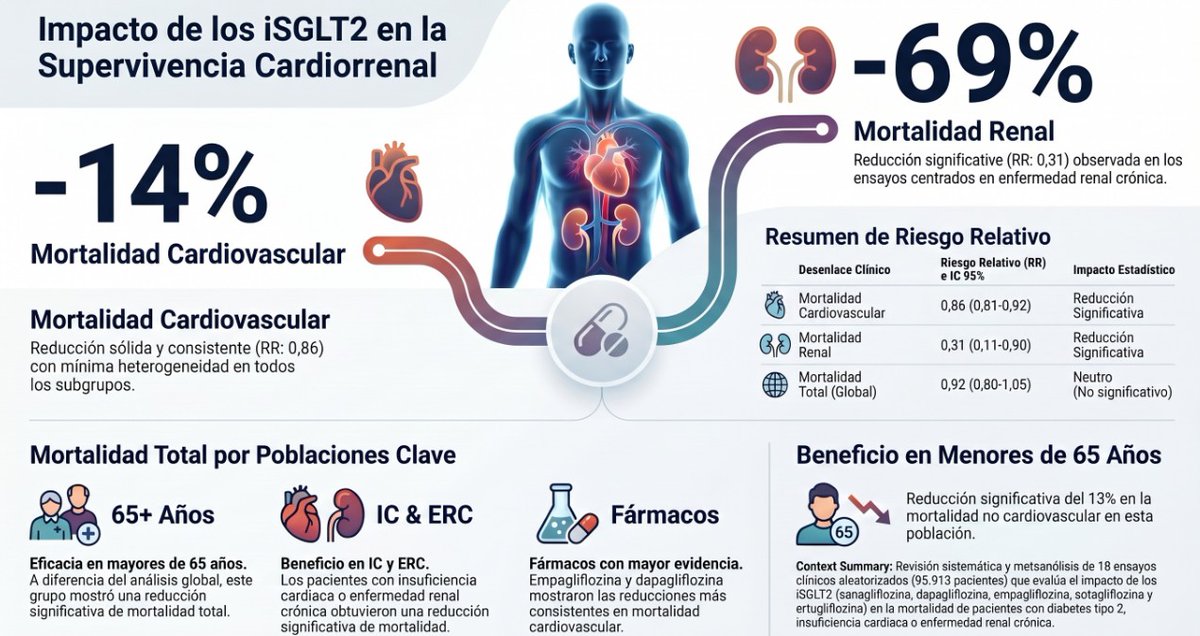
Casi 96.000 pacientes y 18 ensayos aleatorizados después, los datos sobre iSGLT2 y mortalidad son más claros que nunca.
📖 Accede al análisis completo en CardioTeca. https://t.co/leAk3otpHV
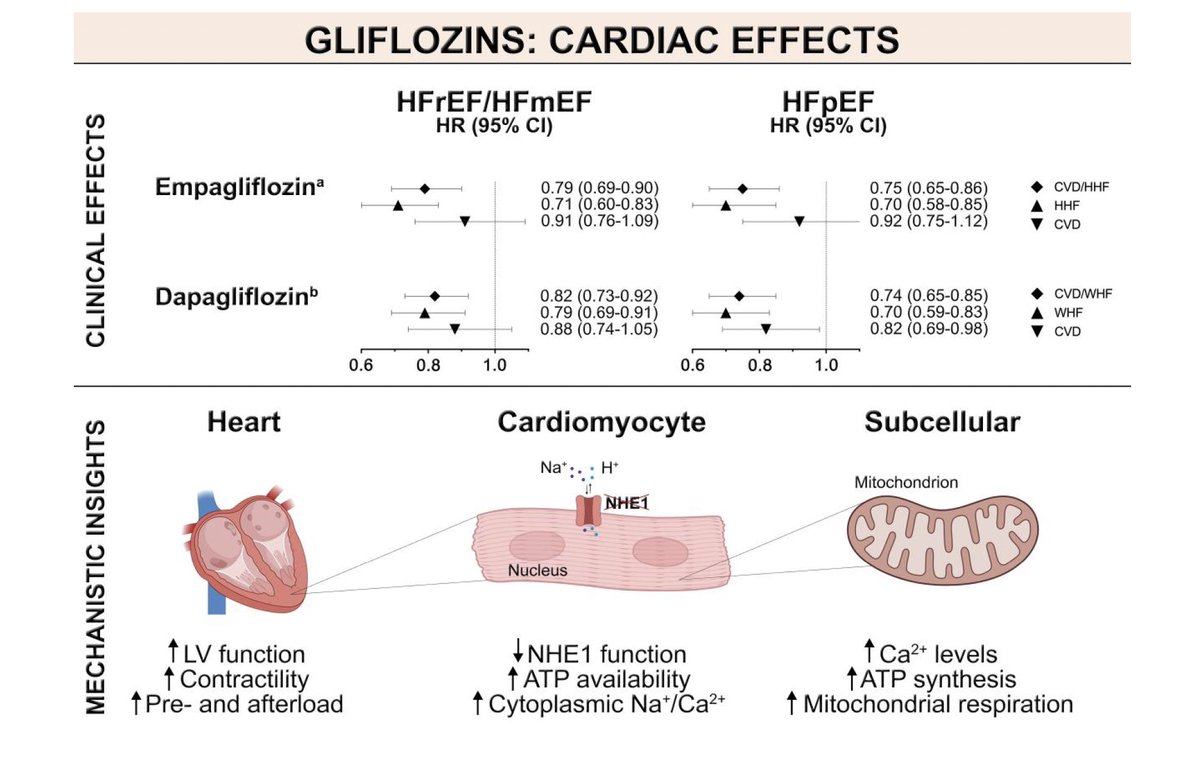
❤️ Reducción del 14% en mortalidad cardiovascular, con efecto consistente en todos los subgrupos de edad.
