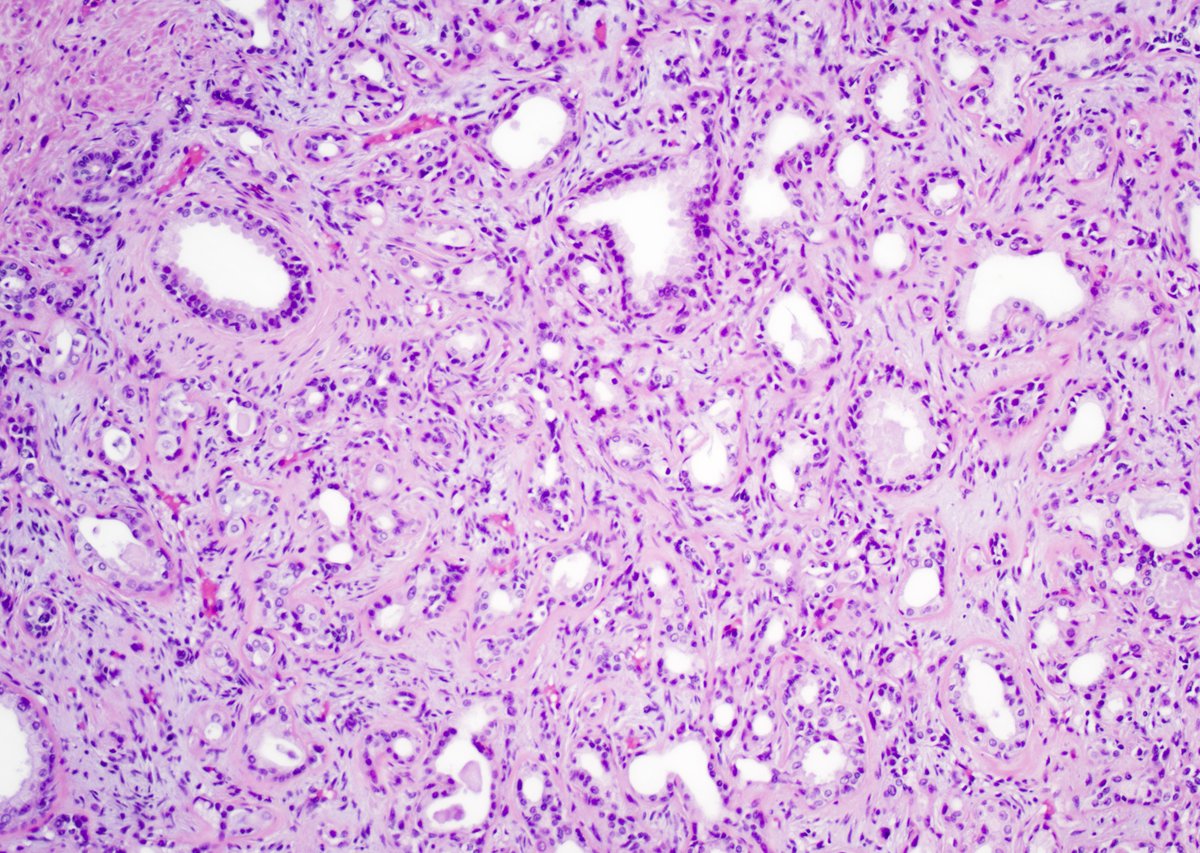
What is your diagnostic criteria for cribriform Prostate cancer?
Experts can disagree with what is cribriform. Here is cancer without basal cells (pin4 not shown). Looks cribriform to me.
https://t.co/kbdIrHbfua
#pathology@slusagar#standardization
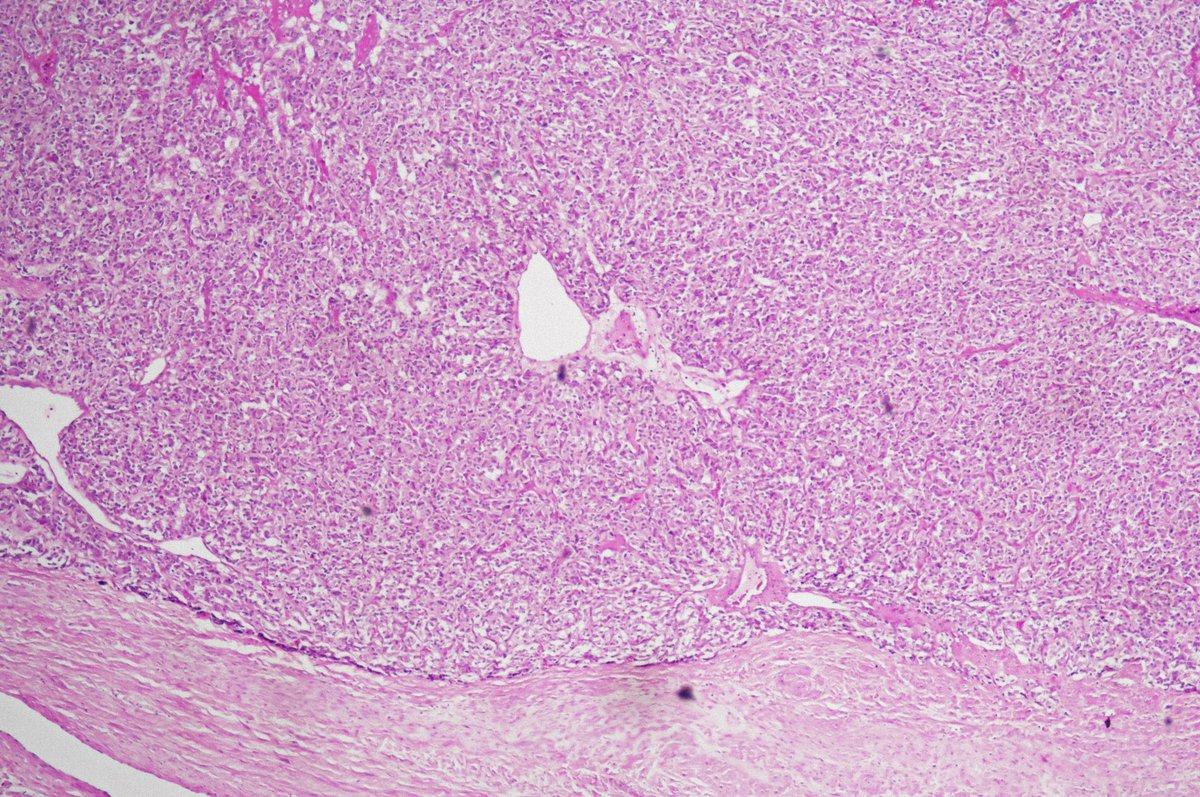
