@CaroPiek Meine Vision: Viele Menschen, d. sich ein kooperatives Miteinander + Schutz v. Kapitaldominanz wünschen, schließen sich mit ihren Ressourcen zusammen, erobern Lebensräume + sind i.d. Lage, diese integrativ, sozial gerecht + hoffnunggebend zu gestalten.
Ziel: Vorbereitung auf 1/x
@HarrySpoelstra deep vein thrombosis + severe post-COVID fatigue.
In Germany, health insurance providers do not officially cover specific examinations capable of revealing lasting physical damage to the cardiovascular or immune systems. 2/2
@HarrySpoelstra What examinations and lab tests would be important to determine what lasting damage my cardiovascular system has sustained after three SARS-CoV-2 infections?
After the second infection: deep vein thrombosis, pulmonary embolism + post-COVID fatigue. After the third infection: 1/x
The long-term cardiovascular risks of SARSCoV2 infection and reinfections
Your heart is under silent, cumulative attack from SARSCoV2, and every reinfection can reload/worsen the damage.
Here a personal recap of 10 important studies from the last 2 years showing exactly how this virus and its reinfections can/may shape (and shorten) your cardiovascular future.
Evidence is clear, long-term, and growing.
Print and show your Cardiologist.
Let’s connect the dots…
1. Immunothrombosis multi-omics study:
3 months after hospitalisation, long COVID patients still have blood biologically “clot-ready” with persistent endothelial activation and prothrombotic signalling.
https://t.co/9yj7zVbgxO
2. IL-6 & SAA 6-year study:
Higher acute-phase IL-6 and SAA levels independently predict cardiovascular events and death up to 6 years later, the initial inflammatory storm leaves a lasting CV mark.
https://t.co/Vk7FvK9fQc
3. MIS-C long-term outcomes:
Up to 4.5 years later, MIS-C raises cardiovascular disease risk 14× and hypertension 9× in children, with risks still accumulating.
https://t.co/itRENsOlOS
4. Viruses & cardiac disease review:
SARS-CoV-2 stands out for direct cardiomyocyte invasion + explosive damage + relentless accumulation of risk with every reinfection.
https://t.co/fOX07JNW2o
5. Mayo PET long COVID study:
Persistent cerebral hypometabolism in fatigue/PEM patients still detectable up to 2 years post-infection.
https://t.co/puvllNfghC
6. Reinfection CV outcomes summary:
Reinfections worsen cumulative heart damage, arrhythmias, thrombosis, stroke risk and long COVID cardiovascular symptoms.
https://t.co/B3q7DzyxCZ
7. Youth reinfection & long COVID study:
Reinfection roughly doubles PASC risk, with myocarditis up to 3.6× higher, heart disease ~2× higher and increased thromboembolism.
https://t.co/aqN3VV0kMX
8. Mild infection + reinfection risk:
Even mild cases trigger lasting endothelial damage and prothrombotic state (1.5–2× long-term CV risk), each reinfection compounds the burden.
https://t.co/SvPzOBSOx1
9 Mitochondrial dysfunction in long COVID:
Persistent mitochondrial dysfunction and suppressed oxidative phosphorylation remain in long COVID, pointing to durable multi-organ impact.
https://t.co/98MbV19R9r
10. Cumulative reinfection impact on future CV health:
Reinfection stacks additional damage on prior endothelial injury and inflammation, increasing lifetime risk of heart failure, arrhythmias, thrombosis and accelerated cardiovascular disease.
https://t.co/aqN3VV0kMX
11. Extra, my earlier general reminder post on this exact theme: https://t.co/o3QT12nIG4
‼️Overall convergence across the studies:
Immunothrombosis, acute inflammation markers, direct invasion, endothelial damage, and mitochondrial issues create lasting CV vulnerability that reinfections can keep reloading. #L0ngC0vid
The pattern is very clear.
Fewer infections = lower lifetime cardiovascular risk.
You only have one heart.
Protect it!
#AvoidSars2 #AvoidReinfections #CleanAir #VaccineUpdated
Spoiler: Kommt nie!
Realistischer ist, dass Menschen, die im System nix mehr zu verlieren + gewinnen haben Amok laufen. Im Stillen dahinsiechen sieht nicht jeder einen Lebenssinn.
Wann kommt eigentlich die Reform der Abgeordnetenvergütung?
-Diätensenkung
-Senkung der steuerfreien Vergünstigungen
-Streichung der Fraktionsreisen unter dem Radar
-Aus für Doppeldiäten
-Rücknahme der Erhöhung der Parteienfinanzierung
-Einzahlung aller Abgeordneten in das PV,RV
Wann kommt eigentlich die Reform der Abgeordnetenvergütung?