🫘 Mortalidad renal reducida un 69% en pacientes con enfermedad renal crónica.
👴 Mayores de 65 años: beneficio significativo también en mortalidad total.
💊 Empagliflozina y dapagliflozina, los fármacos con mayor respaldo en supervivencia.
🟩Digoxina en insuficiencia cardiaca de FEVI reducida & ligeramente reducida. 💊🫀
✨️📜DECISION trial.
🟢1,001 👥️ con IC sintomática y FEVI ≤50% bajo tratamiento contemporáneo optimizado🔀 digoxina a dosis bajas 🆚️ placebo, buscando concentraciones séricas de 0.5–0.9 ng/mL (low-dose).
🟢Tras un seguimiento mediano de 36.5 meses, la digoxina NO🚫 redujo significativamente el desenlace primario compuesto de eventos de empeoramiento de IC o muerte cardiovascular (RR 0.81; p=0.133). Tampoco disminuyó mortalidad cardiovascular ni mortalidad total. Sin embargo, sí mostró una tendencia consistente a menos hospitalizaciones por IC y menos eventos de descompensación [🫀💦🏥⤵️24%].
🟢La estrategia de “low-dose digoxin” demostró ser segura: no hubo incremento significativo en efectos adversos graves, bradiarritmias, bloqueos AV, necesidad de marcapasos ni eventos digestivos. 🙂👌🏻
📜🆓️⤵️
https://t.co/Y9ASxuJuVM
https://t.co/97B8RJdHrl
Most of your patients already have CKM syndrome. They just don’t know it yet.
Data from 5,705 ARIC participants:
🟢 Stage 0 (no risk factors): only 0.4%
🟡 Stage 1 (obesity/pre-diabetes): 1.8%
🟠 Stage 2 (HTN, T2D, CKD, MetS): 8.1%
🔴 Stage 3 (subclinical CVD): 56.0%
🔴 Stage 4 (clinical CVD): 32.6%
Nearly 9 in 10 adults have Stage 2 or higher.
Cardiovascular-Kidney-Metabolic syndrome isn’t a future risk — it’s the present reality for most patients walking through your door.
Are we staging them? Are we treating them accordingly?
(ACC/AHA CKM Framework; ARIC Study)
#CKMSyndrome #Cardiology #Obesity #CKD #T2D #CardioTwitter #MedTwitter
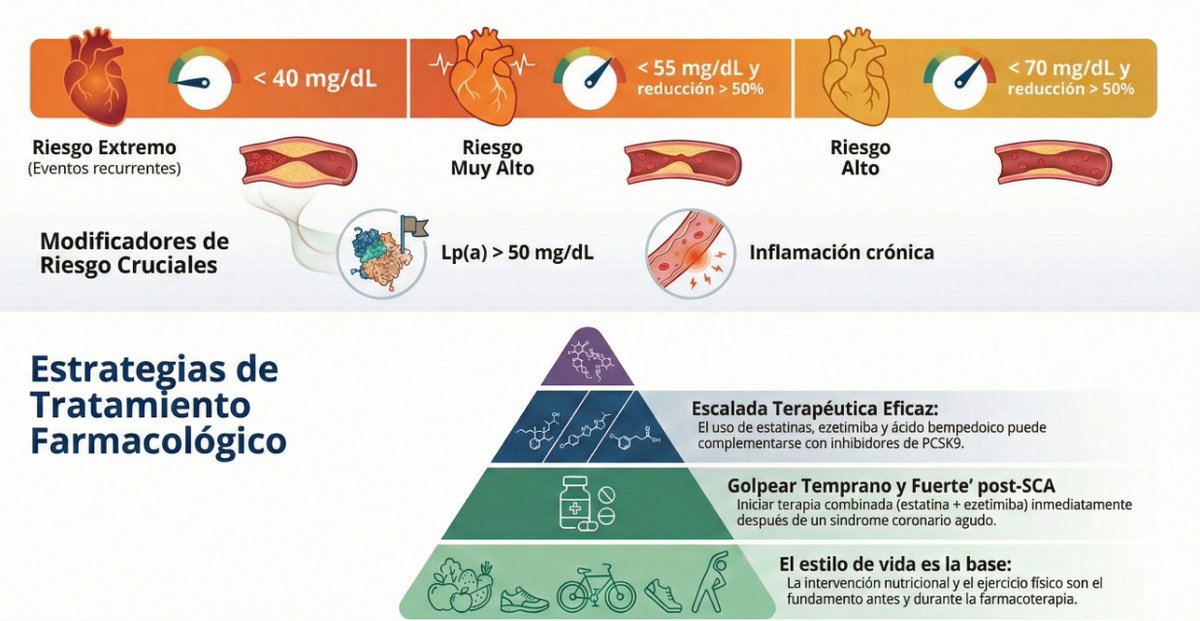
🆕 Guía práctica para el manejo de la dislipidemia: actualización 2025
Lee el artículo completo y revisa las claves prácticas aquí: https://t.co/E1AXoWL66i
🫀 La dislipidemia sigue infradiagnosticada e infratratada: incluso en muy alto riesgo, muchos pacientes no alcanzan objetivos de LDL.
