Continues to amaze me, the lack of differentiation between a treatment and a supportive device. Brought to you by the same mode warring academics who know the words but not the physiology.
As I’ve said for years, in MV you have one job:
TO NOT WEAPONIZE THE VENTILATOR
La medicina se volvió tan románticamente explotadora… que ahora la raza joven ya no quiere “ponerse la camiseta” Y la neta, los entiendo. Porque una cosa es amar la medicina… y otra muy distinta es normalizar: hipertensión a los 38, divorcios por ausencia emocional,gastritis hemorrágica patrocinada por urgencias, lumbalgia degenerativa nivel Chernóbil y seguir haciendo guardias a los 55 años como si el cuerpo fuera un catéter Mahurkar eterno.
El verdadero problema no es que todos quieran derma. El problema es que las otras especialidades siguen funcionando como si el residente fuera un Nokia del 2003: indestructible y sin derecho a batería baja
@vallhebron@EduardArgudo@SimulacioVH@ONT_esp Ha sido una experiencia magnífica. Fantásticos docentes, grandes compañeros/as y alucinantes instalaciones @SimulacioVH. Nos llevamos muchas ideas para mejorar en nuestros hospital. Muchas gracias a Alberto Sandiumenge @EduardArgudo y demás docentes.
Proyecto ECMO de la SEMICYUC estuvo presente la semana pasada en Dublín en el #euroelso2026. Su coordinador, el Dr. @EduardArgudo, moderó varias mesas además de ser ponente en una sesión sobre la ECPR en diferentes sistemas sanitarios. También fueron ponentes y moderadores nuestros socios Ana Delgado, Ricardo Gimeno, María Martínez y Jordi Riera.
#medicinaintensiva #intensivistas #losprofesionalesdelenfermocrítico
You open ChatGPT. You type the question. A clean, structured answer comes back in three seconds. You read it, it makes sense, you move on. You feel like you learned something.
Forty-five days later, a professor walks in and hands you a test you weren't expecting. You don't remember most of it.
André Barcaui at the Federal University of Rio de Janeiro ran the experiment to find out if the feeling was accurate. 120 undergraduate business students, ages 18 to 24. All told to spend two weeks researching AI concepts, ethics, societal impacts, technical foundations, and prepare a 10-minute presentation.
Sixty used ChatGPT freely. Sixty used textbooks, library databases, articles, and standard web search. Then, 45 days later, with no warning, a retention test.
The ChatGPT group scored 57.5%. The traditional group scored 68.5%. Cohen's d was 0.68, a medium-to-large effect. In most grading systems, that's the difference between passing and failing.
This is called cognitive offloading. When your brain delegates thinking to an external tool, it reduces the mental effort required during encoding. Effort is what makes memories durable. Struggling to find, synthesize, and connect information is not an inefficiency in the learning process. It is the learning process. ChatGPT removes the struggle and takes the encoding with it.
Barcaui calls what the AI group experienced "borrowed competence." The answer was structured, the vocabulary was right, the reasoning felt sound. It just wasn't theirs. And 45 days later, it was gone.
The AI group's forgetting curve was steeper and didn't stabilize the way the traditional group's did. The memories weren't just smaller. They were more fragile from the start.
You didn't learn it. You borrowed it.
Delivering bad news as an ICU doctor is one of the harder parts of the job.
Here are some lessons I've learned along the way👇
1. Always sit down
2. Don't just jump into it. Spend the first couple of minutes with introductions to yourself, your team (if present), but more importantly who all is in the room (patient, family etc.)
3. If you will be needing consent for something (procedure, palliation etc.) as part of the discussion, ensure you know who the decision maker(s) are.
4. Preface the bad news "I have to share something that might be hard to hear"
5. Clearly in <30 seconds deliver the bad news then STOP TALKING.
The biggest mistake I see is people give the news and keep going. It takes time to process what may be the worst news they've ever received. Silence is the solution here. They will talk or ask questions when they are ready... it could be 10 seconds, 1 minute, or 10minutes. Give them the time they need before you proceed.
6. Ask if they have any questions about what you have delivered.
7. Be prepared to answer 'what comes next' ..
8. Ask about spirtual / religious beliefs when appropriate and offer support if that is available.
9. Let them know you or someone from your team will be available to answer questions that might come to mind... often in the moment, questions slip people's mind but come to them minutes after you leave. Make sure they know how they can have them clarified.
Just some thoughts here... any others?
Bonus: Don't construe family members becoming angry as them being angry at you or the team. Anger when faced with this news is common, normalize it and realize it likely isn't directed at you!