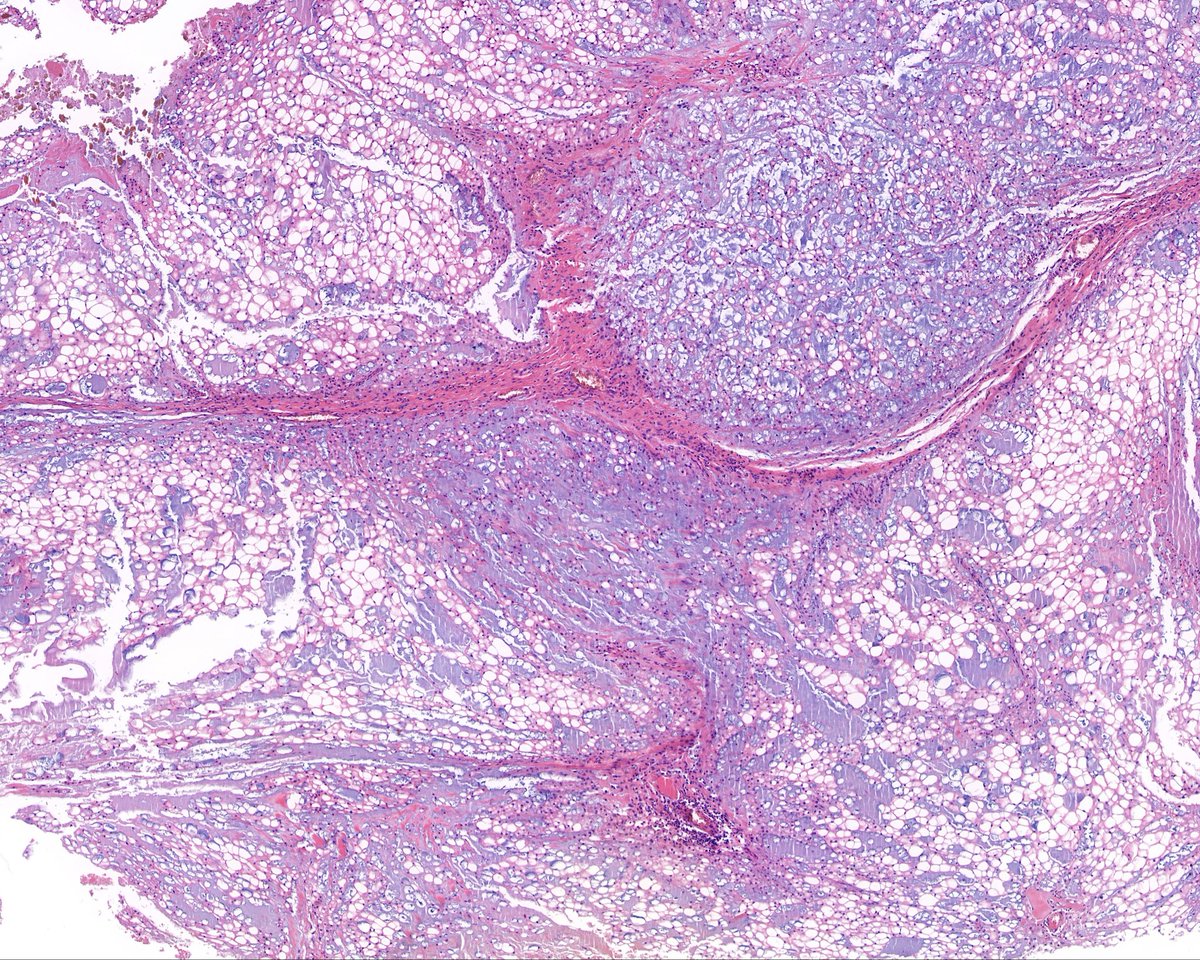
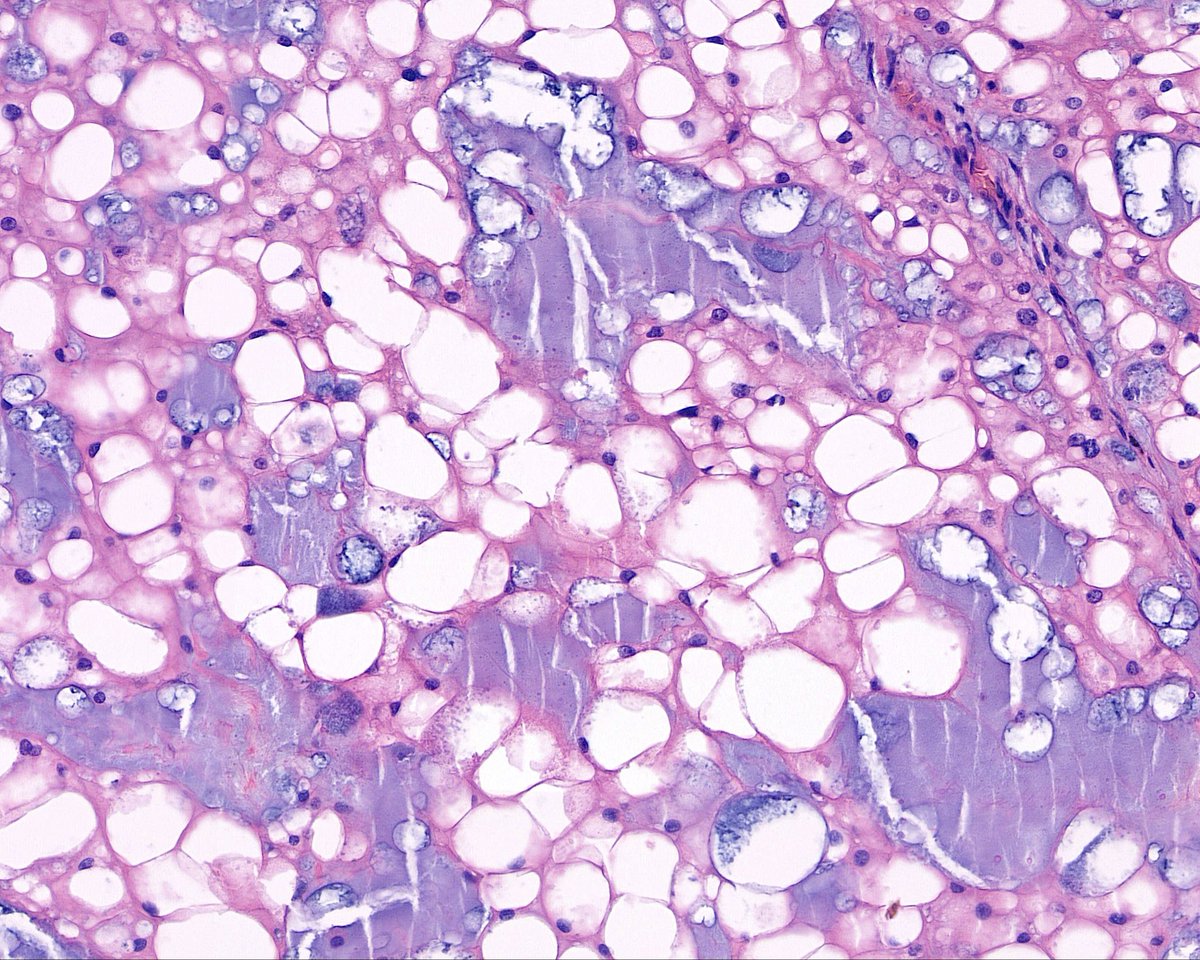
✅ Low-grade Oncocytic Tumor 🎯🧬
• Solid growth of oncocytic cells with uniform, bland nuclei lacking prominent nucleoli or nuclear wrinkles
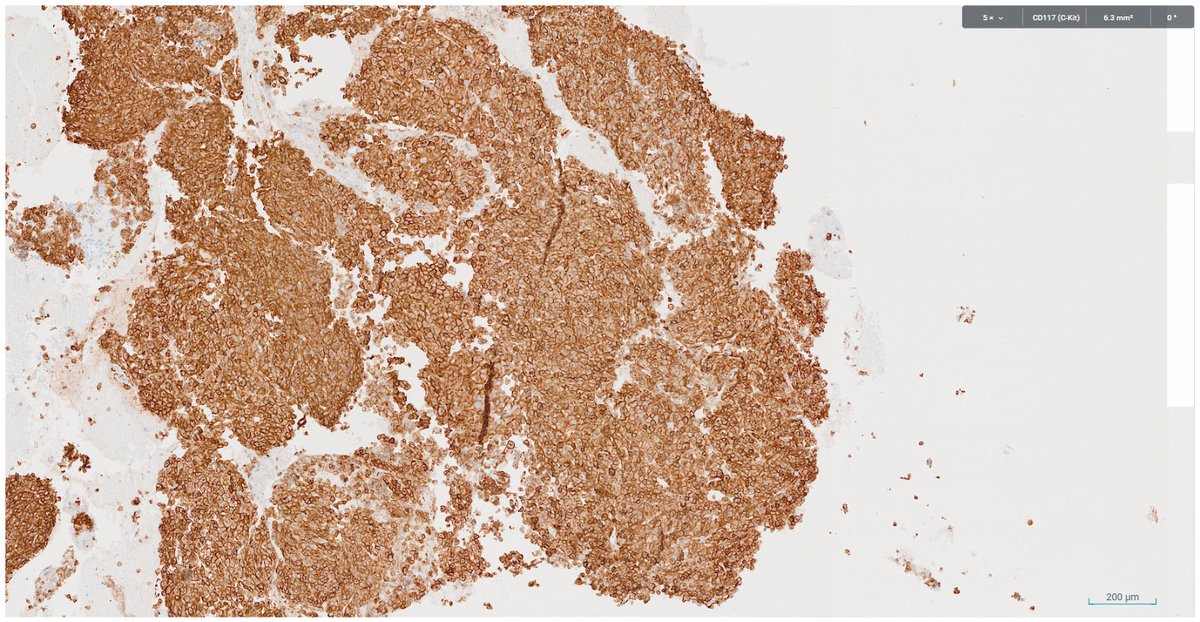