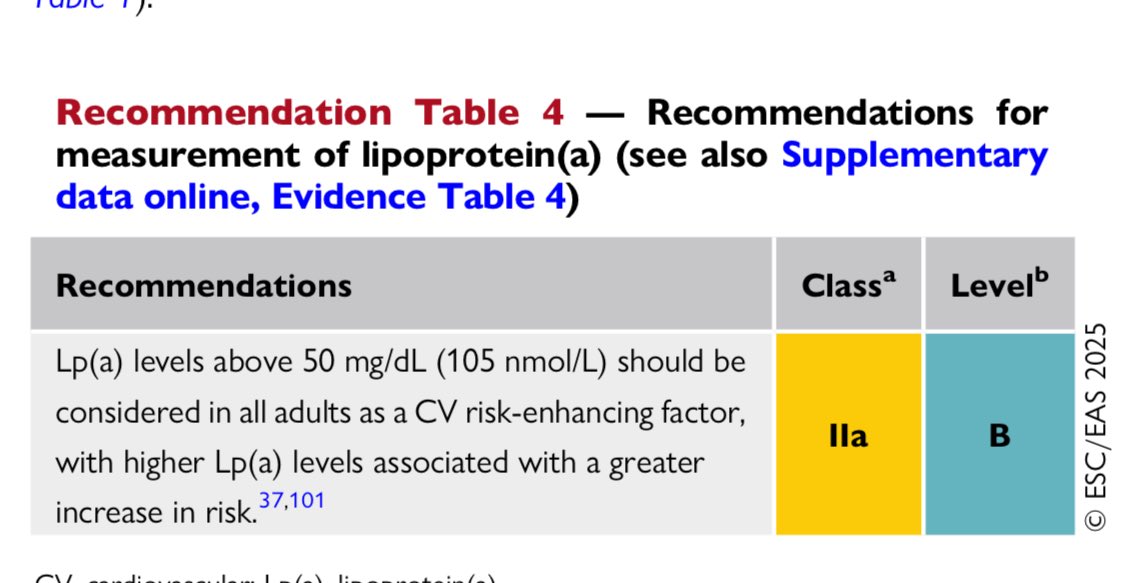
🧪 Más allá del LDL: apoB y colesterol remanente ayudan a explicar el riesgo CV residual; la lipoproteína(a) debe medirse al menos una vez y >50 mg/dL potencia el riesgo.
🎯 Objetivos LDL se mantienen (vs 2019): muy alto riesgo <55 mg/dL (y ↓≥50%); riesgo extremo <40 mg/dL.
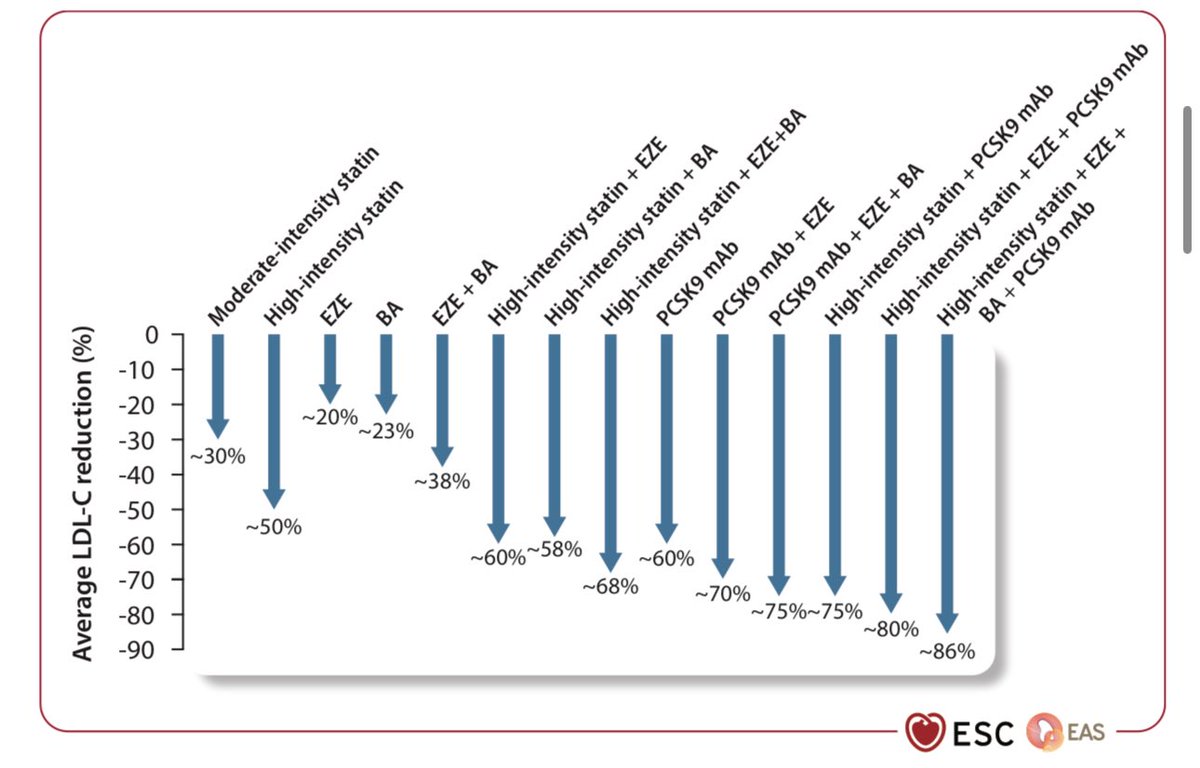
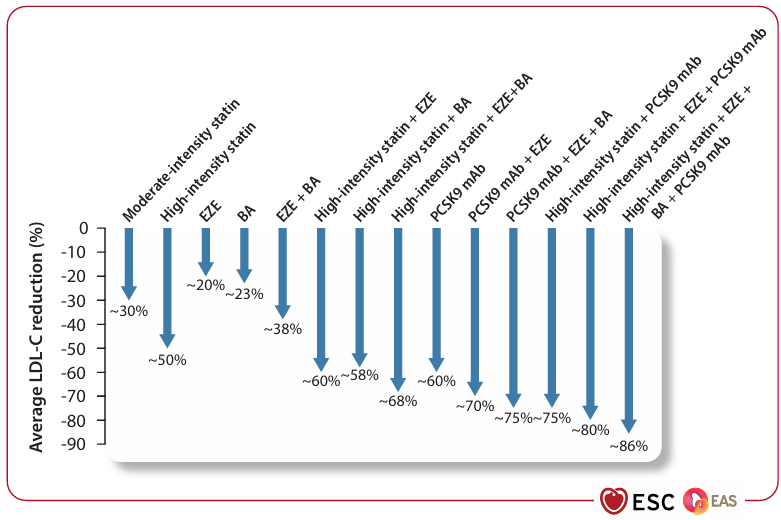
💊 Novedad 2025: terapia combinada precoz y potente tras SCA; si no basta con estatinas, escalar (ezetimibe, ácido bempedoico, PCSK9/inclisirán). 🚀 En camino: fármacos anti-Lp(a) (fase III) y edición génica como apuesta futura.
