1/ Impressive #challenge clinical trial update at #asco26 making a financial case (from Canadian perspective)
Bottom line - SEP can improve DFS for St iii CRC and despite an upfront cost, would save health systems money overall
4/
Practice changing study and I look forward to studies incorporating oral therapy in this deadly in earlier settings and combinations that may overcome patterns of resistance.
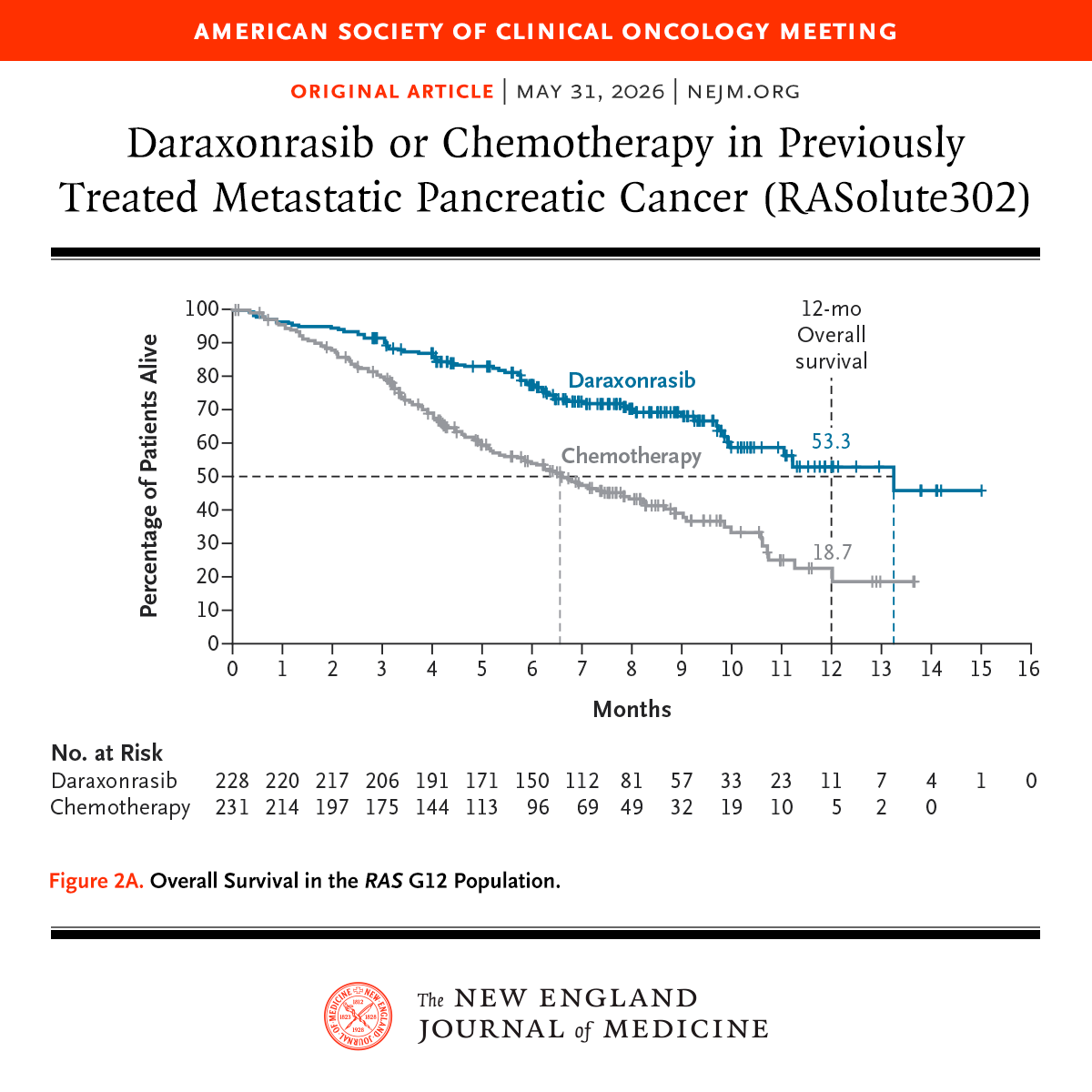
1/ A novel KRAS(on) inhibitor improves survival in previously treated patients with metastatic pancreatic cancer with a RAS G12 mutation
mOS 13.2v6.6 months (HR 0.4)
Toxicities: rash (85%, Gr3 13%)
Limitations: Ctrl arm drop out (>10%), small population of non G12
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
3/
Very small non G12 mutation population, and further data will be necessary to use in other settings
Highly selected population -not all patients have opportunity for second line therapy in PDAC
Lastly drop out in control arm is high (>10%) as unblinded
@NiuSanford For a device with a novel MoA being added to CT, at least one sham Ctrl trial is needed. Did those in ctrl arm drop out early and pursue BSC or seek another trial? How well was survival data collected in pt who dropped out? OS censoring seems unequal at 1yr...
Onc consultations are complex. AI LLMs may help providing patient friendly summaries. Grateful for @JCOOP_ASCO publishing my letter on the topic. Verification studies are required.
https://t.co/agHrG2aFc0