• Distinctive IHC profile: strong and diffuse CK7 positivity, while KIT is often negative or only focal
• Driven by mutations in genes of the mTOR pathway, particularly TSC1, TSC2, or MTOR
• Recognizing this newly defined entity is crucial, as it behaves in an indolent manner and overlaps with oncocytoma/ChRCC
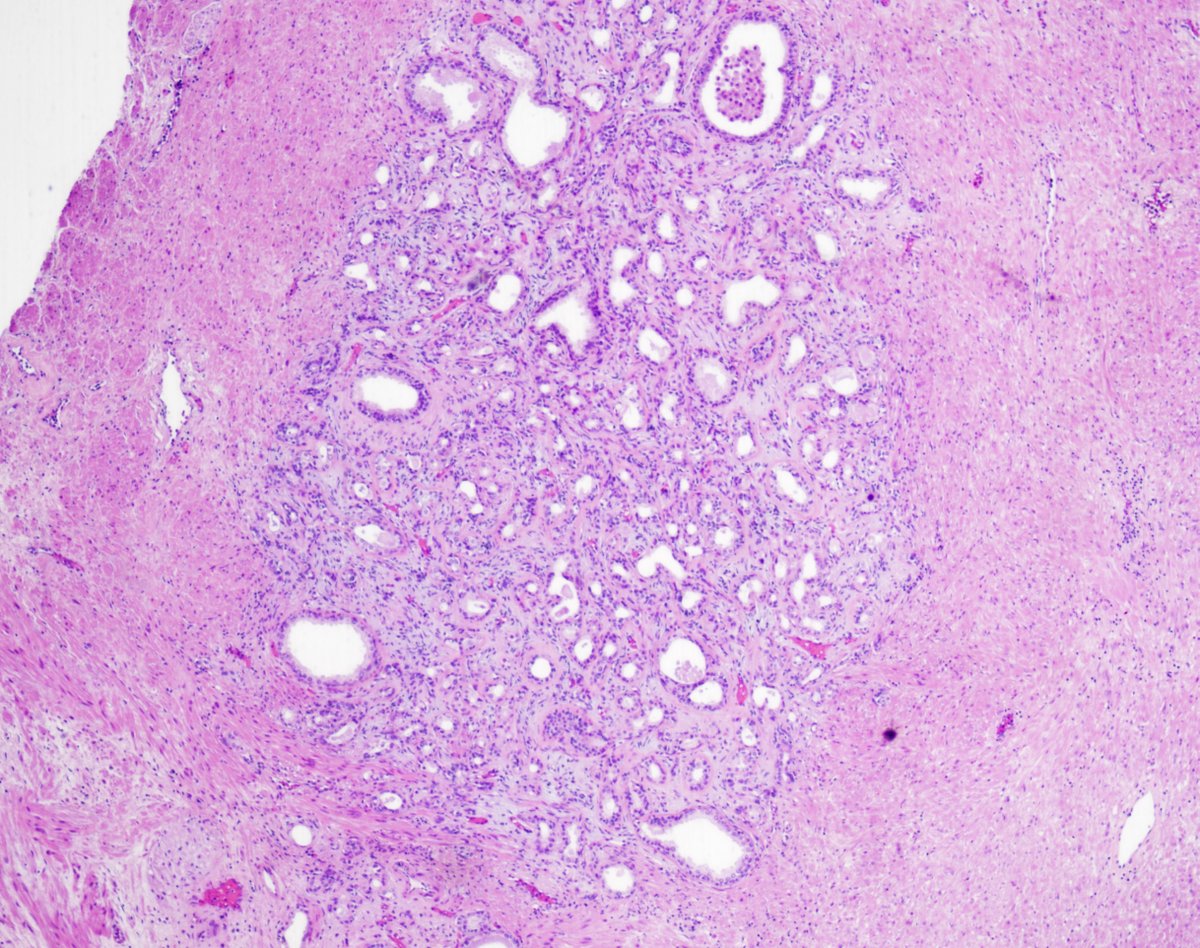
