Honored to share our latest manuscript in Circulation highlighting important advances in cardiovascular imaging and care.
Special thanks to our imaging faculty, @SNagueh , for his continued mentorship and support.
URL: https://t.co/CqcknkvGir
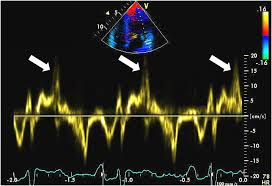
@PWesslyMD@LucySafi@PriyaPanday27@NadeenFaza@ASE360@JournalASEcho Prolapsing valves pull on chords/papillary muscles, stretching the LV wall inward. This causes "curling" (LV crest rotates posteriorly) & the Pickelhaube sign -- a sharp late-systolic S’ wave >16 cm/s on TDI. Both are markers of increased arrhythmia risk! #ASEchoJC
🚨Manejo contemporáneo de la Insuficiencia Cardíaca Aguda. 🫀💦
✔️La hospitalización ya no debe verse solo como una fase de “descongestión”, sino como una oportunidad para modificar la historia natural de la enfermedad. 🧐📈
✔️La ICA sigue asociándose a alta mortalidad y rehospitalización. El tiempo al tratamiento importa: reconocer y tratar temprano mejora desenlaces.
✔️BNP <100 o NT-proBNP <300 prácticamente descartan ICA.🔎
✔️El tratamiento inicial debe enfocarse en: O² si SatO₂ <90%, diuréticos IV tempranos, vasodilatadores IV si PAS >110 mmHg, identificar causas reversibles (SICA, arritmias, infección, valvulopatía, TEP, etc.).🎯
✔️La respuesta diurética debe evaluarse en las primeras 2 horas: diuresis >300 mL, Na urinario >70-80 mmol/L, si no se logra → duplicar dosis y considerar terapia secuencial.💦
✔️La hospitalización es el mejor momento para iniciar o intensificar tratamiento modificador de enfermedad (los 4 pilares ya!). 💊💊
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 👌🏻
https://t.co/xjS6PwznZu
https://t.co/CYXglmP4a5
1/8
🚨 The results of CLOSURE-AF are in, providing a sobering look at Left Atrial Appendage Closure (LAAC).
This was the first trial to test the device against modern DOAC therapy in the high-risk patients seen in daily practice.