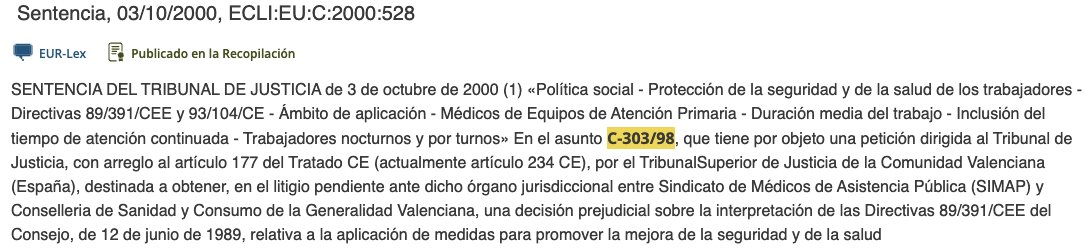
🕵️♂️ La Estafa de la Guardia nació el 03/10/2000.
El Tribunal UE (Caso SIMAP) soltó la bomba: "La Guardia ES tiempo de trabajo".
Pánico en el Estado: Si eran horas reales, violaban el límite legal y el sistema quebraba.
¿La solución? Un crimen administrativo 👇
@tommy_chav 😁👍🏻 Además: 1. La R a PTZ no se da en todas las AmpC, puede haber expresión baja y salir S. Poco probable con 2 días de tto 2. Prácticamente todas las AmpC son S a cefepime. 3. RC 3 en el MIR, incorrecta en la vida real: no hace falta usar un antipseudomónico (ertapenem mejor)
‼️ Sobre las guardias médicas y el borrador del Estatuto Marco que quieren aprobar la ministra Mónica Garcia y los sindicatos que tienen una representación minoritaria o nula entre los médicos como CCOO, UGT, CSIF o SATSE:
🔴 Las guardias siguen siendo obligatorias hasta los 55 años
🔴 La hora de guardia se podrá seguir pagando peor que la hora ordinaria
🔴 Las guardias de días festivos seguirán siendo de 24 horas “voluntariamente”
🟠 Las guardias de días laborables seguirán siendo de 17 horas pero sin trabajar la jornada ordinaria (única mejora objetiva y real aunque suponga seguir trabajando 17 horas seguidas)