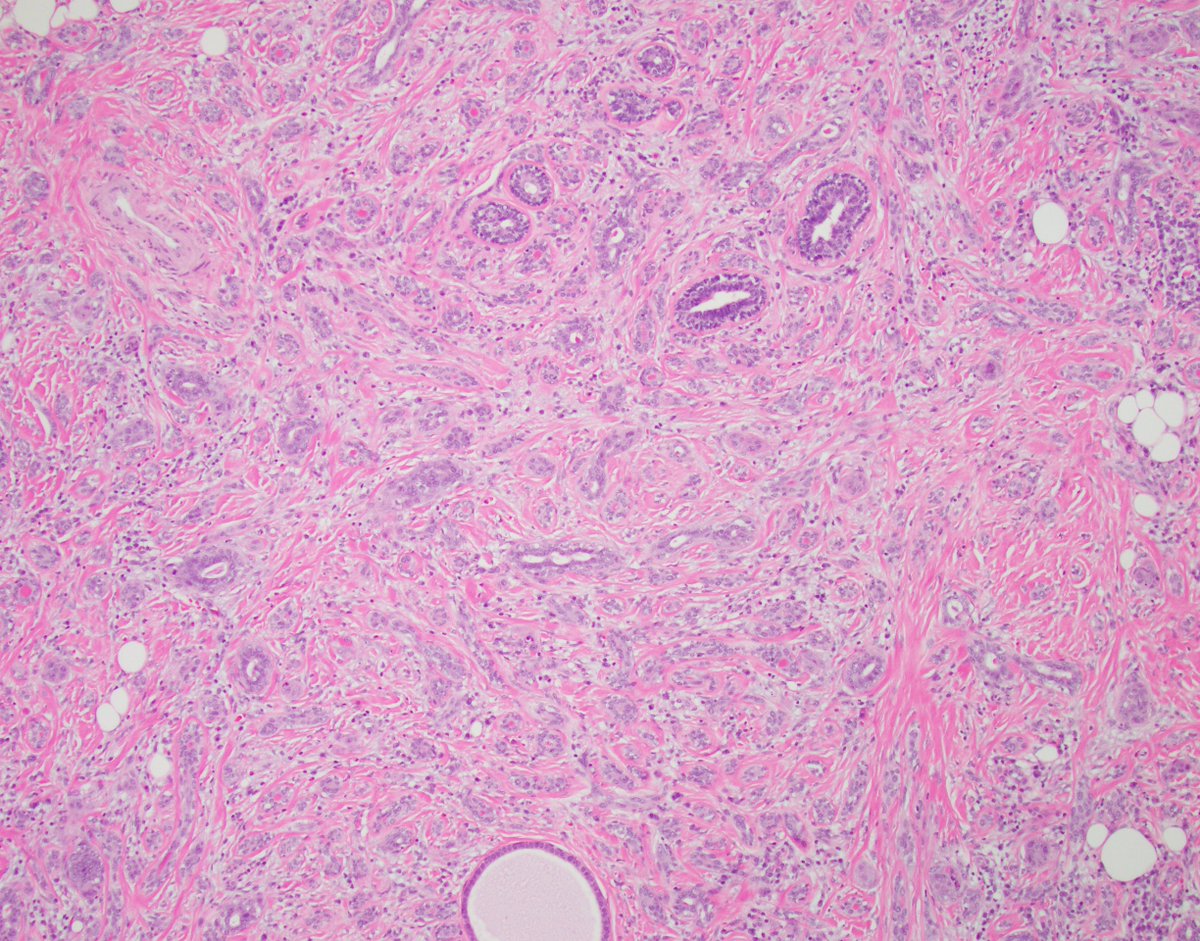
Pitfalls of p63: Case 3
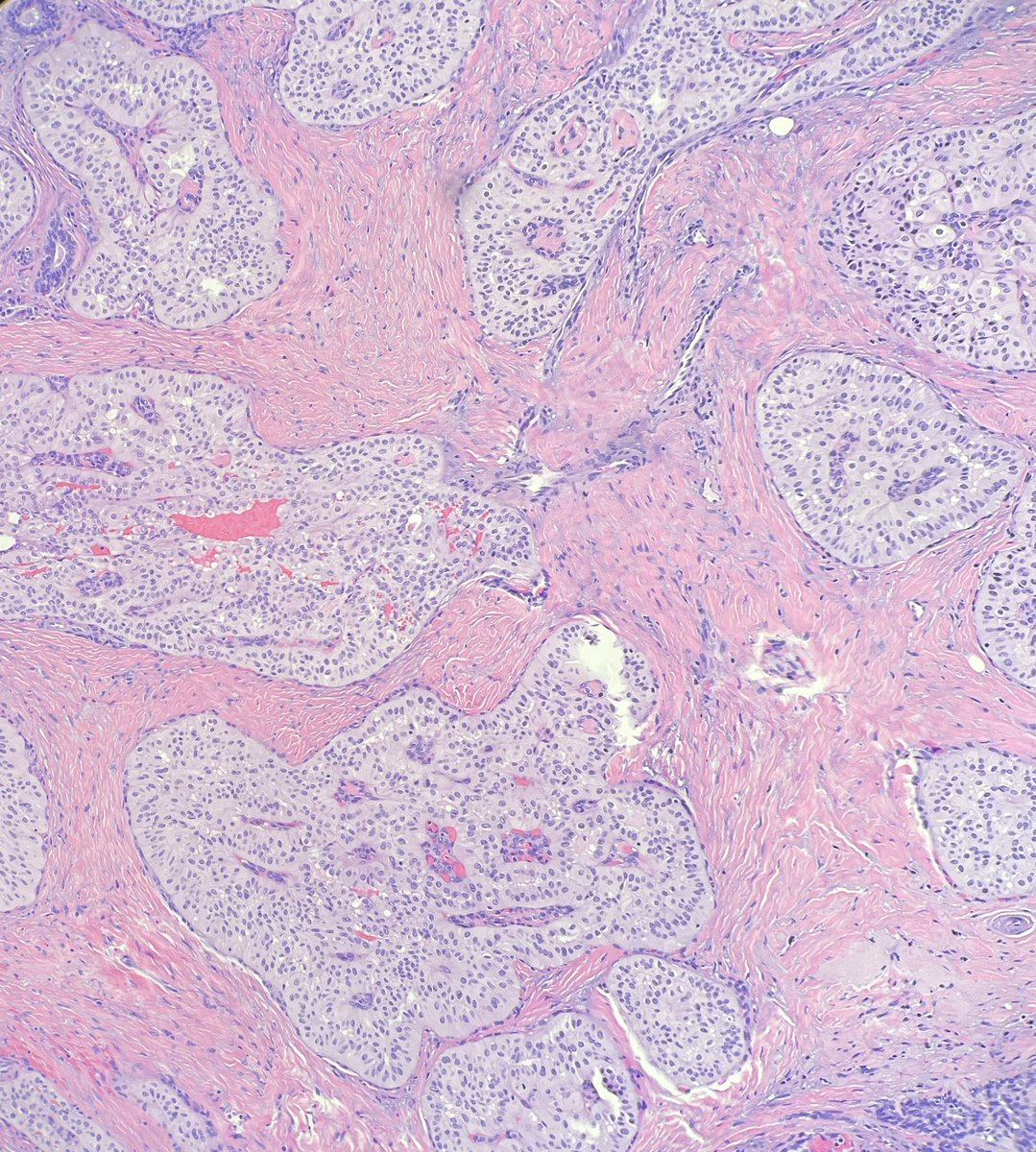
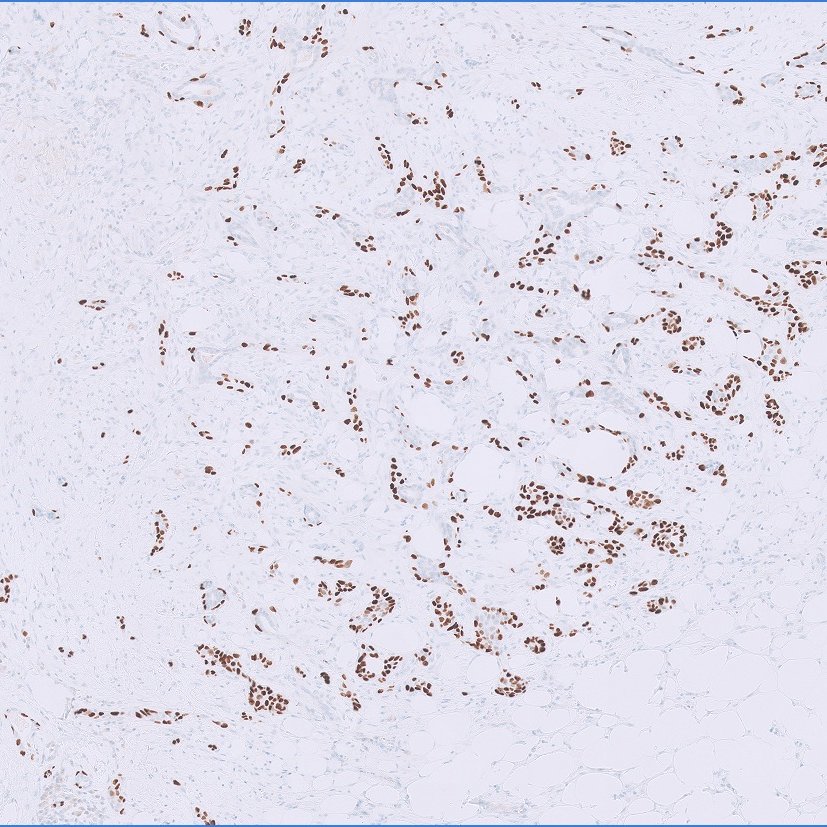
This is a spiculated mass detected on imaging. Again, p63 was performed, likely because of the fibrous background and the cribriform features, and it showed positivity.