-Diätensenkung
-Senkung der steuerfreien Vergünstigungen
-Streichung der Fraktionsreisen unter dem Radar
-Aus für Doppeldiäten
-Rücknahme der Erhöhung der Parteienfinanzierung
-Einzahlung aller Abgeordneten in das PV,RV
i don’t think it’s selfish or unnatural to want to be important to someone. even if it’s just one person. it really does make life seem more worth enduring. if nothing is keeping you tethered here, you’ll just drift away. like a sad little balloon.
Many chronically ill patients no longer fear only their disease. They fear the healthcare system itself after years of dismissal, disbelief, humiliation, and abandonment.
Comprehensive Immunophenotyping of Monocytes and Dendritic Cells Suggests Distinct Pathophysiology in Chronic Fatigue Syndrome and Long COVID
🚨Interesting new decisive data confirming divergence:
ME/CFS and Long COVID are NOT the same disease!
➡️This international study used multiparameter flow cytometry on peripheral blood mononuclear cells to compare immune profiles in ME/CFS (n=103), Long COVID (n=63), and healthy controls (n=41). It targeted monocytes (M1/M2-like), dendritic cells (DCs), and T-cell subsets to uncover disease-specific signatures,
➡️Long COVID Profile:
- Marked by increased M2-like monocyte polarization, elevated CD80 (costimulatory marker) across monocyte subsets, DC expansion, and paradoxically reduced activation markers (e.g., CD69+CD38),
- Indicates persistent immune activation combined with exhaustion features,
➡️ME/CFS Profile:
- Characterized by reduced costimulatory molecule expression (e.g., lower CD80 on DCs/monocytes), impaired CCR7 expression (disrupting immune cell trafficking), and less coordinated activation patterns, consistent with immune suppression,
➡️Additional Analyses:
- Correlation networks showed more extensive, integrated immune interactions in Long COVID vs. fragmented patterns in ME/CFS,
- Principal component analysis (PCA) and PLS-DA revealed distinct immunophenotypic clusters, enabling moderate discrimination between the two conditions (AUC ~0.76 in moderate cases),
➡️Implications:
- Age-adjusted statistics confirmed differences,
- Findings point to divergent post-infectious immunopathologies rather than a shared syndrome,
➡️Conclusion:
- ME/CFS and Long COVID are not the same disease,
- They drive opposite immune failures, one of chronic hyper-activation tipping into exhaustion, the other of outright suppression and trafficking collapse,
- Treating them as interchangeable is scientifically indefensible and clinically harmful,
- Distinct biomarkers now exist:
→Separate pathophysiology demands separate diagnostics and therapies!
#MECFS #LongCOVID #AvoidSars2 #AvoidReinfections
https://t.co/pMKdJKcxoA
If capitalism is so great, why do corporations need so many tax breaks, subsidies, exemptions, grants, legal protections, bailouts, and trade protections?
When citizens need these things, why is it socialism?
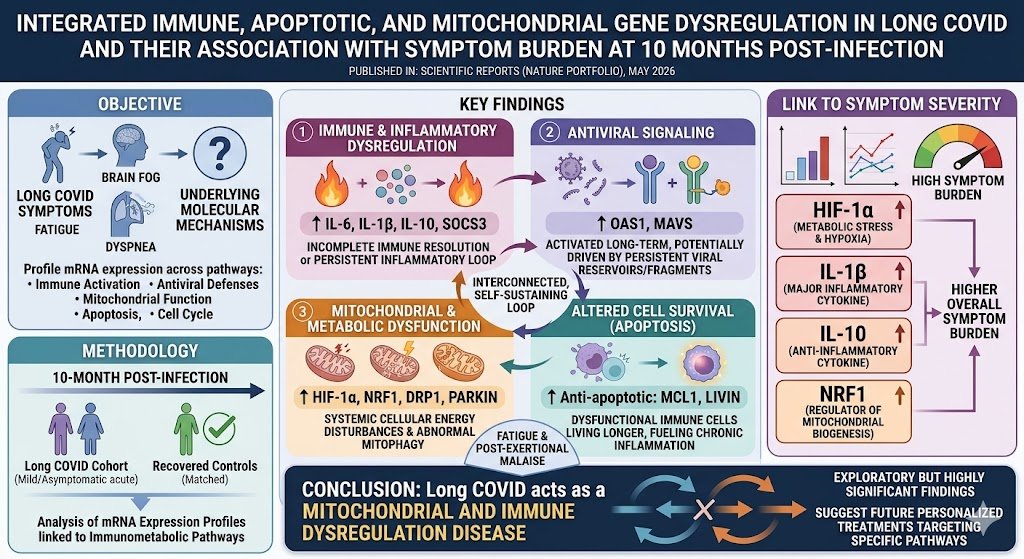
Long COVID shows persistent immune, antiviral, and mitochondrial gene dysregulation 10 months post‑infection, linking IL‑1β, IL‑10, HIF‑1α, and NRF1 to symptom severity. It behaves as a chronic immunometabolic disorder.🧵
A lot of people think Long COVID is a bunch of different diseases. I used to think this myself, but I realize the evidence for this view is actually not that strong.