Una vacuna contra el sarampión cuesta 128 pesos. Vacunar a todos los recién nacidos de México costaría 256 millones de pesos al año.
Y el gobierno de MORENA dejó sin usar 44 mil 457 millones de pesos aprobados para vacunación entre 2022 y 2025.
Eso alcanzaba para vacunar a todas las niñas y niños del país durante más de un siglo.
Hoy enfrentamos un brote epidémico con muertes infantiles.
El dinero estaba. Las vacunas existen. Lo que faltó fue voluntad.
Y mientras este gobierno busca culpar al pasado en vez de admitir sus errores y proteger a la niñez de México,
⚠️ siete de cada diez pesos aprobados para vacunas no se usaron.
La salud pública no admite excusas. Vacunar es salvar vidas.
Los recursos no pueden quedarse en el papel mientras nuestras niñas y niños se enferman.
🚨 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias
#Cardiology#ESC2025#LipidUpdate
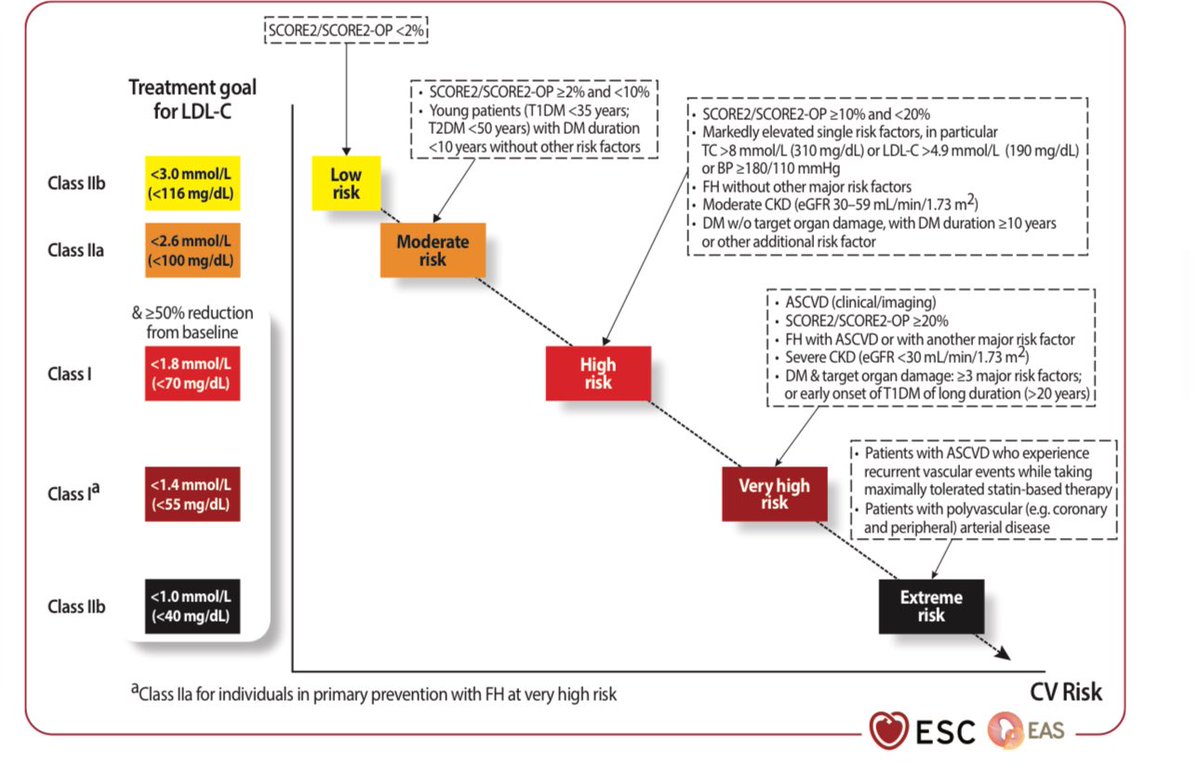
1️⃣ NEW cardiovascular risk estimation:
Use updated #SCORE2 & #SCORE2OP algorithms for 10-year risk in adults aged 40–89, calibrated to local mortality rates.
Risk categories: Very High, High, Moderate, Low.
2️⃣ LDL-C remains the main target ⚡
Lowering #LDLC reduces #ASCVD risk—start pharmacological therapy at thresholds determined by risk and baseline LDL-C.
Goal: “The lower, the better!”
3️⃣ 👨⚕️📉 Innovations in therapy 🧪
•Bempedoic acid now recommended for statin-intolerant/high-risk patients!
•Evinacumab for homozygous familial hypercholesterolemia (FH).
•Inclisiran: ongoing trials, promising ~50% LDL-C reduction.
4️⃣ Acute coronary syndromes (ACS): Early & intensive lipid lowering 🏥
•Initiate high-intensity statin + ezetimibe during ACS hospitalization.
•Combination therapy = Faster & deeper LDL-C reductions, improved outcomes.