What is your diagnosis?
@washu_pathology@washupathedu#breastpath#PathTwitter #PathX
Happy Friday everyone!
Let's tackle our Breast Consult Case of the Week 5 #BCCW#breastpath
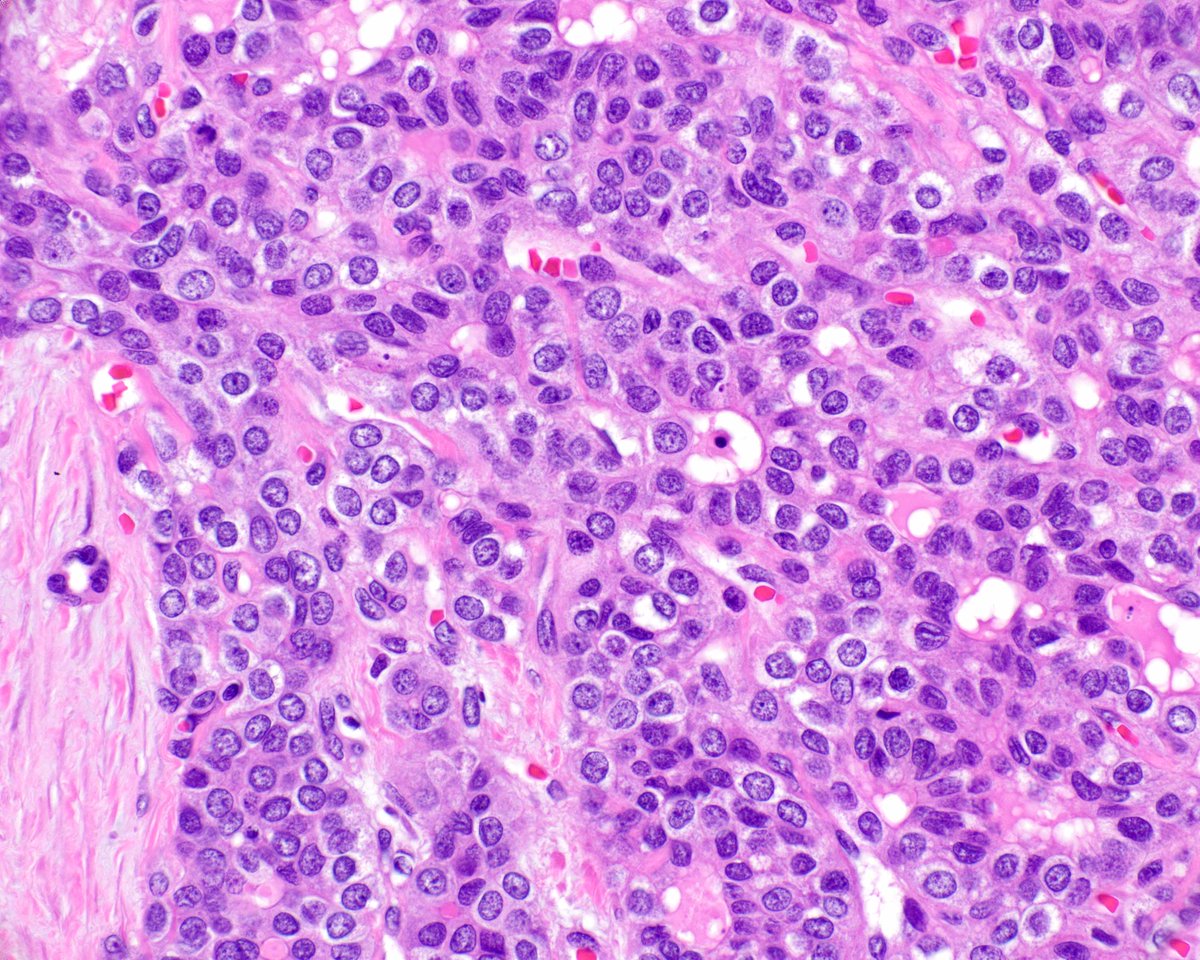
This one is a bit of a head scratcher because of incongruous cytology and architecture.
First of all, we have what appears to be a proliferative lesion with a population of uniform cells involving multiple spaces, which sounds like a very good definition for an atypical/neoplastic proliferation. The confusion here is that the cytology is predominantly columnar, if not tall columnar, and the pattern of involvement is pagetoid (you can see the flattened layer of residual native epithelium lining the luminal aspect of the proliferation).
Pagetoid involvement of spaces is typically seen with lobular neoplasia and higher grade examples of DCIS, while the worst columnar cell proliferation we know of is columnar cell hyperplasia with atypia, which this isn't.