Typically, people point to the 200+ symptoms and go "OMG, this is so heterogeneous, everyone has something different going on." But apply this logic to basically any other disease. Many of them would have just as many symptoms associated with them, if not more.
The more sophisticated take is to point to the research showing different mechanisms: viral persistence in some, microclots in others, autoimmunity in others, mitochondrial dysfunction in others, autonomic dysregulation in others. There is actual data that shows this. Nevertheless, it is still a leap to go from "we see different mechanisms" to "therefore these are different diseases."
About a year ago, Iwasaki said "We now understand that long COVID is likely not a single disease, but rather an umbrella term that encompasses multiple distinct endotypes that's triggered by acute SARS-CoV-2 infection."
I don't buy it anymore.
Pre-1984 AIDS looked exactly like Long COVID looks now, a bewildering multi-system syndrome. I can't find any researchers who attempted to catalog all the different symptoms associated with HIV, but if someone did, it would blow past 200 easily.
You can see this in the name: "acquired immunodeficiency syndrome". It wasn't until they figured out the CD4 depletion thing that they converted a weird grab bag of pneumonias, cancers, wasting, brain issues, etc. into a single illness.
Syphilis is another example. It can cause neurological disease, cardiovascular issues, psychiatric issues, skin issues, eye issues, and bone problems. For hundreds of years people thought these were different illnesses, until they found the bacteria. With syphilis, you have one organism doing many different things to many different tissues in many different people.
Then, there's acute COVID itself. It has at least 5 distinct mechanisms. Some people have respitory failure. Others have heart attacks. Some get MIS-C. Nobody says COVID is different diseases. Why was it acceptable for acute COVID to involve multiple mechanisms but suddenly after the acute infection, it must be split into "endotypes"? Nothing has changed besides the length of time.
Subtypes are not the same as "different diseases." And I'm skeptical that Long COVID even has subtypes. People claim it's necessary to find treatments, but so far, no one has found a treatment for any "subtype" of Long COVID.
I think the subtype framing is mostly used to enable the move of peeling off different groups and folding them into pre-existing buckets (ME/CFS, MCAS, POTS, dysautonomia) largely for social and political reasons.
In Planung: Absenkung des Rentenniveaus, Abstriche bei der Gesundheitsversorgung und der Pflege, Kürzungen beim Wohngeld und beim Elterngeld. All das, um letztlich die Pfründe derer zu sichern, die diesen Sozialstaat ohnehin nicht brauchen. Das ist Klassenkampf von oben.
@Boenau Bah... Yeah, but it's cheap shit for working slaves. You can't drive through. You have to drive backwards to come out. This is a physical and mental burden.
On the airport in Frankfurt/germany there is an hotel where you can take your car with an escelator in your appartment.
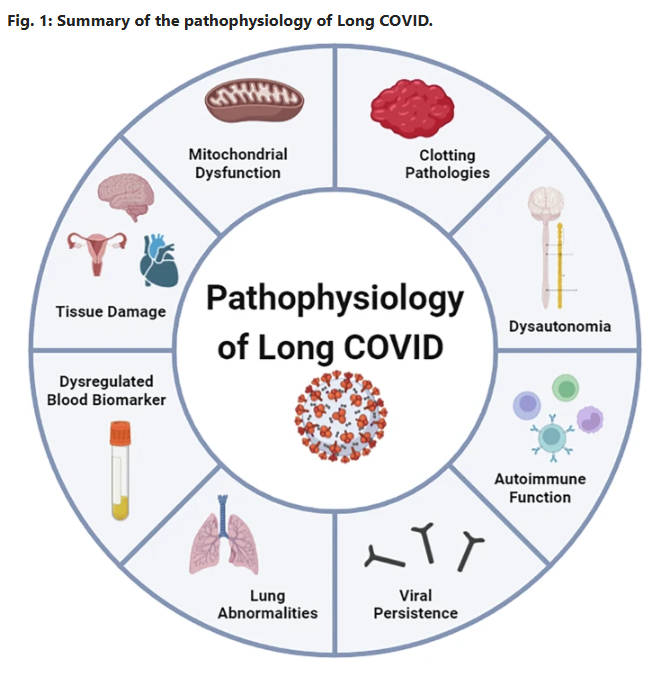
Current status and future perspectives on the mechanistic and pathophysiological understanding of long COVID
🚨JUST DROPPED YESTERDAY and rips open the black box of Long COVID:
Viral persistence up to at least 24 months. Fibrin microclots that laugh at fibrinolysis. Autoimmune storm. Mitochondrial sabotage. An up-to-date full mechanistic map is finally here!