5️⃣ Lipoprotein(a): Causal role confirmed
•Measure #Lp(a) at least once in all adults.
•Levels >50 mg/dL (≥105 nmol/L) are risk-enhancing, require aggressive management.
6️⃣ Hypertriglyceridaemia update
•Statins first-line; fibrates not indicated for CV event reduction.
•High-dose icosapent ethyl (4g/day) for high-risk patients with tg 135–499 mg/dL, proven CV event reduction.
•Volanesorsen for familial chylomicronaemia syndrome.
7️⃣ Special populations
•HIV: Statins recommended ≥40 years regardless of LDL-C.
•Oncology: Statins considered in high CV toxicity risk during anthracyclines.
8️⃣ Dietary supplements: 🚫 NOT recommended
•No supplement/vitamin without proven safety & LDL-C efficacy reduces #ASCVD risk.
•Statins and evidence-based therapies continue to lead.
#Guidelines #ESC #Dyslipidaemia #PreventiveMedicine
Hay una epidemia de caídas y muerte asociada en la tercera edad por prescripción de fármacos que afectan la alerta (opioides, benzodizepinas, gabapentinas y antidepresivos).
No hay que recetarlos como si fueran dulces!
https://t.co/8FooDHoUBd
La presidenta dice que las cifras presentadas por el INEGI son un logro de la 4T. Efectivamente, lograron que 25 millones perdieran el acceso a la salud👇
📌Eliminaron el Seguro Popular
📌Eliminaron el INSABI, tras dos años de fracasos
📌Se acabaron el Fondo contra Gastos Catastróficos en Salud
📌Desmantelaron Hospitales Regionales
📌Quitaron financiamiento a los Institutos Nacionales de Salud
📌Redujeron en 113 mil millones el presupuesto para salud al inicio de este sexenio
📌Le quitaron presupuesto a la Secretaría de Salud y eliminarán 11 de sus programas para 2026
🔴🔴2025 AHA/ACC Hypertension Guideline – Key Clinical Insights for Practice
#Hypertension#Cardiology#HeartHealth#BPControl
1️⃣ BP <130/80 mmHg for all adults 🩺
Primary goal for prevention of #CVD, stroke, dementia, CKD, and mortality. Individualize for frailty, pregnancy, or limited lifespan.
2️⃣ Population impact 🌍
Nearly 1 in 2 U.S. adults have hypertension. Awareness, treatment & control remain suboptimal, with disparities by age & ethnicity. #PublicHealth
3️⃣ BP categories 📊
•Normal: <120/<80
•Elevated: 120–129/<80
•Stage 1: 130–139 or 80–89
•Stage 2: ≥140 or ≥90
#BPClassification
4️⃣ Lifestyle first 🍎🏃♂️
DASH diet, weight management, ↓ sodium, ↑ potassium (unless CKD), moderate activity, stress control, limit alcohol. First-line for all. #Prevention
5️⃣ When to start meds 💊
•Always if BP ≥140/90
•If BP ≥130/80 with CVD, stroke, diabetes, CKD, or 10-year CVD risk ≥7.5% (PREVENT calculator).
•If risk <7.5%: start after 3–6 months lifestyle trial if still ≥130/80.
6️⃣ Preferred therapy 💊💊
Stage 2 HTN → 2 first-line drugs in a single-pill combo to improve adherence & speed control.
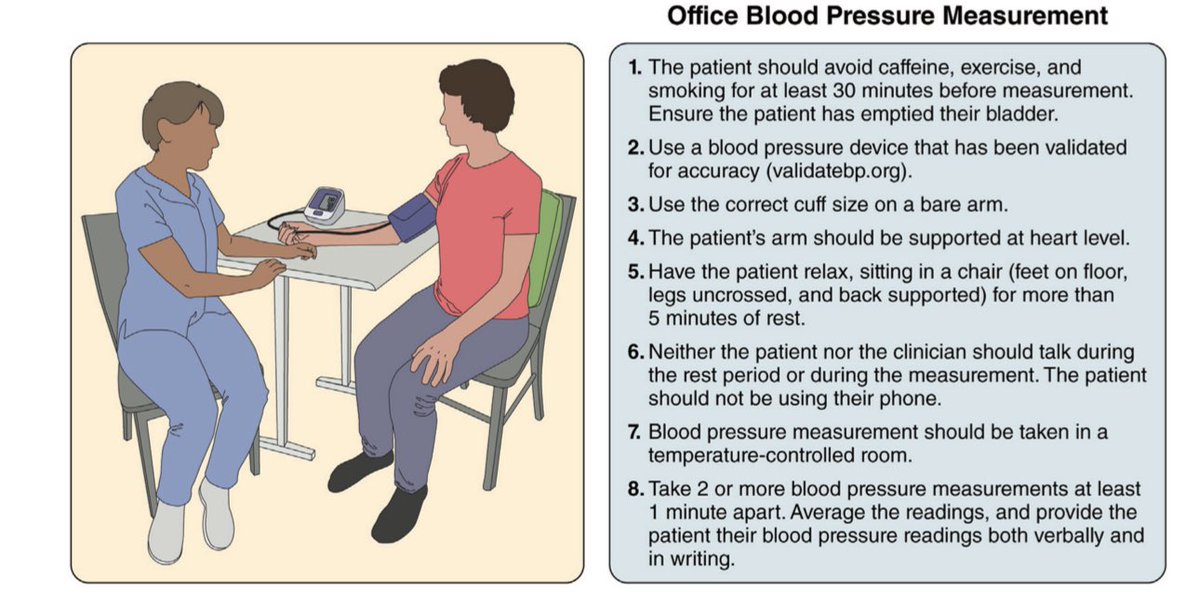
7️⃣ Monitoring 🏠📈
HBPM + team-based care improves control. Avoid relying on cuffless wearables until validated. #DigitalHealth
8️⃣ Pregnancy 🤰
Treat ≥160/110 mmHg urgently. Chronic HTN: target <140/90. Avoid ACEi, ARB, renin inhibitors, atenolol, nitroprusside, MRA. Consider low-dose aspirin to ↓ preeclampsia risk.