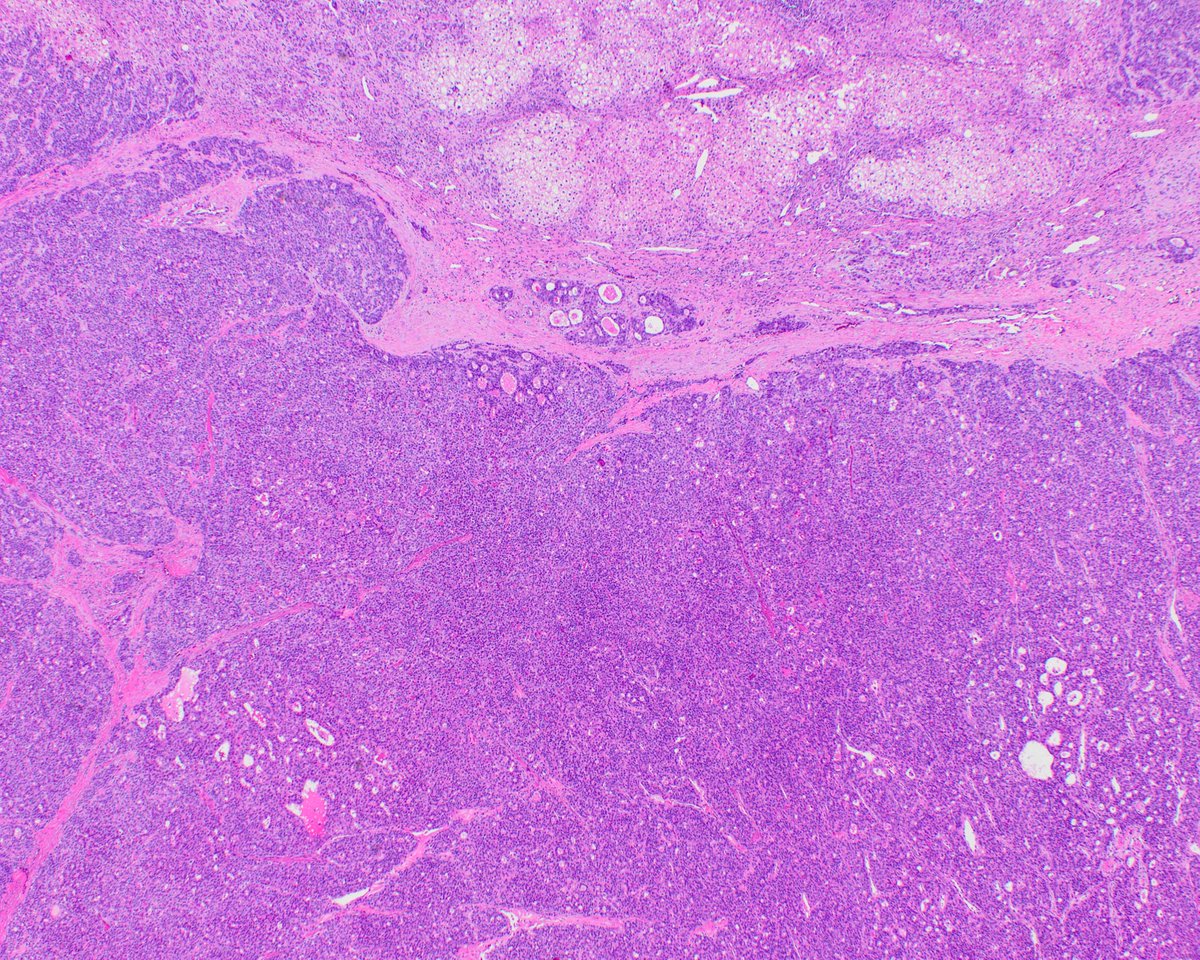
In other words, this is an atypical columnar cell proliferation growing like a D/LCIS. Though I do not claim to have an answer to this diagnostic conundrum, I believe the pattern of growth and involvement of multiple contiguous spaces by a seemingly clonal population of cells in a pagetoid pattern should dictate what we call this, which is why I called it DCIS. Granted, not all DCIS cases are created equal, and one might argue that this columnar pattern of DCIS may carry a smaller risk than classic examples of low grade DCIS, just because the cells are "less abnormal". So I would not be opposed to calling this ADH, though a diagnosis of ADH is essentially inaccurate because this is not ADH by strict diagnostic criteria.