The verdict: LAAC failed to meet non-inferiority
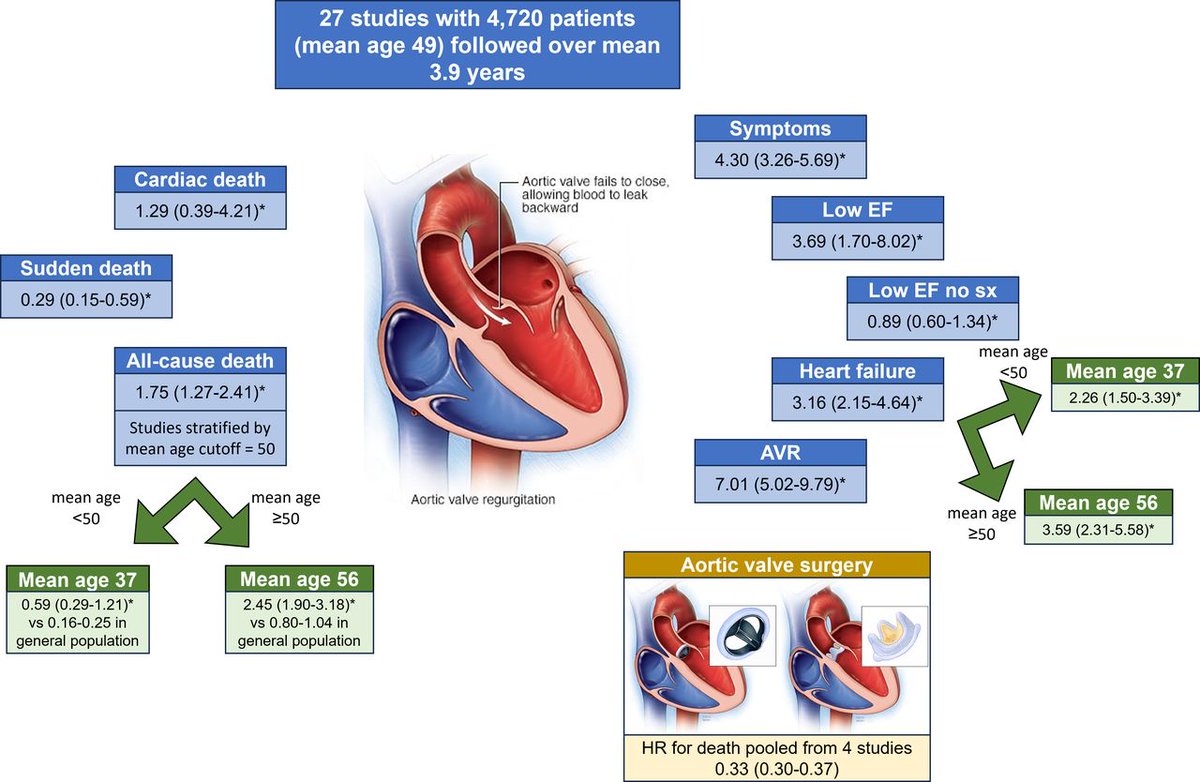
Natural history of asymptomatic moderate or severe aortic regurgitation: a systematic review and meta-analysis
Please read the article and enjoy an in-depth interview between @jhfrudd and the first author, Dr Jwan Naser from The Mayo Clinic in Rochester, Minnesota, USA
Paper: https://t.co/fxWs0bkEiv
Interview: https://t.co/ZGhyrExOAf
#EHJCVI 🫀 A paradigm shift in endomyocardial biopsy? #WhyCMR LGE can be transformed into a patient-specific 3D roadmap to guide biopsy 💉 Targeted EMB directly impact therapeutic decision-making, including immunosuppressive treatment ❤️🔥 Read more ⏩ https://t.co/qUBi5uNUqC
🏃♂️ Elevated troponin after exercise… should we worry?
💥 Cardiac troponin = gold standard for myocardial injury.
👉 But what happens after intense exercise?
📊 A large meta-analysis (129 studies, >7,000 athletes) shows:
➡️ 36% of athletes have troponin levels above the normal limit after exercise
⚠️ That’s more than 1 in 3.
🔬 Key determinants (see Graphical Abstract, page 3):
✔️ High-sensitivity assays → detect more elevations
✔️ cTnT > cTnI
✔️ Peak in endurance sports (running, cycling, triathlon)
✔️ Highest after 3–6 hours of exercise
📈 The curve on Figure 4 (page 29) shows a clear peak around 4–5 hours of effort.
👀 What DOESN’T matter (as much as we thought):
❌ Sex
❌ Training status
👉 It’s not about who you are…
👉 It’s about what and how long you do.
🧠 Clinical dilemma:
Troponin ↑ = myocardial injury
BUT
Exercise alone can cause it
👉 So… how do we interpret it in the ER after a marathon?
💡 Take-home message:
🩺 Context is everything
👉 Consider exercise type, duration, and assay used
👉 Not every troponin rise = pathology
🚀 This is a perfect example of why biomarkers need clinical interpretation, not just thresholds.