9️⃣ Resistant HTN 🛡
Screen for secondary causes (e.g., primary aldosteronism) even without hypokalemia. Multidisciplinary eval before considering renal denervation.
🔟 Severe HTN (>180/120) w/o acute organ damage 🚫🏥
Manage outpatient—no rapid IV/PO BP lowering unless organ injury present.
💡 Bottom line:
Early detection, risk-based thresholds, lifestyle integration, combination therapy, and team-based follow-up are the cornerstones of modern hypertension control.
📎 Full guideline: https://t.co/UIoACytOgv
#Hypertension2025 #ACC #AHA #Guidelines #CardioTwitter
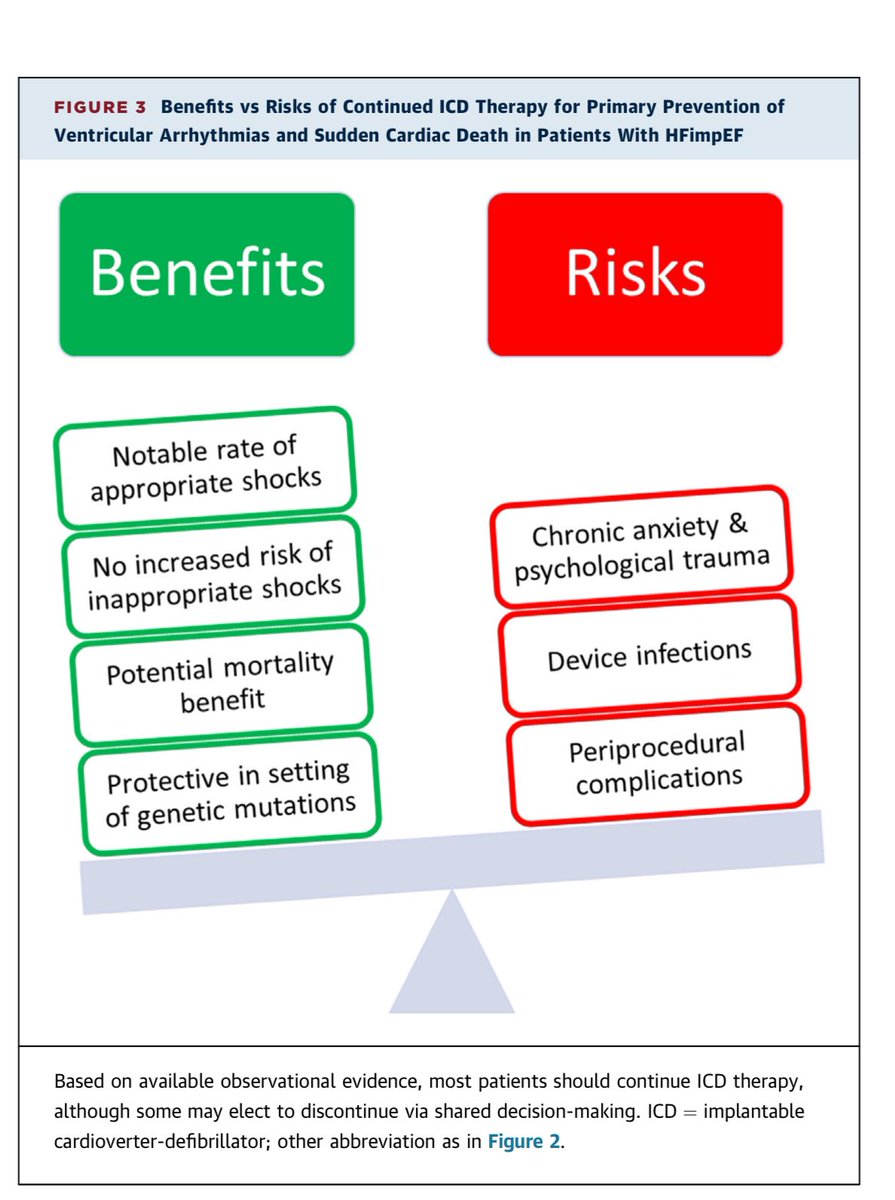
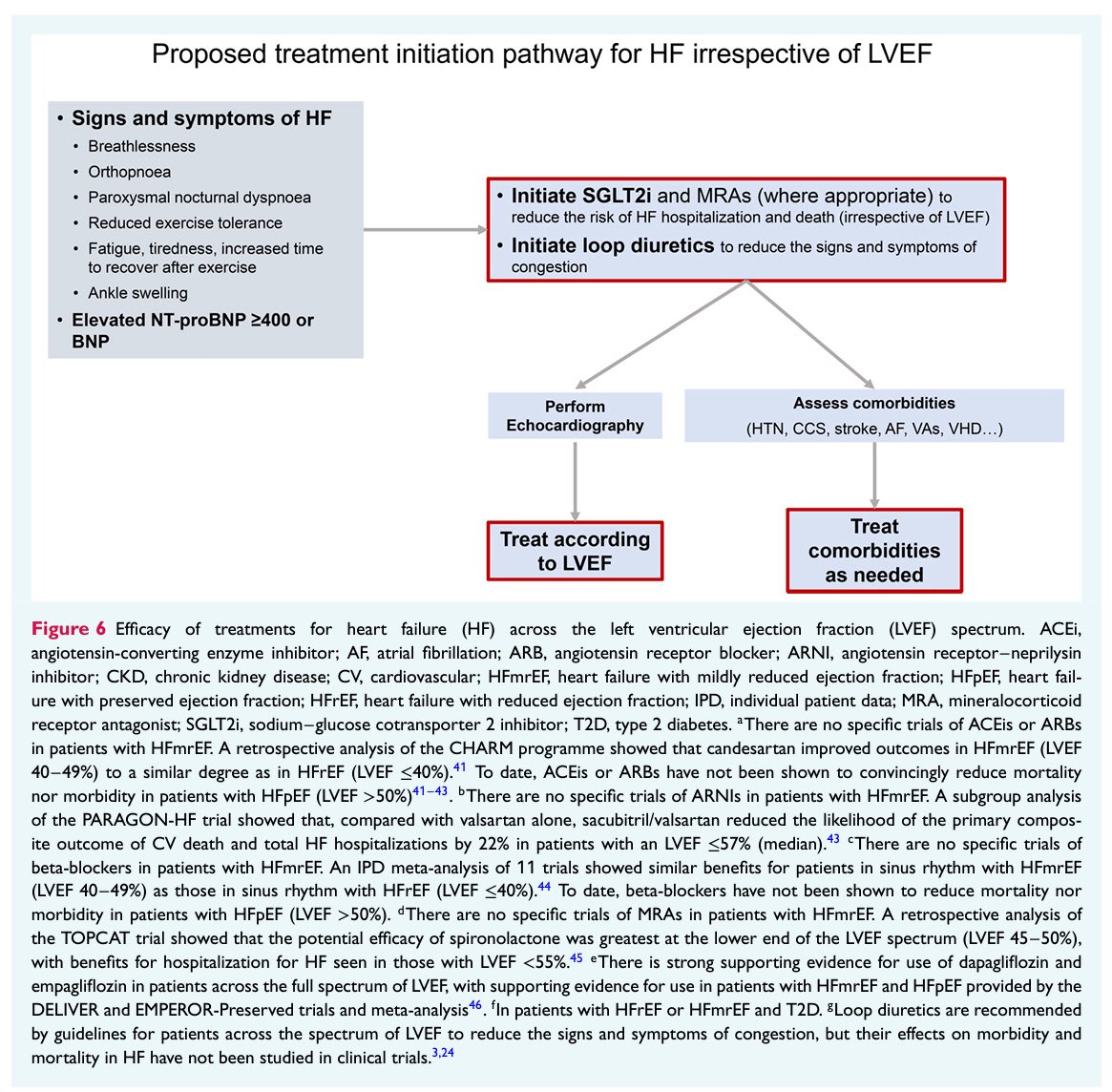
🔴 Management of Heart Failure With
Improved Ejection Fraction @JACCJournals
📪 https://t.co/8uNIdDHYeF
What to do when your HFrEF patient “recovers”?
LVEF improves, symptoms resolve, but the heart failure story isn’t over.
Let’s unpack #HFimpEF — the new frontier in #HeartFailure care.
#CardioTwitter #MedTwitter🧵
2/ First things first: what is HFimpEF?
▶️ Baseline LVEF ≤40%
▶️ Follow-up LVEF >40%
▶️ ≥10-point improvement
This is not “cure” — it’s a state of remission.
#EjectionFraction #HeartFailure
3/Why it matters:
Up to 20–25% of patients with HFrEF now meet criteria for HFimpEF thanks to modern GDMT.
But here’s the catch…
Relapse is real — especially if meds are stopped.
#CardioCare #EvidenceBasedMedicine
4/What does the evidence say?
🧪 Trials like TRED-HF show a high rate of relapse after withdrawing HF meds — even in asymptomatic patients with recovered EF.
Bottom line: Don’t stop GDMT.
#HeartFailureManagement
5/The 4 Pillars of GDMT still apply:
✅ ARNi/ACEi/ARB
✅ Beta-blockers