Finally, I would not go down the LCIS route because the cells are columnar, which means that their cellular scaffolding is robust, unlike the plasmacytoid cells of lobular neoplasia that suffer from a disrupted internal architecture.
That's all. Such cases with unclear diagnoses make us think more intently about our criteria and understanding of the neoplastic processes of mammary epithelium.
See you all Monday for BCCW 6!
@washupathedu@washu_pathology #PathTwitter #PathX
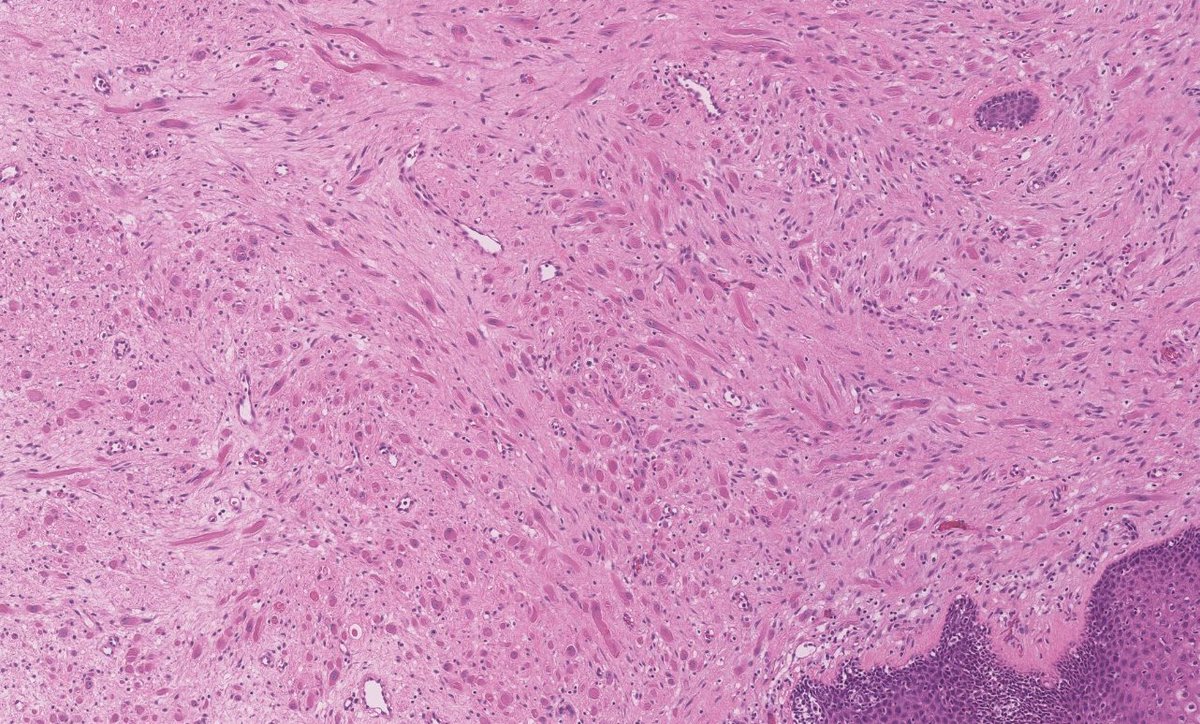
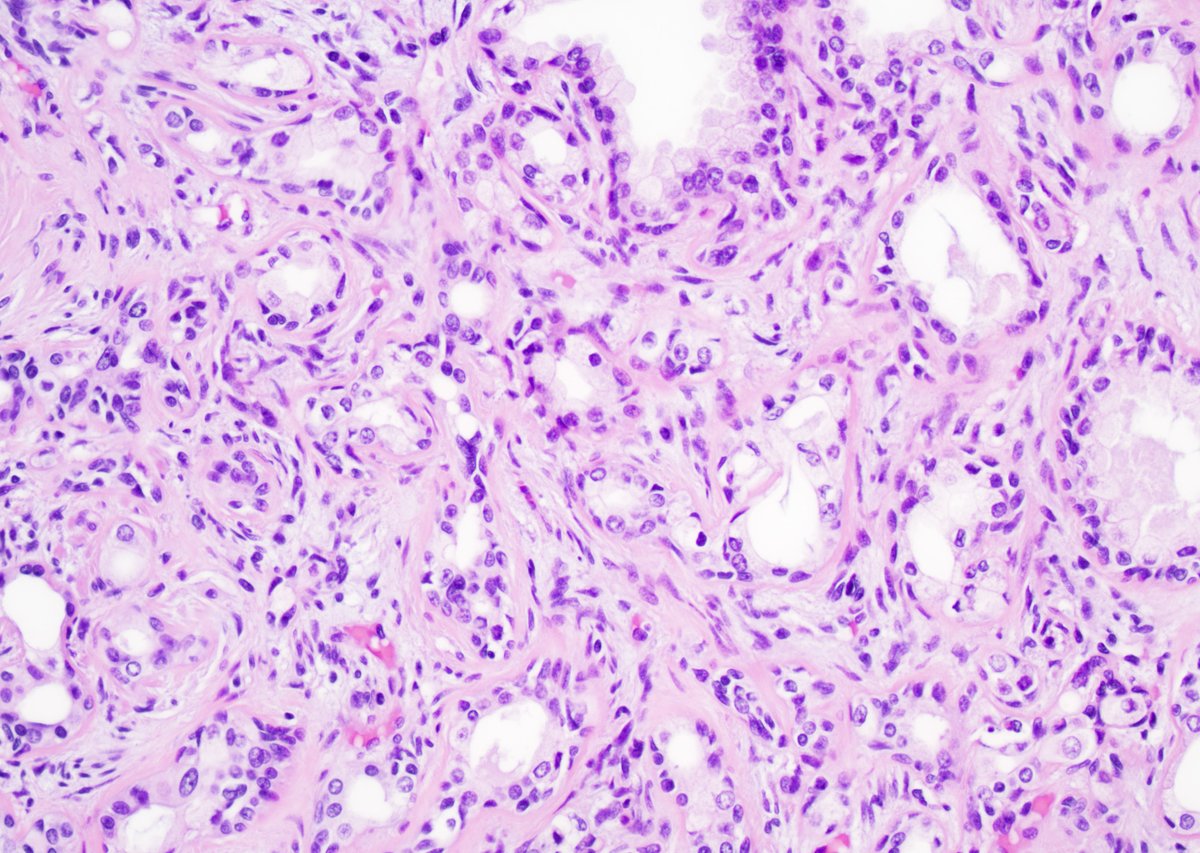
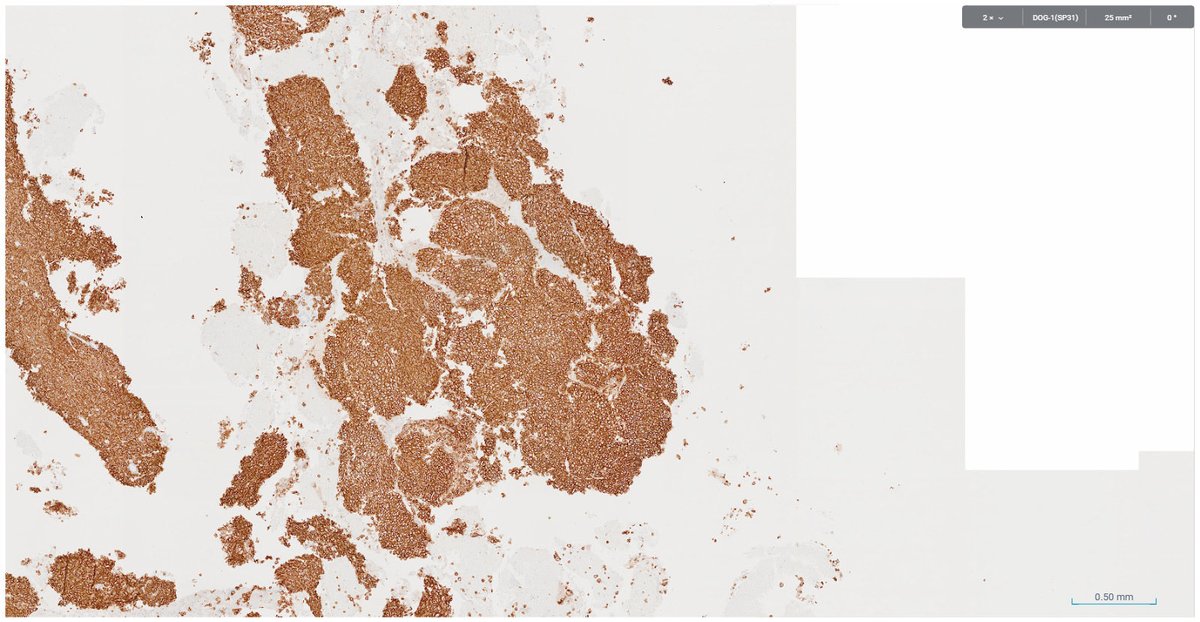
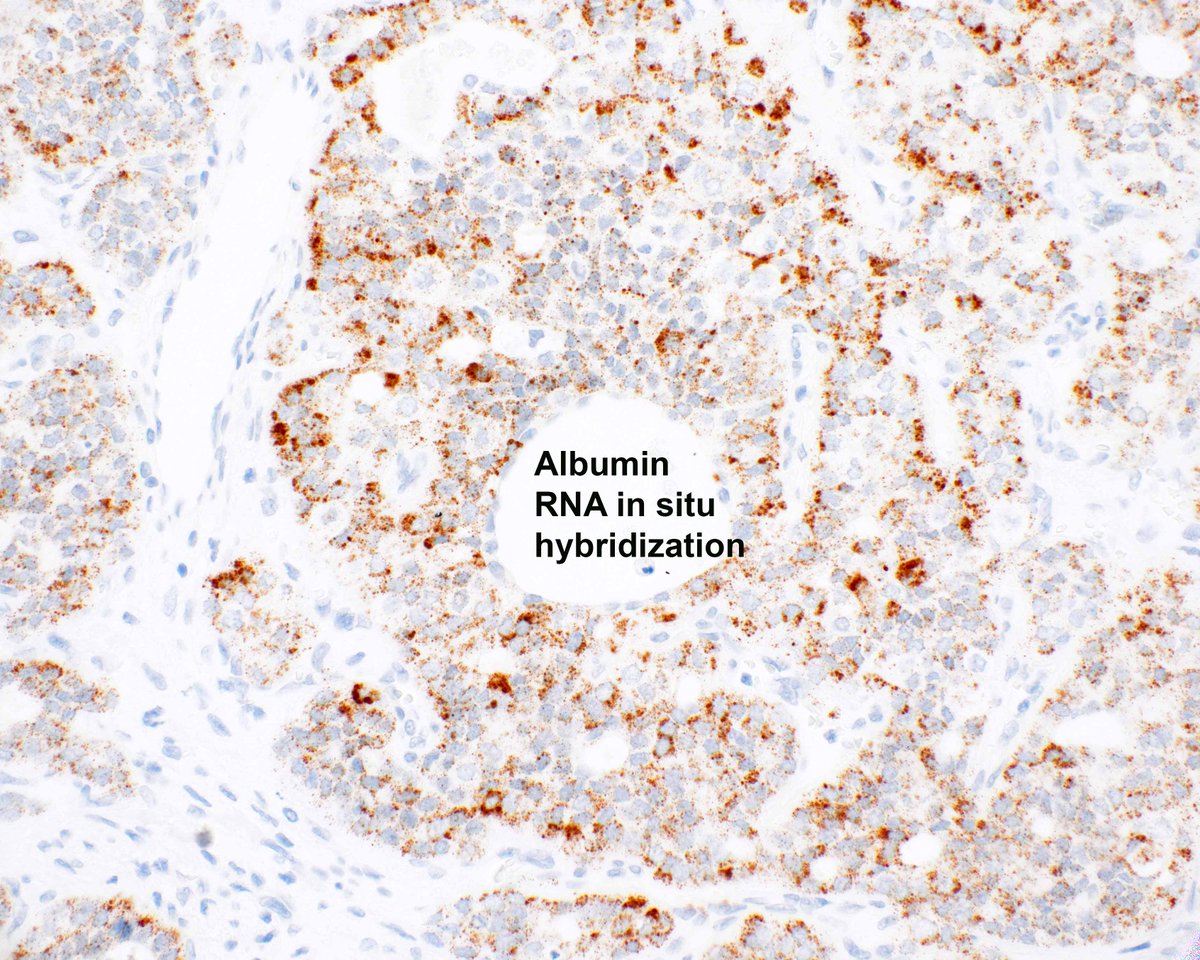
Stunning example of the cholangioblastic variant of intrahepatic cholangiocarcinoma. At first glance these look like neuroendocrine tumors and there is chromogranin/synaptophysin expression (patchy) but not INSM1. The kicker is inhibin. PMID: 33999553; PMCID: PMC8516671.