🪧 Por estas y por otras razones la huelga médica continuará los días 14 y 15 de enero.
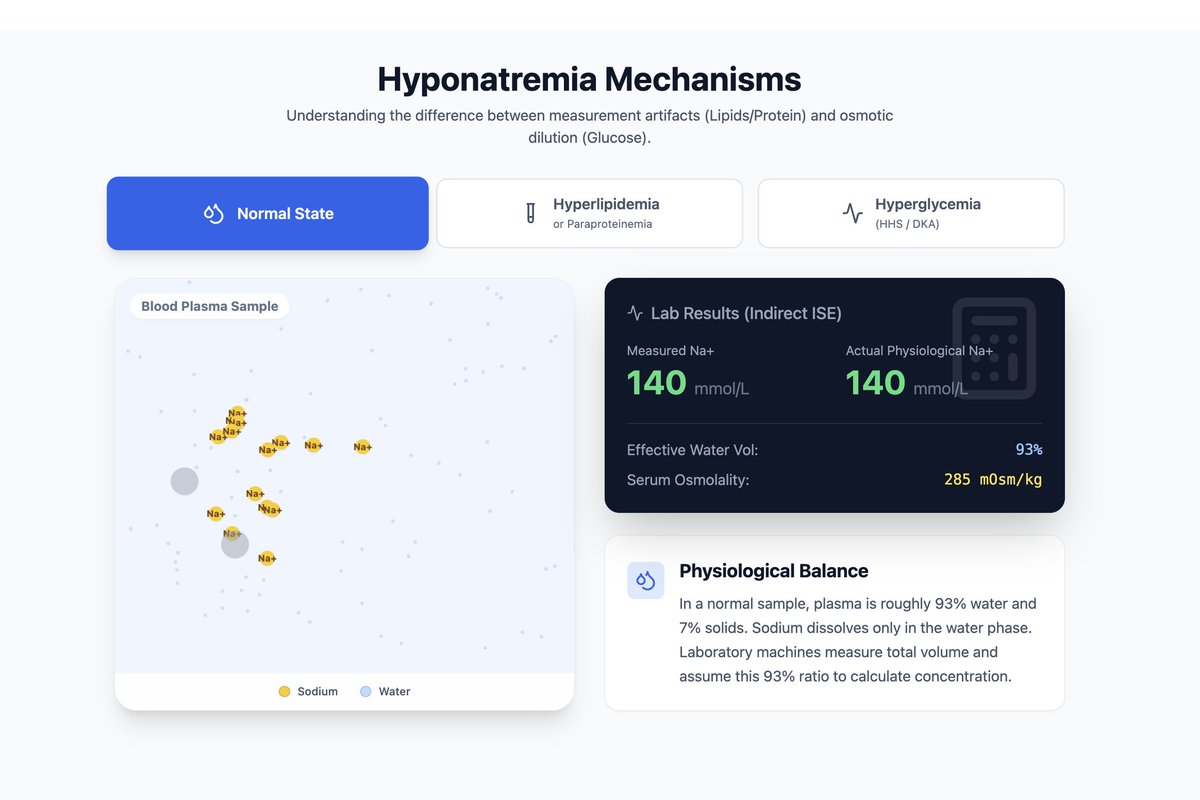
'Pseudohyponatremia' due to hyperglycemia is REAL hyponatremia which gets better when you fix the glucose
'Pseudohyponatremia' due to elevated lipids or protein is NOT real hyponatremia. The lab tells you the sodium is low but there is no true hyponatremia
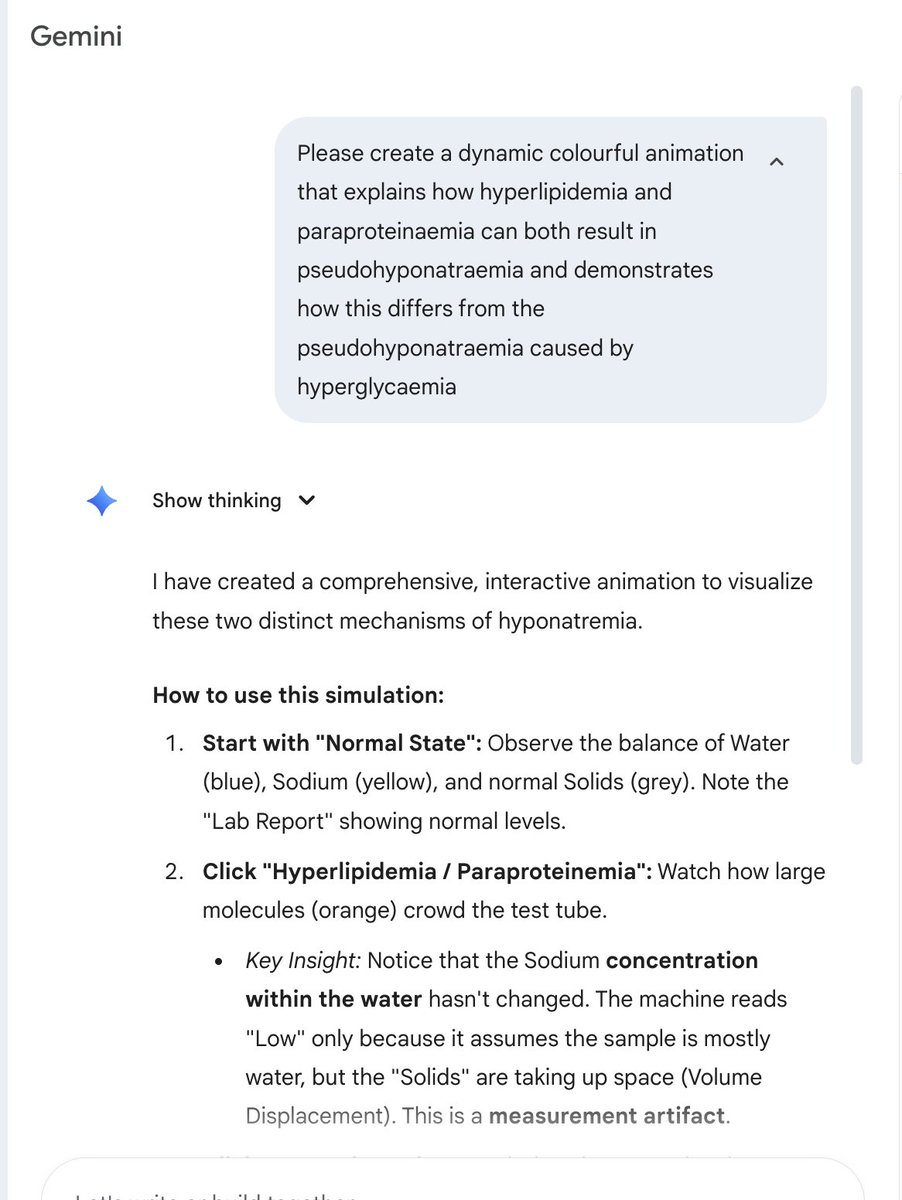
I made this animated graphic using the latest Gemini AI model with a single simple prompt that explains the difference nicely
https://t.co/GgYcX9BTG0
@cliffreid Excelent! And blood gas analizers dont suffer this artifact (direct ISE technology) so for real Na levels just check the ABG and forget the lab. For the same mechanism ICU patients with severe hypoalb could have pseudoHIPERnatremia.
@ehlJAMA Ohhh very glad to hear that BUT >90% of recents cardiology trials (included those published in JAMA) used composite outcomes just like this one, leaving to questionable changes in guidelines recomendations @drjohn
In honor of Dr. Robert Bartlett’s passing, here is the first ECMO patient, Esperanza Pineda, both on ECMO shortly after birth in 1975 and at age 44. She is now 50.