#Cardiology #SportsCardiology #Troponin #Biomarkers #Endurance #ExercisePhysiology #CardioImaging #PrecisionMedicine #Athletes #Research 🏃♂️🧬
#CardioNugget
Pickelhaube sign = sharp, high-velocity systolic spike (>16 cm/s) on tissue Doppler at the lateral mitral annulus 🪖
Seen in mitral valve prolapse → reflects sudden systolic annular recoil
⚠️ Red flag for arrhythmic MVP & ↑ risk of ventricular arrhythmias/SCD
#EchoBoards #Cardiology #MedEd
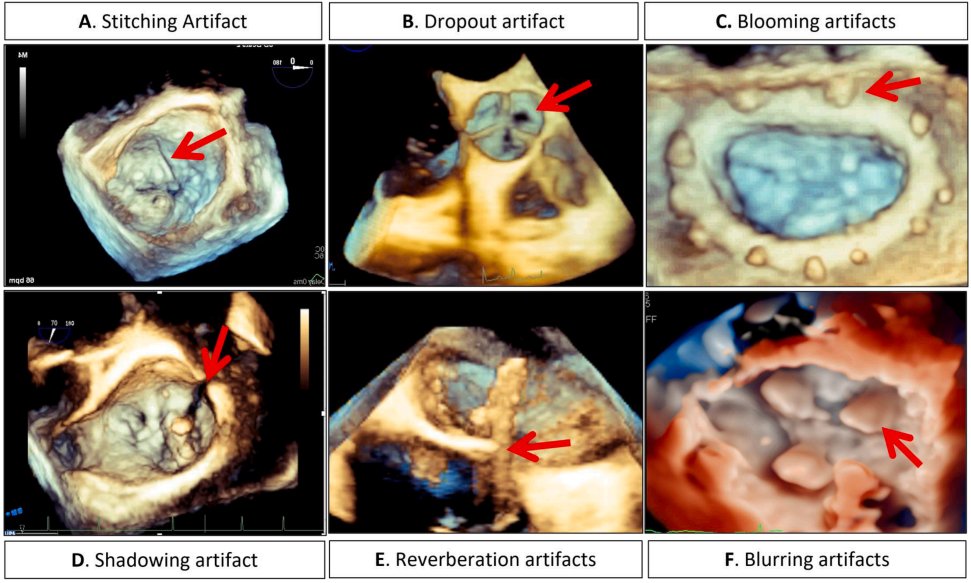
🫀NEW GUIDELINE🫀
Read our newest #ASEGuideline, "Recommendations for the Identification and Mitigation of Cardiac Ultrasound Artifacts!" https://t.co/wST56DL1ZH
🚨 HOT OFF THE PRESS! 🚨
New guidance from the American Society of Echocardiography @ASE360 for Cardiac Ultrasound Artifacts 🫀📡
➡️https://t.co/UB6Pz1H5NV
👉 A must-read for everyone in #EchoFirst!
🔍 What is an artifact?
➡️ An imaging feature that does NOT reflect true anatomy/pathology
➡️ Common, expected, and rooted in ultrasound physics ⚙️
💡 Why this matters
⚠️ Artifacts can mimic disease → misdiagnosis → inappropriate management
⚠️ Present across ALL modalities:
• 2D 🖥️
• Spectral Doppler 📈
• Color Doppler
• 3D echo 🧊
📘 What this guideline delivers
✅ Standardized, structured approach to artifacts
✅ Clear explanation of:
• Appearance 👁️
• Mechanism ⚙️
• Clinical impact 🏥
• Real-world cases 🧾
• Mitigation strategies 🛠️
🧠 Also covers
🔹 “Artifact-like” phenomena
🔹 Interference from external devices & equipment 📡
🎯 Key takeaway
👉 Artifacts are inevitable—but misinterpretation is not
👉 Mastering them = safer, smarter echo practice
👩⚕️👨⚕️ Who should read this?
➡️ Sonographers
➡️ Cardiologists
➡️ Trainees
➡️ Anyone interpreting cardiac ultrasound
📢 Elevate your imaging game. Recognize. Understand. Mitigate.
#CardioX #Cardiotwitter @JournalASEcho #ACCFIT
#EHJCVI 🫀 Time to refine #echofirst quantification of aortic regurgitation? 🔍 Using #whyCMR as reference, a 2-step TTE algorithm (RegVol≥45 mL + LVEDVi≥93 mL/m²) outperformed traditional criteria for severe AR definition‼️ #VHD ⏩Read more: https://t.co/g7xUAkbhOM
Curious about #CVImaging 💓 Read 'Multisequence cardiac #WhyCMR tissue characterization of cardiac masses: a retrospective cohort study🌟 by Vallurupalli et al. in #IJCVI.