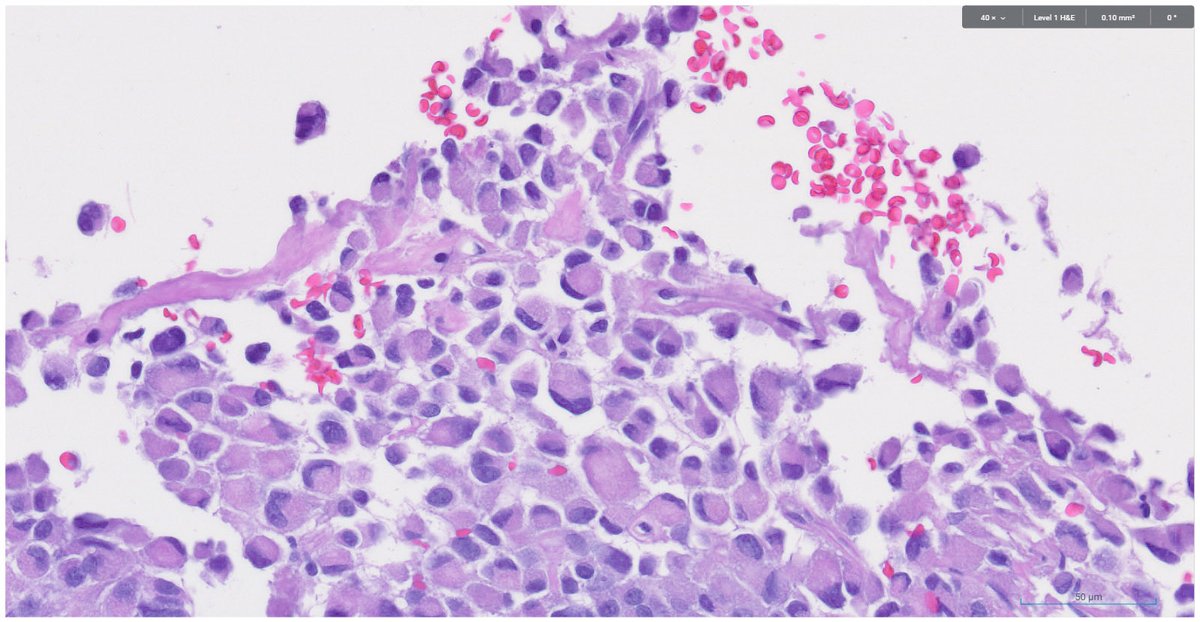
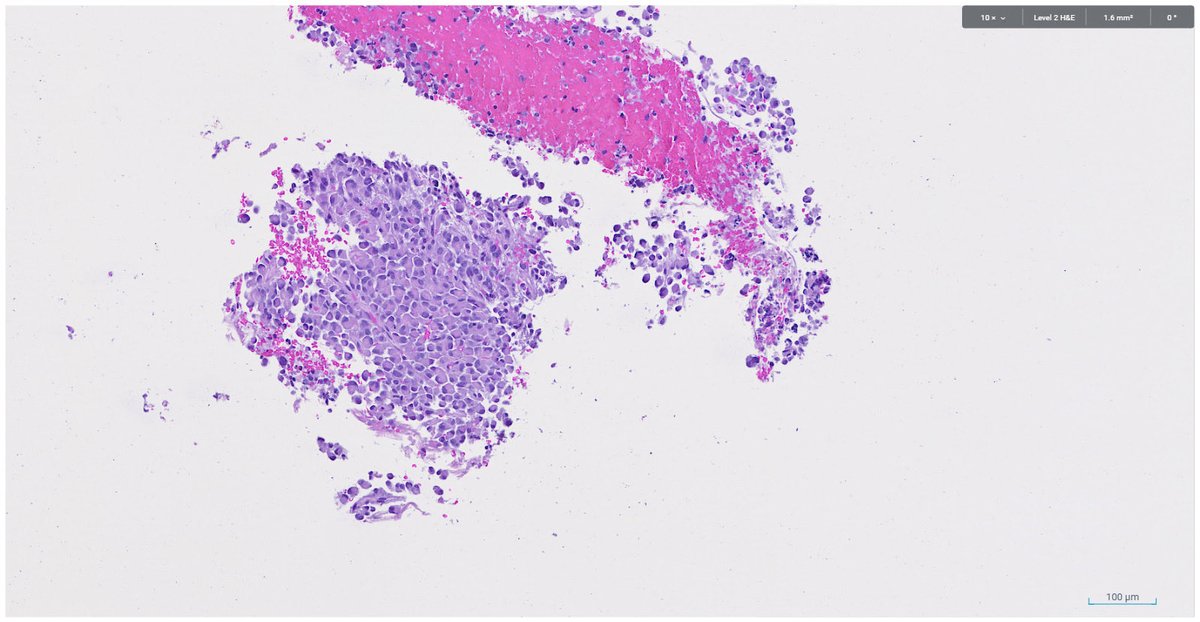
I want to share especially with the #PathTwitter trainees an important lesson that I keep learning. Here's a case to show it.
Bladder biopsy, tumor fully included in one block. What do you think? 🔬
#GUPath
Thank you all for taking part in the case I posted last Friday.
I chose one of the trickier fields to share with you, because of its educational value. The additional images provide more insight into the diagnosis.
Let's go over the answers 1 by 1🧵
#breastpath#PathTwitter