No more guessing. This changes everything, let’s dig into this overview👇, better yet…..read it yourself!! #MustRead
➡️Global Impact & Context:
- Long COVID (PASC) affects >400 million people worldwide, incurring >$1 trillion in annual economic costs,
- Core symptoms, debilitating fatigue, cognitive dysfunction (“brain fog”), sleep disturbances, and post-exertional malaise (PEM) in 50–80% of cases, persist months to years’ post-infection, with a mechanistic overlap to ME/CFS,
➡️Core Mechanisms:
1. Immune Dysregulation:
- Persistent systemic inflammation features elevated cytokines (IL-6, TNF-α, IL-1β) detectable up to 14 months, driving T-cell exhaustion (reduced CD8+ IFN-γ/TNF-α production) and monocyte activation (COX-2, IL-8Rβ, CXCR6),
- Autoantibodies (anti-GPCR, anti-PITX2, anti-FBXO2, ANA/ENA) persist 12–14 months and correlate directly with fatigue, dyspnoea, palpitations, and cognitive impairment with molecular mimicry, gut dysbiosis and latent herpesvirus reactivation (EBV, HHV-6) amplifying autoimmunity,
2. Viral Persistence & Reactivation:
- SARSCoV2 RNA, spike protein, and antigens remain detectable in brain, muscle, gut and plasma up to 14–24 months in ~60% of cases, fuelling chronic low-grade inflammation,
- EBV/CMV reactivation signatures are common with spatial transcriptomics highlighted as a possible next tool to map tissue reservoirs,
3. Endothelial/Microvascular Pathology:
- Glycocalyx shedding (elevated SDC-1), capillary rarefaction and endothelin-1 elevation create a pro-thrombotic state,
- Platelet hyperactivation releases vWF/FVIII, forming anomalous fibrin(ogen) microclots that resist fibrinolysis and these circulate and fragment during exertion, causing hypoxia, ischaemia-reperfusion injury, and PEM,
4. Autonomic Dysfunction:
- Present in ~50% of patients (POTS predominant), driven by hypovolaemia (70%), small-fibre neuropathy (20–40%), vagus-nerve damage and microclot-induced compensatory tachycardia with 4-fold norepinephrine spikes,
5. Mitochondrial Impairment & Neuroinflammation:
- Skeletal-muscle biopsies show reduced respiration, cytochrome c oxidase activity and WASF3-mediated supercomplex disruption, producing rapid lactate rise and PEM within 48 h,
- Systemic cytokines breach the blood–brain barrier, sustaining microglial activation and cognitive sequelae,
➡️Diagnostic & Therapeutic Gaps:
- No validated biomarkers or subtype-specific criteria exist.
- Graded exercise is contraindicated.
- Observational promise exists for IVIg, low-dose naltrexone and apheresis, but large RCTs are urgently required.
➡️Future Priorities:
Calls for subtype-specific research, large-scale RCTs, advanced techniques (spatial transcriptomics, proteomics), and interdisciplinary collaboration to develop precision diagnostics and therapies.
‼️This exceptional review delivers a masterful, evidence-based roadmap that not only clarifies Long COVID’s complex pathophysiology but stimulates the scientific community toward urgently needed mechanistic breakthroughs and effective, patient-centred interventions.
‼️Bottom line: Long COVID is not a single disease but a complex, multisystem condition that can impact your life seriously!
#AvoidSars2 #AvoidReinfections
A huge thanks to all authors, @DrMark_Faghy@DavidJoffe64@PutrinoLab@DaniBeckman@resiapretorius@Sunny_Rae1 are only some of them!👏👏
https://t.co/cDL5dMpEoj