🚨 Exciting news! Application for the 2025 SABI-ECC team is now OPEN! 🚀
@rgrasmus & I invite you (trainees! junior radiologists in practice!) to apply or reapply for roles that inspire you.
Deadline: Jan 18th!
🔗 https://t.co/xLzsfT0wk2
#SABI2025@SABImaging
Our upcoming webinar will be a great opportunity for current #radres to learn the challenges and potential solutions to developing/nurturing academic endeavors and maintaining a sense of professional fulfillment. Register today! #radtwitter#radxx
https://t.co/ds4HhAo5cN
@EmmaradMD @nellytanmd More intricate & patient oriented than 280 characters, but many @UTSWUrology utilize it for T1a masses where (for appropriate patients) ccLS1-2 would undergo active surveillance (for more likely indolent subtype), ccLS3 undergo biopsy, & ccLS4-5 undergo partial nephrectomy
@francisdeng @nellytanmd Likely from ccLS 2 being underpowered relative to others in the multi center study (ie 21 ccLS2 vs 99, 145, 124, 111 for ccLS 1, 3-5 respectively). Also mri protocol not standardized across institutions (ie lower flip angles on DIXON less sensitive for microscopic fat)
@swoo_rad @nellytanmd Ideally in the future there will be more knowledge about cancer radiomics-genomics correlation that may help personalize neoadjuvant therapy in advanced cases
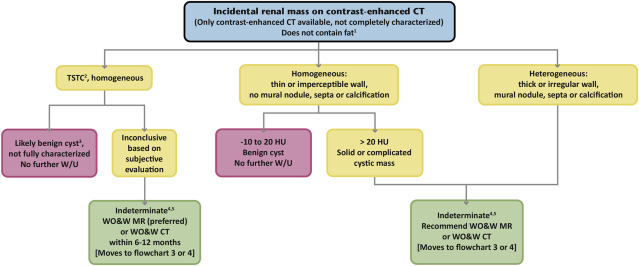
@JacobFlemingMD@becker_rad See ACR incidental findings paper (https://t.co/qa9kZFI4Ox). TSTC when size is less than twice the slice thickness (https://t.co/zh1Dbz5g9l). Still, if clearly fat density, call it an AML. If clearly fluid density range, likely benign cyst. Otherwise indeterminate