https://t.co/1ACl0yWqNi
#EHJCVI 🧲 MRI reveals what wall thickness alone can miss 📏 Wall Thickness SD (WTSD) identifies both overt and early hypertrophic cardiomyopathy, even before hypertrophy is evident 🔍✨Read more 👉 https://t.co/gRqkbeIXKc
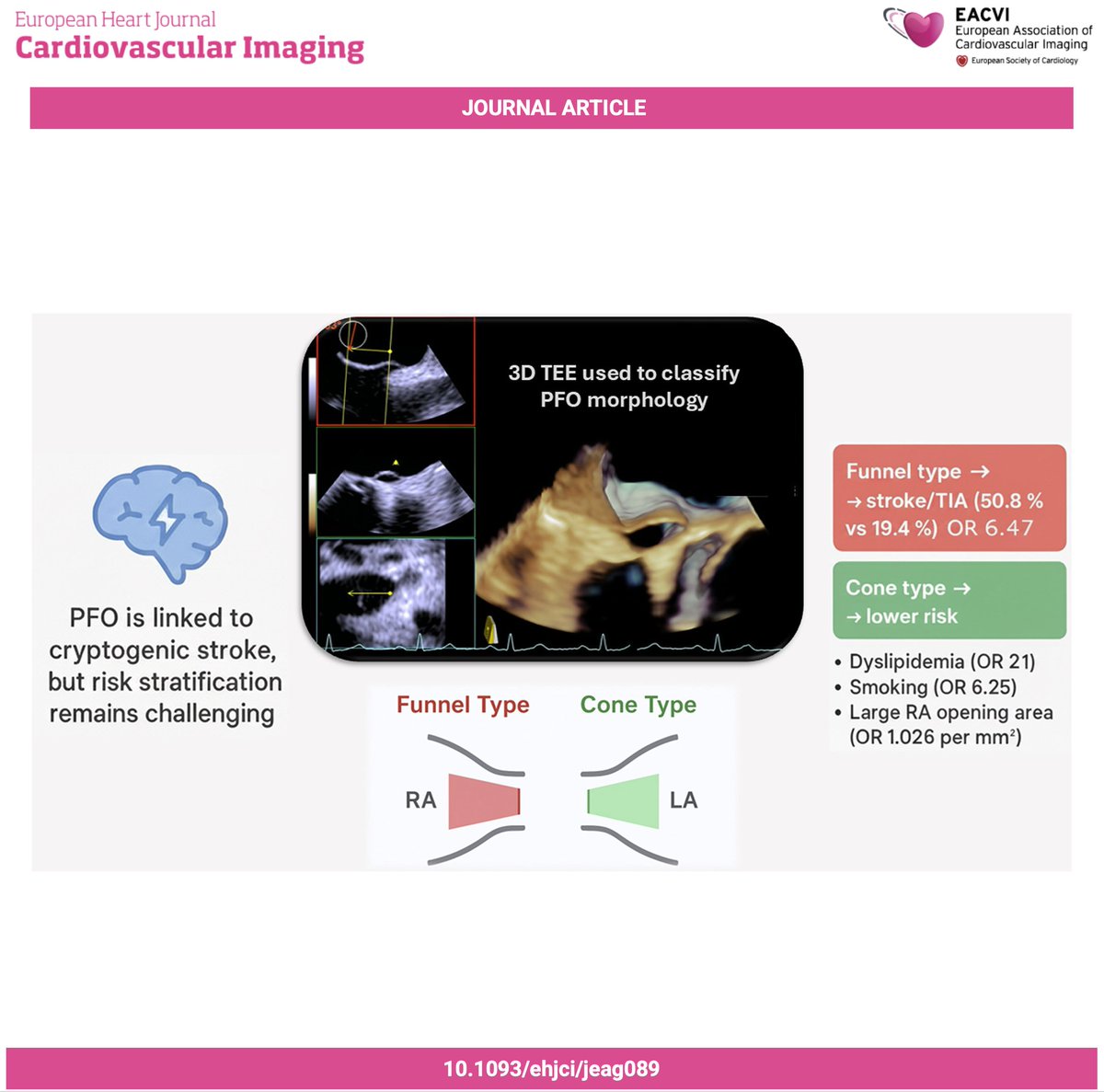
#EHJCVI 🔍 New insights into PFO risk. Totaro et al. identify “funnel-type” PFO morphology on 3D-TEE as a novel high-risk feature 🧠📊 Read more 👉 https://t.co/V9ijxSuz5J
#EHJCVI 🫀 Scar is more than just the presence of LGE on #WhyCMR 💡 In this study with >400 #HCM patients, scar composition and border-zone channels predicted arrhythmic events and improved ESC and AHA/ACC risk models ‼️ Read more: https://t.co/Nn7hfOqCkQ
#EHJCVI 🫀 Mixed aortic disease is a hemodynamic challenge and an #echofirst dilemma! In this large Korean cohort, moderate aortic stenosis + regurgitation carried a risk of cardiac death and HF hospitalization comparable to severe AS ‼️ Read more: https://t.co/jGUHsryh87