✅ MRA
✅ SGLT2i
Even if EF looks good, these drugs prevent reverse remodeling.
#SGLT2 #Cardiology #HFpEF
6/ Phenotyping is key
Not all HFimpEF is the same:
🧬 Ischemic vs. non-ischemic
🧬 Inflammatory (e.g. myocarditis)
🧬 Genetic (e.g. TTN truncations)
Tailor follow-up + treatment accordingly.
#PrecisionMedicine
7/ What’s new in follow-up?
🔁 Serial imaging (echo, strain)
🩸 Biomarkers (NT-proBNP, troponins)
⚠️ Watch for recurrence: weight, edema, fatigue.
#CardioMonitoring #Telemedicine
8/ How to counsel patients?
“Your EF has improved, but your heart is still vulnerable.”
➡️ Reframe as remission, not cure
➡️ Lifelong follow-up
➡️ Stay on meds
#PatientEducation #HeartHealth
9/ HFimpEF is not the end of the story — it’s a new chapter.
Treat it with the same vigilance as HFrEF.
Let’s not be fooled by numbers alone.
#HeartFailureAwareness
🚨 Hypertension remains the #1 cause of death worldwide! 🌍💔 But new drugs are changing the game.
🔬 Aprocitentan, a dual endothelin receptor antagonist, is the first new #hypertension drug class approved in almost 2 decades! 💊🚀
📉 New therapies like siRNAs, aldosterone synthase inhibitors & non-steroidal MRAs could transform #BloodPressure management.
💡 Personalized medicine & better adherence strategies will be key! 🔑
🔗 Read more: https://t.co/FbiZUbcvUE
#Cardiology #HeartHealth #MedicalInnovation #HypertensionAwareness #BloodPressureMatters ❤️🩺
1.28 billion people worldwide are living with hypertension - an alarming global health challenge.
This silent condition often goes unnoticed but significantly increases the risk of heart disease and stroke.
Don't wait for symptoms, take action today!
