Follow us for discussions around procedural technique; evidence updates, live Q&A, and more!
1/16
Why does cirrhosis predispose to "bacterial translocation"?
I have long heard that this is the mechanism of spontaneous bacterial peritonitis (SBP), but I hadn't understood why cirrhosis leads to more of it.
[Or where the bacteria translocate to...]
Let's have a look.
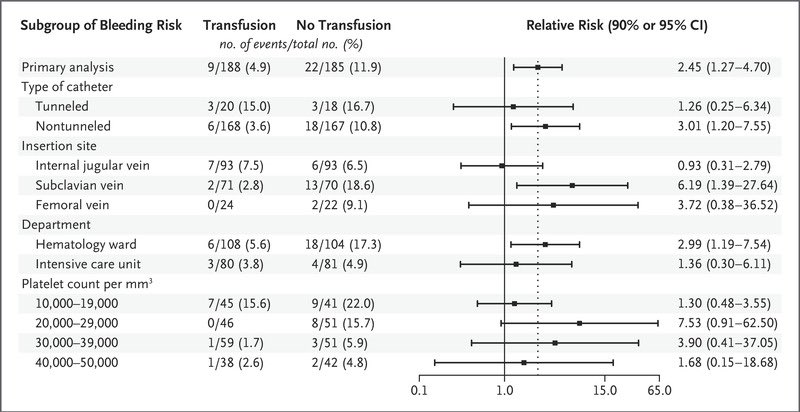
Interesting RCT in @NEJM about platelet transfusions prior to CVC placement in people w/ thrombocytopenia (Plt 10-50k):
- higher rate of grade 2-4 bleeding w/o Plt transfusion: 11.9% vs 4.9%
- difference driven by much more bleeding w/ subclavian lines
https://t.co/MwlDtLPxub
1/
#POCUS image of the day 📸
Classic example of rapid atrial swirl sign (RASS) - rapid opacification of right atrium after saline (preferably agitated but not necessary) injection. Positive test suggests correct placement of central venous catheter
#MedTwitter#Nephpearls#FOAMcc
Image courtesy: https://t.co/gRPhxWUVKK
@phlegmfighter@RabbleRouseED@ria_dancel Sure you can look solely based on time. You can also factor in the patients’ fear, anxiety, pain, inconvenience when having to reposition…
Ok team. Let's talk about this mysterious, pulsatile-appearing thing in the abdomen.
Many of you were concerned that this was a massive AAA 😱😱😱
And, to be fair, that was my first split-second reaction when I scanned the patient as well.
BUT!
@critconcepts They’re small arteries! I don’t have a good citation for the average velocity of flow; but lowering your Nyquist will only increase your sensitivity, and I’ve never run into trouble with excess signal. Will play around with different Nyquists and report back