#Hypertensionawareness
Como médico q atiende a pacientes con enfermedad vascular coronaria, periférica y cerebral; me preocupa q un fármaco que disminuye:
- mortalidad CV+ictus+IAM
- mortalidad total
- reingresos por IC
- enfermedad renal
en estos pacientes q además tienen adipopatía,(1)
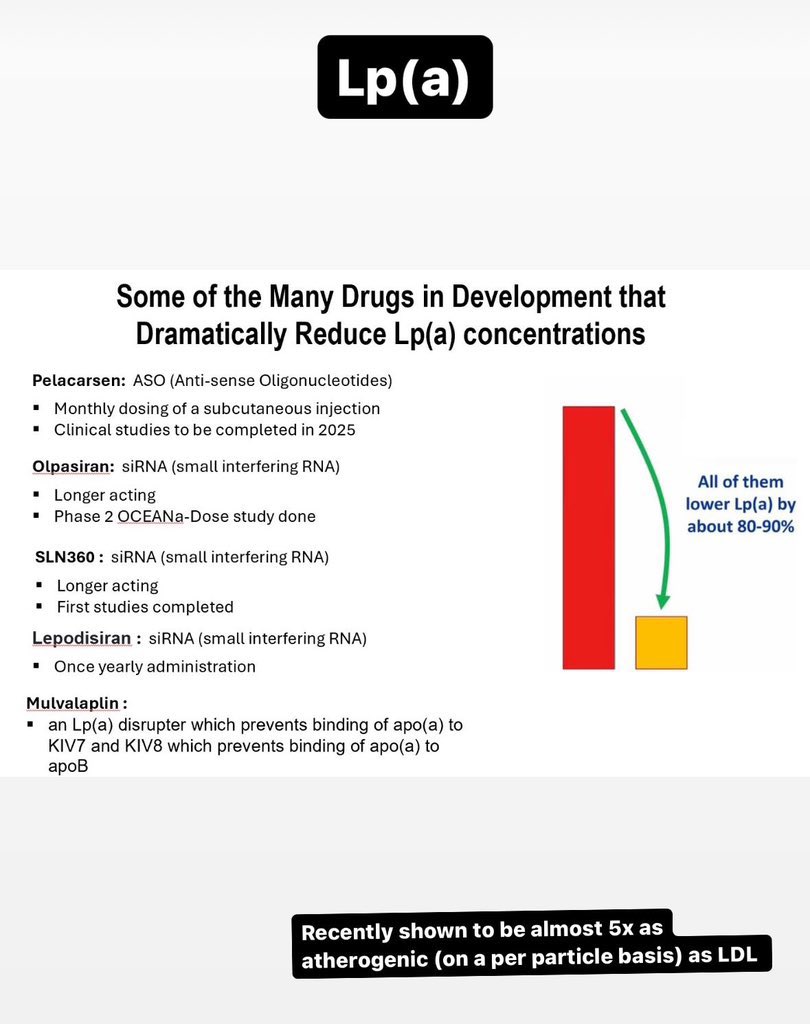
Lp(a) – recently shown to be almost 5x as atherogenic (on a per particle basis) as LDL
Some on the many Lp(a) targeted therapies in development, and their evidence 👇 via @Drlipid


![javier20ch's tweet photo. 🟩Digoxina en insuficiencia cardiaca de FEVI reducida & ligeramente reducida. 💊🫀
✨️📜DECISION trial.
🟢1,001 👥️ con IC sintomática y FEVI ≤50% bajo tratamiento contemporáneo optimizado🔀 digoxina a dosis bajas 🆚️ placebo, buscando concentraciones séricas de 0.5–0.9 ng/mL (low-dose).
🟢Tras un seguimiento mediano de 36.5 meses, la digoxina NO🚫 redujo significativamente el desenlace primario compuesto de eventos de empeoramiento de IC o muerte cardiovascular (RR 0.81; p=0.133). Tampoco disminuyó mortalidad cardiovascular ni mortalidad total. Sin embargo, sí mostró una tendencia consistente a menos hospitalizaciones por IC y menos eventos de descompensación [🫀💦🏥⤵️24%].
🟢La estrategia de “low-dose digoxin” demostró ser segura: no hubo incremento significativo en efectos adversos graves, bradiarritmias, bloqueos AV, necesidad de marcapasos ni eventos digestivos. 🙂👌🏻
📜🆓️⤵️
https://t.co/Y9ASxuJuVM
https://t.co/97B8RJdHrl](https://pbs.twimg.com/media/HIDD1e2XsAADIRs.jpg)


















![javier20ch's tweet photo. 🟩Digoxina en insuficiencia cardiaca de FEVI reducida & ligeramente reducida. 💊🫀
✨️📜DECISION trial.
🟢1,001 👥️ con IC sintomática y FEVI ≤50% bajo tratamiento contemporáneo optimizado🔀 digoxina a dosis bajas 🆚️ placebo, buscando concentraciones séricas de 0.5–0.9 ng/mL (low-dose).
🟢Tras un seguimiento mediano de 36.5 meses, la digoxina NO🚫 redujo significativamente el desenlace primario compuesto de eventos de empeoramiento de IC o muerte cardiovascular (RR 0.81; p=0.133). Tampoco disminuyó mortalidad cardiovascular ni mortalidad total. Sin embargo, sí mostró una tendencia consistente a menos hospitalizaciones por IC y menos eventos de descompensación [🫀💦🏥⤵️24%].
🟢La estrategia de “low-dose digoxin” demostró ser segura: no hubo incremento significativo en efectos adversos graves, bradiarritmias, bloqueos AV, necesidad de marcapasos ni eventos digestivos. 🙂👌🏻
📜🆓️⤵️
https://t.co/Y9ASxuJuVM
https://t.co/97B8RJdHrl](https://pbs.twimg.com/media/HIDD1fDXUAAaXot.jpg)